In this study, we report that the provision of emergency anaesthesia is expedited by a pre-hospital RSI-capable team across three trauma networks in the south of England. The prompt provision of emergency anaesthesia in patients with major trauma, who have lost the capacity to independently maintain their airway or ventilate effectively is critical [9].
On average, time from emergency call to RSI was 64-min in the PHRSI group, compared to 84-min in the EDRSI group, highlighting a significant timesaving for the delivery of this time-critical intervention. This time is comparable to other rural settings [9]. A national standard is important to enable comprehensive audit and evaluation, with the overarching goal of ensuring equitable healthcare provision. However, the applicability of a national standard in regions characterised by nuances in critical care delivery, trauma network capabilities and geographical factors warrants scrutiny. Time from first contact with an RSI-capable team to delivery of RSI was shorter in those receiving EDRSI. This is likely influenced by complexities seen in the pre-hospital environment that aren’t experienced in the ED. Entrapment and scene safety are two elements unique to the pre-hospital environment which could influence this parameter and prolong on-scene time.
National data indicate a 25% adherence to the prescribed 45-min window for RSI with a median time of 55 (45–70) minutes, [9] which is like our own data. Further, other Air Ambulance Services acknowledge difficulties in meeting this target [16]. In the undifferentiated trauma patient, RSI is often not the definitive intervention needed and therefore time to RSI should not be a stand-alone target, unless the patient has significant airway compromise or ventilatory failure.
The three trauma systems within which our study took place span a mixed rural and urban area covering 7390 km2 which introduces considerable variability in incident locality. Travel times are further influenced by factors such as weather conditions, mode of transportation (helicopter or ground vehicle) and other operational considerations. Pre-hospital times more than 60-min to non-tertiary centres are not uncommon and inevitably lead to a subsequent secondary transfer facilitated by ground EMS, thereby incurring further delay. Our study reports a significantly longer conveyance interval for those patients receiving a PHRSI signalling they were further from hospital demonstrating the unique operational utility behind HEMS.
Our study evidences a potential unmet demand in the provision of early advanced airway management for major trauma patients. In this cohort of major trauma patients, around 50% required urgent advanced airway management on arrival to ED within 60 min. In keeping with UK major trauma demography, those identified as having emergent airway interventions were mostly male and had suffered blunt trauma with associated head injury, and a high injury severity [4]. Those patients who had an extended time to RSI were likely to be older and present with a higher GCS score, which on detailed interrogation is the case for the outliers seen in the PHRSI group. Local pre-hospital service provision models with variable case mix may benefit from geo-temporal analysis, to further understand access to pre-hospital RSI following major traumatic injury.
The evidence for the benefit of pre-hospital advanced interventions, including RSI, which prolong on-scene times, has been mixed and is debated [25]. A historic tenet of trauma care has been the ‘golden hour’, the first hour after injury where initial resuscitation and expedient transport are thought to have the most impact on patient outcome. Resultantly, time has been thought of as a predominant factor determining outcomes after trauma [25]. However, a 2015 systematic review of level III evidence by Harmsen, et al. [25] showed that in an undifferentiated trauma patient cohort, there may be a positive correlation between on-scene time and survival, as well as total pre-hospital time and survival. This was except for patients suffering traumatic brain injury and those who were hypotensive after penetrating trauma. Our study found no significant difference in mortality between EDRSI and PHRSI groups, however the latter group had significantly longer total pre-hospital times. These data likely reflect the advancements of pre-hospital care since the advent of the ‘golden hour’ and suggest that there is a cohort of patients who benefit from advanced pre-hospital interventions. However, the NAP-4 study provided warning of the disproportionately high reported rates of airway complications outside of operating theatres. Despite the time-saving advantage, the decision to undertake PHRSI should, therefore, be made after careful consideration of the additional pre-hospital related risks of adverse airway related events, compared with the benefits associated with a definitive airway and titratable ventilation. The additional time and resources that PHRSI requires should be considered case-by-case, particularly in circumstances with multiple high acuity patients.
