
記住我









Dactylitis is a typical lesion in psoriatic arthritis (PsA) and is associated with radiographic progression in chronic disease.
In early PsA, dactylitis is a common finding, but the associated impact of this lesion on the disease burden is unknown.
What does this study add?This study demonstrates that disease-modifying antirheumatic drug (DMARD)-naive patients with early PsA with dactylitis (dactylitic PsA) have a greater burden of disease than patients with PsA without dactylitis (non-dactylitic PsA), which was confirmed independently (ie, when dactylitis was excluded) demonstrating greater swollen joint count, C reactive protein, ultrasound (US) synovitis and US erosions.
Our data confirm that dactylitis is a clinical marker of a more severe phenotype in DMARD-naive early PsA.
How might this impact on clinical practice or future developments?In patients with early PsA, the presence of dactylitis identifies a more severe disease phenotype and may be an important discriminator for risk stratification in early arthritis clinics and clinical research trials.
IntroductionDactylitis is defined as diffuse swelling of a finger or toe and represents a specific lesion typically associated with psoriatic arthritis (PsA). The prevalence of dactylitis in PsA has been estimated at 33%–55%, with approximately 70% occurring at presentation.1 Dactylitis is the epitome of PsA pathophysiology, encompassing multiple underlying pathologies including inflammation to joints (synovitis) and tendons/ligaments (enthesitis). Flexor tenosynovitis, surrounding diffuse peritendinous inflammation and soft tissue oedema, are typically responsible for the ‘sausage digit’ appearance.2 Importantly, synovitis and bone erosion can develop, adding to further structural and functional impairments.3 Bone marrow oedema and ligamentous enthesitis have also been demonstrated using high-resolution MRI.4 At the bedside, the accuracy of ultrasound (US) for detecting inflammatory arthritis in PsA is regarded as comparable to MRI, with studies suggesting US may be superior for the assessment of synovitis.5
The presence or history of dactylitis adds high sensitivity and specificity towards classifying PsA (CASPAR criteria).6 Further, dactylitis is associated with greater radiographic damage in chronic established PsA.7 However, to our knowledge, direct evaluation of the impact of dactylitis on overall disease phenotype and severity in early, untreated PsA has not been characterised. The objective of this study was to determine the impact of dactylitis on clinical phenotype, US synovitis and erosion in disease-modifying antirheumatic drug (DMARD)-naive early PsA.
MethodsPatients, clinical details and examinationIn total, 177 DMARD-naive patients with early PsA meeting CASPAR criteria were recruited into the Leeds Spondyloarthropathy Register for Research and Observation for baseline cross-sectional analysis.6 Clinical examination included tender joint count (TJC) (78) and swollen joint count (SJC) (76). The early PsA cohort was dichotomised by the presence or absence of dactylitis at baseline (PsA with dactylitis (dactylitic PsA) or PsA without dactylitis (non-dactylitic PsA)). Dactylitis was recorded per digit via the dichotomous (Clegg et al) method including tender (‘hot’) or non-tender (‘cold’) status.8 9 Clinical enthesitis was measured by the Maastricht Ankylosing Spondylitis Enthesitis Score (MASES) to include peripheral and axial entheses.
US examinationExperienced ultrasonographers blinded to clinical details (four operators with over 5 years’ experience) scanned 50 joints per patient using the GE Logiq E9 machine with matrix linear (ML) 15–6 MHz or small-footprint linear array 18–8 MHz transducer and had regular training and calibration on the US examination protocol and quality of sonographic assessment throughout the study period, conducted every 6 months to maintain high consistency for US assessment, image interpretation and scoring.
SynovitisSynovitis was graded by semiquantitative scores (0–3) and defined as grey scale (GS) ≥2) or abnormal power Doppler (PD) signal (PD ≥1), and GS of ≤1 was determined as non-significant as it occurs frequently in healthy individuals.10
Wrists (radiocarpal, intercarpal and ulnar carpal recesses), metacarpophalangeal (MCP) joints 1–5, proximal interphalangeal (PIP) joints 1–5, distal interphalangeal joints 2–5, elbows, knees (suprapatellar, medial parapatellar and lateral parapatellar recesses), ankles (tibiotalar joint), subtalar joints, talonavicular joints and metatarsophalangeal (MTP) joints 1–5 were scanned in longitudinal and transverse planes (online supplemental table S1A).
