It is well established that patients with isolated accidental hypothermia are at risk of cardiac arrest [1]. In England and Wales between 2013 and 2018 there were 330 deaths from ‘exposure to excessive natural cold’ (Office for National Statistics), whilst in the United States an average of 1301 deaths/year occurred between 1999 and 2011 [2]. The fundamental cause of death in hypothermia is the level of critical brain hypoxia. The fall in brain oxygen-consumption at lower core temperatures provides some resilience to low or no cardiac output states [1, 3, 4], but the brain cannot withstand hypothermic cardiac arrest indefinitely. It is therefore vital to try to maintain any ongoing cardiac output during initial patient management.
Hypothermic patients have a susceptibility to ‘rescue-collapse’. Traditionally described in water rescue, this sudden deterioration of the patient on initial management by first responders is frequently seen in the land environment [5,6,7]. The pathophysiology behind rescue-collapse is not entirely understood, but is likely a combination of ‘afterdrop’, catecholamine changes, and movement induced arrhythmias in an unstable myocardium [8,9,10,11,12,13,14,15,16]. Rapid stratification of risk of cardiac arrest in these patients would have two main benefits. Firstly, accidental hypothermia is often encountered in remote areas including backcountry environments, military operations/exercises, and expeditions; the ability to efficiently triage hypothermic patients and decide who can be managed in the field with low risk of cardiac arrest is invaluable in appropriate logistic asset allocation. Secondly, having an early appreciation of cardiac arrest risk can guide initial management decisions towards maintaining a perfusing rhythm.
Traditionally, methods to stratify the risk of cardiac arrest have been based on core temperature [1, 17,18,19]. In the pre-hospital environment, reliable measurements of core temperature are often not accessible. Infrared tympanic probes are generally considered unsuitable for field use because the sensors are not calibrated in low core temperature [20]. Low reading core temperature thermometers may not be in use and, when available, many have methodological issues. Rectal probes require exposure and handling of the patient possibly resulting in further drops in core temperature (thermoneutral temperature for an unclothed human is 28 °C) [21] and/or movement induced arrhythmias [15]. In addition, rectal temperatures can lag behind true core temperature by up to an hour during warming and cooling and it has been suggested they are unsuitable for monitoring afterdrop [20, 22, 23]. Epitympanic thermistor probes may give falsely low values in patients with unstable circulation and require both modification and validation for pre-hospital use [4, 20, 24,25,26]. Oesophageal probe temperature, when placed in the lower 1/3 of the oesophagus, closely correlates with pulmonary artery temperature and should be the gold standard in patients with a secured airway [9]. However this is usually only appropriate for patients with reductions in consciousness. These factors, combined with the requirement to make rapid early management decisions, support the necessity for a clinical assessment tool as an adjunct to the initial patient evaluation.
Given the increased likelihood of cardiac arrest with lower core temperature [21], the well-known Swiss-Staging Model of hypothermia uses vital signs at presentation to estimate core temperature (as a surrogate for cardiac arrest risk) from clinical indicators only (Table 1) [19].
Table 1 Swiss staging of hypothermia, Brown et al. 2012 [27]There are a number of issues with this assessment tool. Its ability to estimate core temperature has been shown to be unsatisfactory [18]. Shivering is a notoriously unreliable sign, continuing with a core temperature at least down to 28–30 °C [23, 28]. Many studies have described patients with a core temperature of below 24 °C with vital signs [7, 29,30,31]. For these reasons the Wilderness Medical Society guidelines on accidental hypothermia, 2014 & 2019, advise against relying on the Swiss-Staging system [21, 32]. This is further supported by the most recent adaption of the Swiss System by the International Commission for Mountain Emergency Medicine (ICAR MedCom) [33].
Hypothermia is a clinical continuum with much interpersonal variation. Stratifying the risk of cardiac arrest by estimating the patient’s core temperature from the presenting clinical picture is not plausible because of the variance in individual response to specific core temperatures. Instead, directly predicting cardiac arrest risk from clinical features is preferable.
A retrospective case report analysis from Pasquier et al., reviewing 183 cases of accidental hypothermia for concordance between traditional Swiss-Staging classification and measured core temperature, demonstrated that no patients in their subgroup analysis with a normal conscious level (defined as ‘HT1’) suffered cardiac arrest [18]. However, given that their primary endpoint was the correspondence between core temperature and Swiss-Stage, no further conclusions regarding the use of conscious level as the predictor were drawn. In addition, Frei et al. undertook a systematic literature review of witnessed cardiac arrest in hypothermia to assess for clinical characteristics and outcomes in this patient group [34]. Crucially, all of the patients who had their GCS recorded (n = 24) who arrested had a GCS < 11—this GCS was referred to as ‘Pre-Cardiac Arrest GCS’ with no further information on timing of this assessment given.
The initial hypotheses of this study are therefore:
1.
The risk of cardiac arrest is directly proportional to conscious level. Categorising hypothermia by level of consciousness is more appropriate and clinically repeatable for the management of hypothermic patients than traditional assessment by clinical estimation of core temperature.
2.