Injury Severity Score was significantly higher in those receiving PHRSI, demonstrating the larger burden of disease in this group and this is comparable to previous studies [17]. However, there was no difference in mortality between our two groups, contrary to an expected increased mortality in patients with higher injury burden. The only identified randomised control trial comparing mortality after PHRSI and EDRSI also found no significant difference in mortality [18]. Observational studies have shown that even after adjusting for ISS and GCS score, there is no significant difference in mortality for those receiving PHRSI versus EDRSI [19]. Crewdson et al. (2017) suggest it is probable that provision of increasingly enhanced pre-hospital care, results in a higher proportion of critically ill patients reach hospital alive rather than having resuscitation efforts terminated in the pre-hospital setting [20]. This could be reflected by our finding of significantly longer length of critical care admission in those receiving PHRSI. Our study findings are encouraging and support the potential benefit of early, definitive airway management on-scene.
Overall time from call to emergency services to CT scan was similar in our cohort and a study by Haslam, et al. [10] who also found that the median time from initial call to CT scan was 120 min. Time from call to emergency services to CT scan was found to be slower in the PHRSI group compared to EDRSI. Time to CT scan might be considered a surrogate for time to treatment, which suggests patients who receive an PHRSI are waiting longer to receive definitive care. However, it has been previously recognised that patients attended by HEMS teams are frequently further away from hospital than those seen by ground ambulance clinicians [27]. This is a principal factor in determining whether a patient will be flown by HEMS or conveyed by ground ambulance [27] and would account for the extended conveyance intervals and time from emergency call to CT scan seen in our cohort. Incident location for EDRSI patients is not collected by TARN, therefore determining the mean distance from hospital to further contextualise the conveyance interval for each group, was not possible. Centralising major trauma care has been a primary aim of trauma networks in England and has been shown to improve trauma outcomes [2]. However, a continuing criticism is that patients suffering major trauma may need to be transported over longer distances to an MTC, often bypassing nearby hospitals. A pre-hospital RSI capable team thereby forms an important component in facilitating centralised care, by supporting the extra distance major trauma patients need to travel to receive specialist, centralised care.
Our regression analysis found that higher presenting GCS was associated with longer time to RSI. GCS is easy to use and reproducible, however it has been previously shown that severe TBI (defined as AIS head ≥ 3) is poorly predicted by GCS alone, with more than one-fifth of TBI patients presenting with GCS > 8 [21]. Head injuries in patients presenting with high initial GCS may be occult and difficult to recognise, contributing to the increase in time to RSI. Indication for RSI may only become apparent after subsequent decompensation of a head injured patient. Increasing age was found to increase the time