ErosionsErosions were determined by periarticular cortical bone discontinuity present in two perpendicular planes (longitudinal and transverse), with MTP1 excluded as it is a frequent site of osteoarthritis.
EnthesitisEnthesitis was determined by the Outcome MEasures in Rheumatology (OMERACT)-defined elementary lesions and modified Glasgow Ultrasound Enthesitis Severity Score (GUESS), calculated per patient based on all the enthesitis sites and domains (except bursitis at the quadriceps tendon insertion—not recorded in the study protocol).11 12 The US data recorded for entheses are shown in online supplemental table S1 (B).
Statistical analysisStatistical tests were two-tailed, statistical significance prespecified at 5% (p<0.05) with 95% CIs. Differences between mean, medians and proportions were calculated using Student’s t-test, quantile regression (continuous variables), χ2 test (binary variables) and Kruskal-Wallis (categorical variables) via Stata V.16.1.
ResultsClinical characteristicsDactylitic PsA versus non-dactylitic PsADactylitic PsA occurred in 81/177 (46%) patients vs non-dactylitic PsA in 96/177 (54%) patients. Mean ages were similar; 43.7 and 44.4 years, respectively. More patients in the dactylitic group had a symptom duration of <24 months (68/81 (84%) vs 64/96 (66.7%), p=0.008). The median TJCs and SJC were significantly greater in patients with dactylitic PsA compared with patients without dactylitic PsA (TJC: 9 vs 4, p<0.01; SJC 7 vs 1, p<0.001), with polyarthritis being the predominant phenotype in dactylitic PsA (65.4%, p<0.01), while oligoarthritis was dominant in non-dactylitic PsA (86.5%, p<0.001). Excluding dactylitis affected digits, dactylitic PsA remained predominantly polyarticular (51/81 patients, 62.9%), and the SJC (but not the TJC) still significantly greater (total SJC: 326 joints (81 patients) vs 209 joints (96 patients), median 3 vs 1, p=0.002).
Clinical enthesitis was more prevalent in patients with dactylitic PsA (42/81 (51.9%) vs 34/96 (35.4%); p=0.027), with greater median MASES (1.0 (0.0–2.0) vs 0.0 (0.0–2.0); p<0.01). The prevalence of nail dystrophy did not differ between groups, however the median modified nail psoriasis severity index (mNAPSI) was greater in non-dactylitic PsA (2.0 (0.0–7.5) vs 0.0 (0.0–8.0); p<0.05).
Elevated C reactive protein (CRP >10 mg/L) occurred more frequently in dactylitic versus non-dactylic patients (44% vs 25% (p=0.006)) including with a greater median CRP and erythrocyte sedimentation rate (ESR; mm/hr) (CRP: 8.1 vs 5.0 (p<0.01), ESR: 16.5 vs 11 (p<0.05)). Disease Activity in Psoriatic Arthritis (DAPSA) scores were greater in dactylitic PsA but not significant (median 24.4 vs 20.8, p=0.07). No significant differences were observed in PsAQoL, HAQ, and DLQI. Comparison of patient characteristics between groups are shown in table 1.
Table 1Characteristics of the early PsA cohort dichotomised by the presence or absence of dactylitis
Characteristics of dactylitisOf 81/177 (45.8%) patients with dactylitic PsA, dactylitis affected 214 digits, predominantly with multiple digit involvement (>1) in 51/81 (63%) patients (median digits: 2 (IQR 1–3)) and was distributed asymmetrically (52/81 (64%) patients). Hands were affected in 23/81 (28.4%) patients, feet in 40/81 (49.4%), and both in 18/81 (22.2%). Dactylitis was more prevalent in toes (146/214, 68.2%) than fingers (68/214, 31.8%) with the majority of digits classified as hot dactylitis (179/214 digits, 83.6%) (cold dactylitis (35/214, 16.4%)). The second finger (23/179, 12.8%) and fourth toe (40/179; 22.3%) were most frequently affected by hot dactylitis, and the third finger (2/35; 5.7%) and fourth toe (10/35; 28.6%) by cold dactylitis (online supplemental figure S1A).