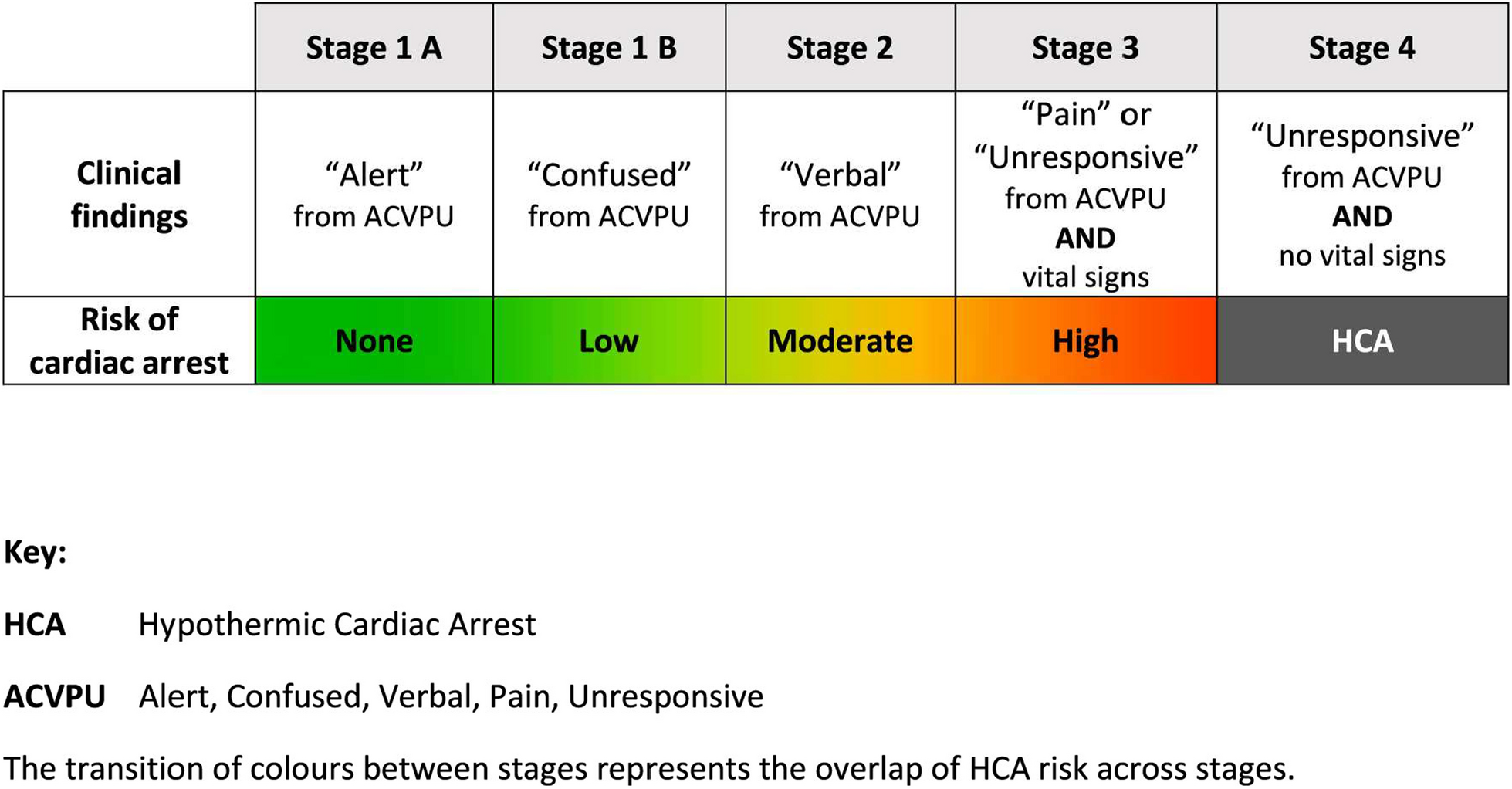
The following proposed novel clinical stages will more accurately predict the risk of cardiac arrest, making management decisions easier, clearer and safer than previous assessment tools:
3.
Cold stressed with no risk of cardiac arrest Patient Alert with normal cognition
4.
Hypothermia with low risk of cardiac arrest Patient alert but has signs of altered cognition
5.
Hypothermia with significant risk of cardiac arrest Patient has significant reductions in conscious level (V, P, U)
These hypotheses are partially supported by the recent ICAR MedCom ‘Revised Swiss-System’ [33]. This system applies a three point ordinal scale of ‘low’, ‘medium’, and ‘high’ risk of cardiac arrest based on conscious level as the primary element for staging, without attempt to quantify this risk further. The indirect argument presented is based on Pasquier et al’s study which demonstrates that haemodynamic and conscious level parameters correlate with core temperature, the latter showing the highest correlation (Spearman’s rho = 0.78) [35]. It is worth noting that this correlation is not the strongest, with a GCS of 5 being associated with a core temperature between 20 and 31 °C and a GCS as high as 14 being associated with a core temperature from 25 to 34 °C.
Testing the above hypotheses of this study aims to provide direct evidence for conscious level as an independent risk stratification tool in the initial assessment of patients with isolated accidental hypothermia. A retrospective case report analysis was conducted to look for correspondence between conscious level on arrival of medical support and cardiac arrest in the isolated accidental hypothermia patient group.




留言 (0)