to RSI in our study. It has been recognised previously that older trauma patients are often under-triaged in pre-hospital care and trauma triage tools are inadequate in accurately identifying the older trauma patient [22]. False reassurance from low-energy mechanisms are a contributor to this bias. As the average age of our population continues to rise, so too will the burden of older trauma on trauma systems. The relationship between age and time to RSI found in our study provides further justification for ongoing research into improving pre-hospital care and outcomes for the older trauma patient.
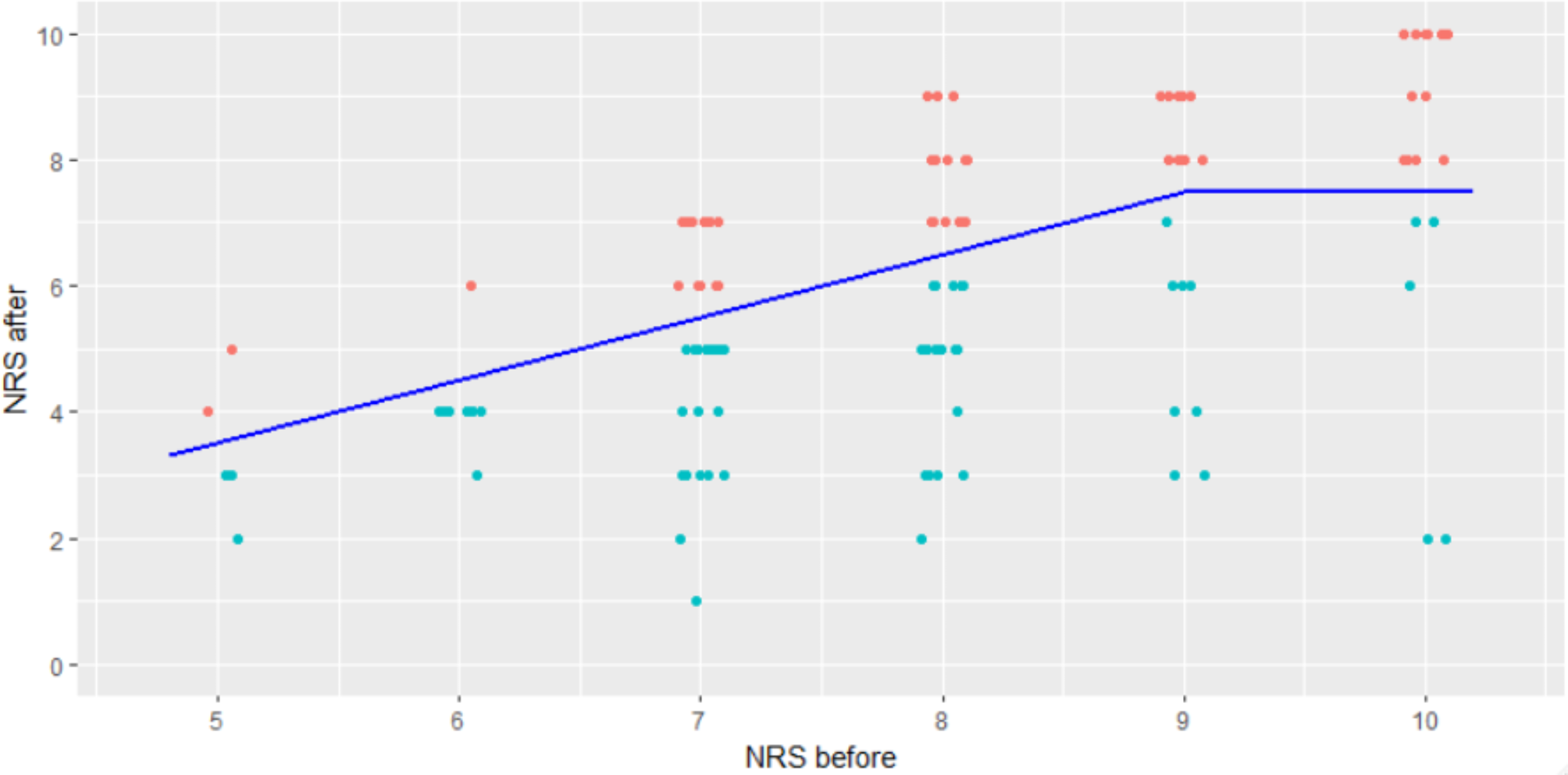
Inherent limitations of the study design mean that confounding factors cannot be removed. A proportion of patients who received EDRSI had time of arrival in ED stated as identical to their RSI time. There is certainly a cohort of patients who require emergent interventions upon arrival to the ED and prior to handover which could explain some of these cases. However, identical timings in this instance could represent information bias in the form of retrospective or absent data entry from receiving teams in the ED. Similarly, a large proportion of the initial sample were excluded. In addition, limitations in the dataset meant that regression analysis on additional variables could not be undertaken i.e. it is unclear what proportion of patients who had ‘urgent’ tracheal intubation in ED (within 60 min) could have been delayed or may have not met PHRSI criteria. However, a large proportion who had a presenting GCS ≤ 8 on hospital arrival which confirms that many were emergent. Investigation of individual encounters was undertaken in those patients for whom time intervals were prolonged and classed as outliers (Fig. 2). Of these patients, a majority were over 75 years old, suffered head injury and presented to ED with a GCS score ≥ 13. As mentioned above, we posit that presenting injuries in these patients may have been occult and not immediately obvious to presenting teams. The subsequent, delayed deterioration of intracranial injury and following RSI could explain the delayed time intervals of these patients.
Baseline characteristics in each cohort differed with regards to mechanism of injury and ISS, introducing selection bias to the analysis. This could be explained by HEMS dispatch criteria, which could withhold dispatch to less severely injured patients. Information on physiological parameters and adverse airway incidents of patients was not available for our cohort. This could also further explain time intervals, as resuscitation of a patient with severe shock could cause prolonged on-scene time. This is an important factor in determining the safety and effectiveness of delivering PHRSI, as increased rates of adverse events could change decision making in patients who are particularly sensitive to secondary insults, such as traumatic brain injury. The study population spanned across a mixed urban and rural area in the South-East of England, containing three trauma networks and three MTCs. Generalisability of our results to aeromedical services in different parts of the UK and worldwide may be limited by the relative density of specialist MTCs across our region. Widespread data collection across the UK may help to increase the generalisability of our results.




留言 (0)