US synovitisIn total, 155/177 (87.5%) patients with PsA underwent ultrasonography (6143 joints): 69/155 (44.5%) patients with dactylitic PsA and 86/155 (55.5%) without dactylitic PsA (online supplemental figure S1B). US synovitis was significantly more prevalent in dactylitic PsA (GS ≥2: 23.6% vs 16.1% joints (p<0.001); PD ≥1: 7.3% vs 3.3% joints (p<0.001); GS ≥2+PD ≥1: 6.3% vs 2.6% joints (p<0.001)) as outlined in table 2A. GS ≥2 synovitis was most frequently observed at MCP 2–5, PIP1–3, MTP2–5, and PD ≥1 synovitis at MCP 2 and MTP 4–5. On exclusion of digits affected by dactylitis, US synovitis remained significantly more prevalent in patients with dactylitic PsA (GS ≥2: 21.3% vs 16.1% joints (p<0.001); PD ≥1: 5% vs 3.3% joints (p<0.001); GS ≥2+PD ≥1: 4.1% vs 2.6% joints (p<0.003); table 2B). Further subgroup analyses stratified for phenotype (defined by SJC ≥5 as polyarticular) confirmed greater GS ≥2 and PD ≥1 synovitis, respectively, for polyarticular subsets in dactylitic PsA (p<0.001), including greater GS ≥2 synovitis when dactylitis was excluded (p=0.01) (online supplemental table S2). Application of the second definition inclusive of tender joints (tender and/or swollen joints<5 as oligoarticular) indicated significantly greater GS of ≥2 and PD of ≥1 synovitis, respectively, independent of phenotype in dactylitic PsA. Exclusion of dactylitis from dactylitic PsA also confirmed greater GS of ≥2 synovitis in oligoarticular and polyarticular subsets independent of dactylitis affected joints (online supplemental table S3).
Table 2Ultrasound synovitis and bone erosions in non-dactylitic versus dactylitic PsA: (A) including dactylitis affected digits and (B) excluding dactylitis affected digits
US erosionsPeriarticular cortical bone erosions were identified in a significantly greater proportion of patients with dactylitic PsA, compared with those without dactylitis (20/69 (29.0%) vs 11/86 (12.8%), p=0.012). There was also a significant difference in the total number of erosions detected in dactylitic versus patients without dactylitic PsA (33/2557 joints vs 15/3206 joints, p<0.001; table 2A). The anatomical sites for joints most prone to erosive damage were MCP2 (9/33 (27.3%)) and MTP5 (11/33 (33.3%)).
