The learning curve to attain surgical competency in robotic colorectal surgery
Introduction
The aim of the study was to assess the robotic colorectal surgery (RCS) learning curve of an experienced surgeon.
Methods
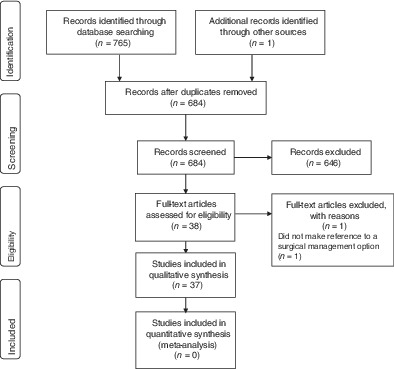
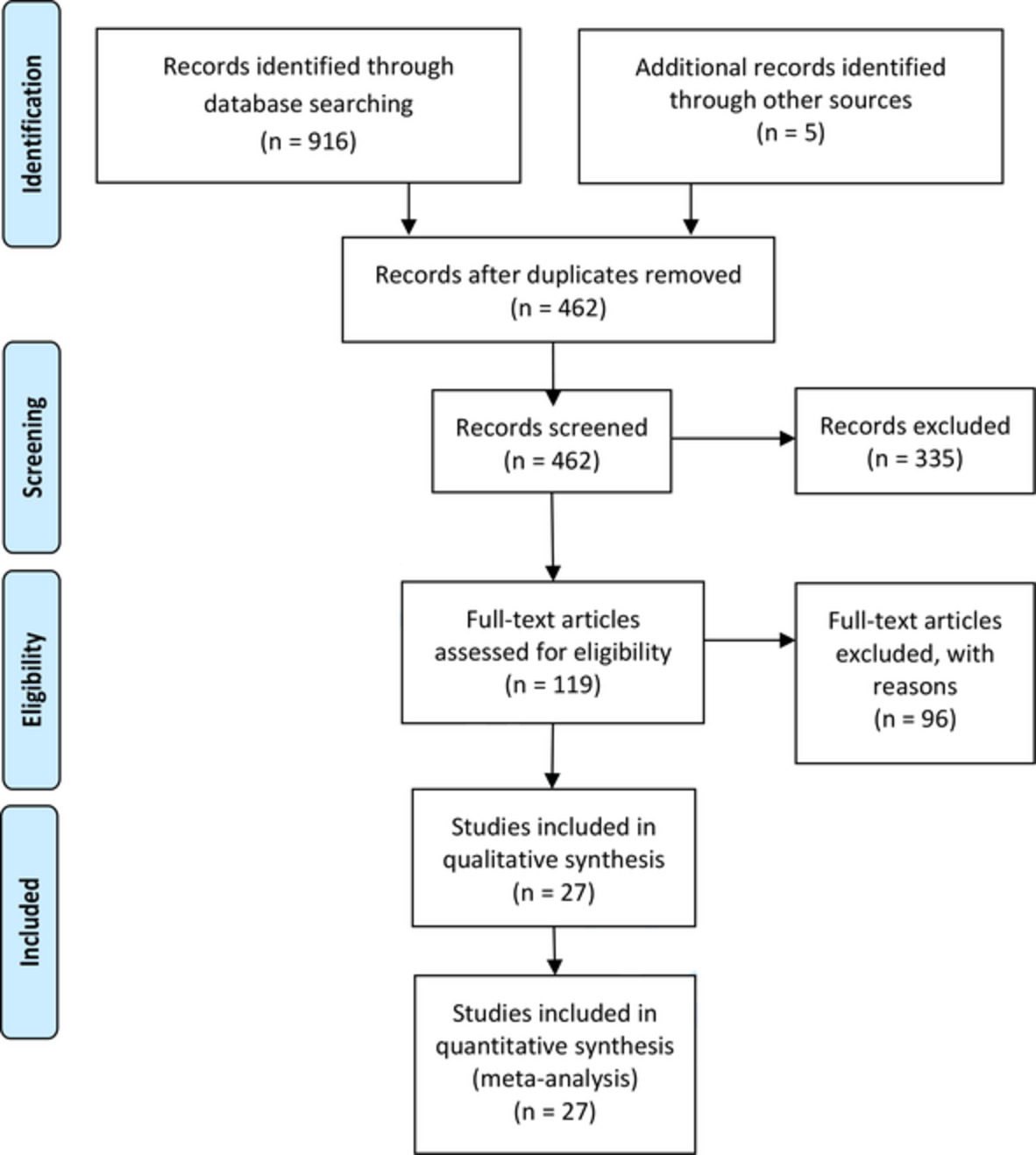
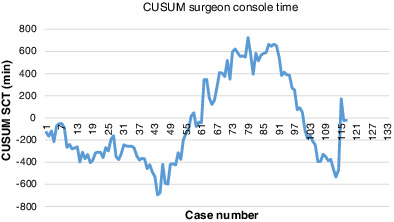
A retrospective review of 117 consecutive patients who underwent total RCS at a single institution between October 2018 and July 2021 was performed. Patient demographics, surgery indications, operation type, intraoperative data, histopathology, morbidity and mortality, and length of stay were analysed. Cumulative summation technique (CUSUM) was used to construct a learning curve of surgeon console and total operation times (SCT and TOT).
Results
There was no open conversion, positive resection margin and mortality in the study population. There were four Clavien-DIndo grade III complications and one local recurrence. The range for SCT was 18–855 min (mean 214, median 211) and TOT was 68–937 min (mean 302, median 291). The SCT CUSUM graph identified change in slope at cases 44 and 88, which divided the learning curve into three distinct phases. Patient demographics were similar through the three phases. There was proportionally more cancer cases performed in the first phase (P = 0.001). The mean SCT was significantly higher in Phase 2 when compared with Phases 1 and 3 (P = 0.03). The failure rate was similar through the three phases. There was a non-significant steady decline in LOS over the three phases, from 6.9 to 6.1 days.
Conclusion
Experienced colorectal surgeons can perform robotic surgery safely, even on patients with high complexity early in the learning curve. Audit of patient outcome should be an important component of learning curve assessment.



留言 (0)