On exclusion of dactylitic digits, US erosions were more frequent in dactylitic PsA than non-dactylitic PsA (24/2315 (1.1%) vs 15/3206 (0.5%) joints, p=0.008). The proportion of patients with US erosions (US erosion-positive patients) was greater for dactylitic PsA (18/69 (26.1%) vs 11/86 (12.8%) patients, p=0.035). Total erosion scores at the patient level were also higher in dactylitic PsA (p=0.016), including when dactylitis was excluded (p=0.048), as shown in table 2B. Subgroup analyses confirmed greater total US-detected erosions in polyarticular stratified subsets regardless of the phenotype definition applied and on excluding dactylitis affected joints (online supplemental table S2 and S3). The US appearances of erosions detected in the dactylitic PsA group are illustrated in figure 1B,D.
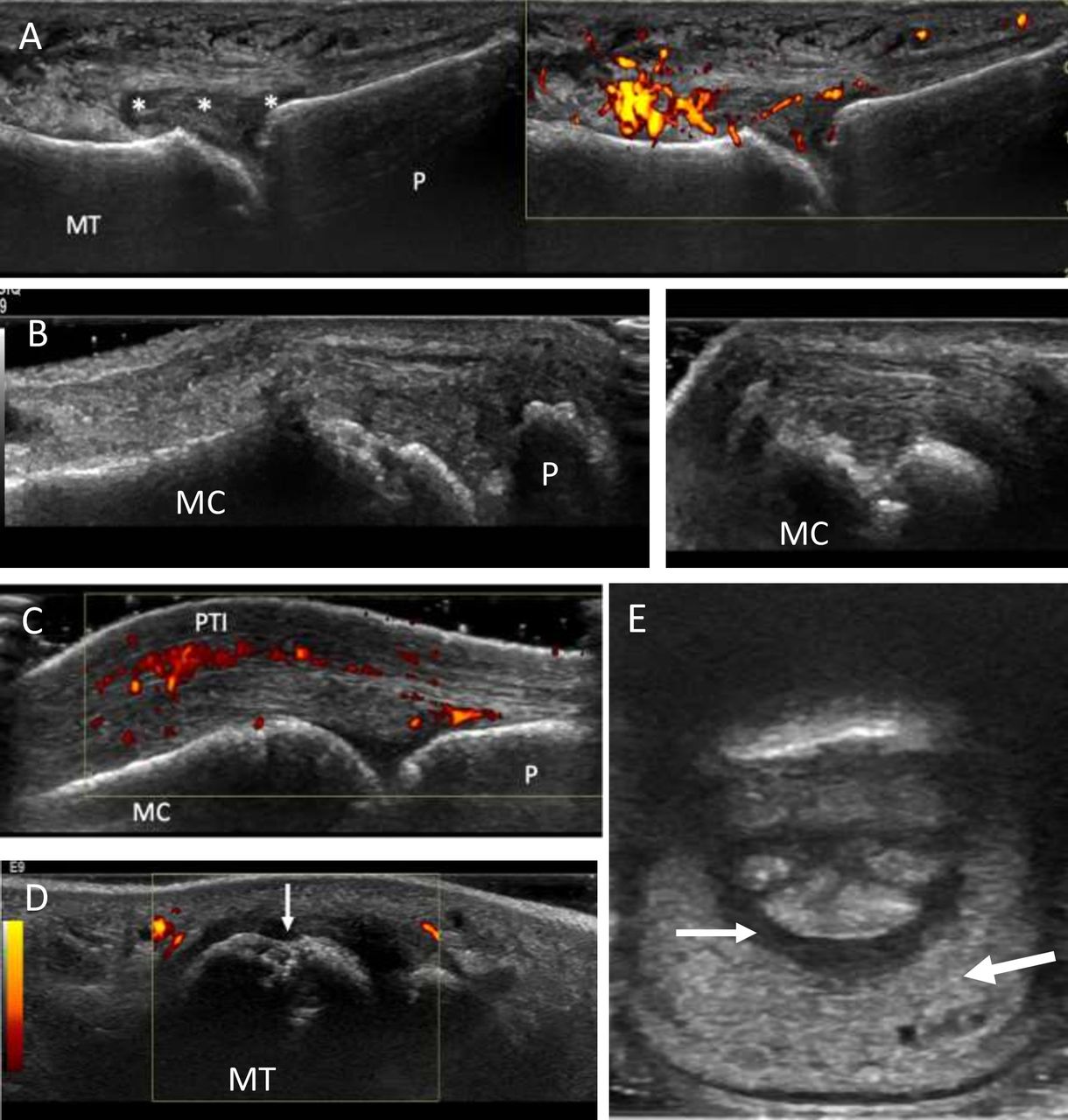 Figure 1
Figure 1 Characteristic ultrasound pathologies in early dactylitic patients with PsA. (A) Longitudinal view through the fifth metatarsophalangeal joint illustrating synovitis within a dactylitic toe. There is grey scale synovitis (grade 3) with effusion (*) and abnormal power Doppler signal (grade 2, right image) consistent with ‘active’ synovitis. (B) Periarticular cortical bone irregularity at the second MCP joint confirmed in the longitudinal (left) and transverse planes, respectively (right), confirming erosion. A common site of erosion in PsA and in dactylitis. (C) Longitudinal view at the MCP joint displaying power Doppler signal above the extensor tendon (PTI). (D) Image in the transverse plane showing the fifth metatarsal head, the most frequent site of erosion in feet, demonstrating periarticular bone irregularity (arrow). Bone irregularity was confirmed further in the longitudinal plane to signify erosion. There is also surrounding grey scale synovial hypertrophy (grade 2). (E) Transverse view of volar aspect of dactylitic third toe showing diffuse soft tissue oedema (large arrow) and flexor tenosynovitis (small arrow). MCP, metacarpophalangeal; MC, metacarpal head; MT, metatarsal head; P, phalanx; PsA, psoriatic arthritis; PTI, peritendon inflammation.
US in dactylitisIn digits affected by dactylitis, US synovitis (GS ≥2) was prevalent in 137/255 (53.7%) joints. A higher prevalence of US synovitis was observed in joints affected by hot dactylitis versus those with the cold type (129/227 (56.8%) vs 8/28 (28.6%) joints, p=0.0047). US PD synovitis (PD ≥1 regardless of GS grade) was present in 72/255 (28.2%) of the total joints clinically affected by dactylitis and was more prevalent in hot type (hot: 69/227 (30.4%) and cold: 3/28 (10.7%) joints, p=0.0289). In hot dactylitis, erosions occurred in 9/227 (2.6%) of affected joints (4/69 (6%) patients) and none in cold dactylitis (0/28) (p=0.388). Figure 1 illustrates synovitis at MTP5 (figure 1A) and shows soft tissue oedema and flexor tenosynovitis (figure 1E).
US enthesitisOf 1534 entheses examined by US, modified GUESS scores indicated no significant differences between patients with dactylitic PsA and patients without dactylitic PsA (median 3 (IQR 2–6) vs median 4 (IQR 1–6), p=0.91). There were no relevant differences between groups on analysis of OMERACT elementary lesions.
DiscussionThis is the first study, to our knowledge, to evaluate the overall clinical and US disease burden in a DMARD-naive early PsA cohort based on the presence/absence of dactylitis. These study results confirmed a greater burden of disease in PsA with dactylitis. Moreover, patients with dactylitic PsA had greater SJC, CRP, prevalence of US synovitis and erosive damage independently (ie, on exclusion of digits affected by dactylitis) compared with non-dactylitic PsA. These results therefore provide an insight into the significance of dactylitis in early PsA, demonstrating that it is an indicator of a more severe phenotype. Indeed, more aggressive disease accounted for an earlier diagnosis of patients with dactylitic PsA who presented with shorter disease duration. Further analyses to include history of dactylitis and exclude patients with a symptom duration of >24 months, respectively, did not change results confirming the increased burden of disease in the dactylitic group (online supplemental table S4 and S5).
Previous studies in established PsA have shown that digits affected by dactylitis are associated with significant pathological findings. Brockbank et al first reported that radiographic damage occurred frequently in hot dactylitis with an average PsA cohort disease duration of 8 years.7 Healy et al reported a high prevalence of synovitis in hot dactylitis present on MRI in 69%, closely matching the prevalence of US detected synovitis in our study (56.8%), confirming that synovitis is present in the majority of dactylitis in early PsA.13 Moreover, in our early PsA study, the greater prevalence of US synovitis and erosions in patients with dactylitic PsA (vs non-dactylitic PsA), even when excluding the dactylitis digits, has to our knowledge not previously been shown and reflects an increased burden of disease. Further, this was reflected by CRP, also a marker of disease activity which was elevated (>10 mg/L) more often in patients with dactylitic PsA (44.4% vs 25%, p=0.006) and with higher median values. This is a relevant observation, since elevated baseline CRP is associated with poor radiographic outcomes.14 Additionally, radiographic joint destruction is reportedly predicted by the development of dactylitis in men from longitudinal PsA cohort data.15 Despite the differences found for clinical enthesitis, a possible limitation of our study was the inability to show meaningful differences in US enthesopathy possibly related to the outcomes used or the known clinical and US mismatch shown in other stuides.16 However, our results do provide new data, including for US synovitis and erosion, showing that there is a difference in the burden of disease between patients with early PsA with and without dactylitis.
Tailoring therapy specific to PsA phenotypes is increasingly pertinent to avoid biologic disease-modifying antirheumatic drug (bDMARD) failure, especially given the diverse mode of action therapies available. Moreover, superior treatment responses have been shown for dactylitis with bDMARDs over conventional synthetic DMARDs, including first-line combination therapy.17 18 Our study findings can facilitate early risk stratification to optimise treatment outcomes, coherent with the European Alliance of Associations for Rheumatology (EULAR) recommendations that regard dactylitis as a poor prognostic factor in early PsA and advocate rapid initiation of DMARDs.19 Overall, these data may further inform management strategies, including clinical trials for targeted therapy to understand differential responses within PsA phenotypes.
ConclusionsThe presence of dactylitis is independently associated with an increased burden of disease with greater SJC, CRP, US-detected synovitis and erosive bone damage in DMARD-naive early PsA. Dactylitis should therefore be considered a clinical marker for a more severe phenotype in early PsA and may be an important discriminator for risk stratification in early intervention strategies.
Data availability statementData are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statementsPatient consent for publicationEthics approvalEthics approval was granted by the Leeds West Research Ethics Committee (ref: LG03/028) and written informed consent was received from all participants.
AcknowledgmentsThe authors thank the study sonographers, particularly Kate Smith and Borsha Sarkar. This report presents independent research supported by the National Institute for Health Research Leeds Biomedical Research Centre.
留言 (0)