
記住我





Splenosis is a benign condition that occurs after iatrogenic or traumatic splenic rupture. It is usually located within the abdominal or pelvic cavity and involves the visceral and parietal peritoneum.1 Splenosis is usually an incidental finding and is only addressed when causing symptoms.2 However, since malignancy cannot be ruled out through imaging, most patients go through an extensive diagnostic workup.3 The true incidence of splenosis is not well documented because it is usually found incidentally or at postmortem. The majority of patients present with minor symptoms, usually abdominal discomfort; however, severe symptoms such as gastrointestinal bleeding have been reported as well.4 Gastric splenosis is a rare presentation that can be misdiagnosed.5 Herein, we present a case of a gastric nodule mimicking a gastric gastrointestinal stromal tumor (GIST).
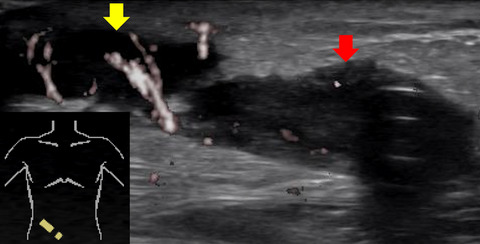
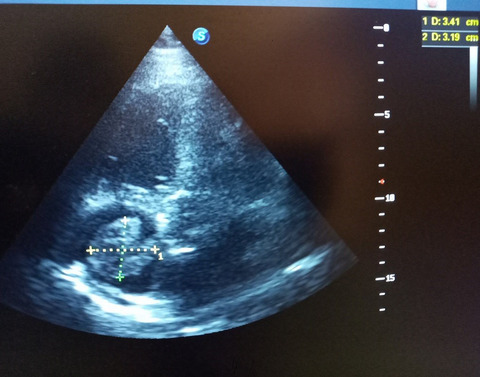
2 CASE SUMMARYA 29-year-old male patient presented with a history of multiple vomiting episodes. These episodes were taking place for the duration of the last year especially after excessive consumption of food. His surgical history included an open splenectomy 10 years ago due to traumatic splenic rupture after a fall. Apart from this operation, his medical history was clear. Upon admission from the emergency department and after the initial resuscitation, an abdominal ultrasound was performed showing a large mass in the lesser omentum in close proximity to the pylorus, measuring 3.3 × 3.2 cm. MRI scan was performed, and a round mass of 3 cm was reported with no clear evidence of it originating from an organ (Figure 1.1). The patient subsequently underwent an endoscopic ultrasound, which showed a hypoechoic nodule. Fine needle aspiration (FNA) was inconclusive (Figure 1.2). The differential diagnosis included gastric GIST and splenosis. In view of the presence of obstructive symptoms and the inability to exclude malignancy, surgical resection was offered. Laparoscopic surgical resection was performed 48 h after admission. The mass was found to be severely adherent to the stomach and the liver, and its blood supply was derived from the surrounding tissues. The mass was removed (Figure 2), and postoperative course was uneventful. The patient was discharged on the second postoperative day and reported instant relief of his symptoms. The pathology report revealed a rounded encapsulated accumulation of splenic tissue, 3.5 cm in size, consistent with the diagnosis of splenosis (Figure 3).

Preoperative abdominal MRI tomography scan showing a mass of 3.7 cm (1) and endoscopic ultrasonography (2) shows a submural low echohomogenous mass with close proximity to the left hepatic lobe measuring 3.7 × 3.4

Surgical specimen measuring 3.3 cm

Pathologic examination. Presence of splenic tissue confirmed the diagnosis of splenosis
3 DISCUSSIONEctopic splenic tissue can be found in two forms: accessory spleen and splenosis.2 Accessory spleens are congenital and arise from the left side of the dorsal mesogastrium during the embryological period of development. Splenosis, on the contrary, is an acquired condition that results from autotransplantation of viable splenic tissue in different anatomic sites of the body. This condition occurs after traumatic or iatrogenic rupture of the spleen.3 An accessory spleen is characterized by normal splenic histology with its blood supply uniformly arising from the splenic artery. However, the blood supply in splenosis derives from the surrounding tissues and vessels depending on the location of the splenic tissue, without any association to the splenic artery.2 This characteristic allows the distinction of the two entities. Recent publications have reported a 67% possibility of splenosis in patients with a history of splenic injury and surgery.6, 7 Most of the patients are asymptomatic and present with slight abdominal discomfort.3 Patients’ symptoms depend on the anatomic location of the ectopic splenic tissue. The majority of the patients have splenosis of the abdominal cavity, including the liver, the adrenal glands, the greater omentum, and the mesentery.2 The pelvic cavity, subcutaneous tissue, and other organs may also be involved.8 Splenosis can cause specific clinical symptoms according to its location. There have been reported cases of gastroenterological splenosis leading to gastrointestinal bleeding,4 multiple splenosis nodules in the abdominal cavity causing intestinal adhesions and acute intestinal obstruction.9
In this case, we present a case of gastric splenosis mimicking a gastrointestinal stromal tumor causing intestinal obstructive symptoms. Our patient had a history of splenic injury and underwent splenectomy. He was admitted to our hospital with multiple vomiting episodes after heavy meals and received an upper endoscopy, an MRI, and an endoscopic ultrasonography examination. The findings were inconclusive as the manifestations of splenosis and GIST are similar. The tests showed a smooth round mass, with homogeneous low echo, which seemed to derive from the muscularis propria of the stomach. At that point, the diagnosis of splenosis was considered along with the diagnosis of GIST. The possibility of a more extensive workup with Tc-99 m-labeled heat-denatured red blood cells (Tc-99 m-DRBC) and FNB in order to exclude the possibility of malignancy was discussed with the patient. However, the patient did not want any further investigation performed and specifically requested to proceed with surgery in order to be relieved of the obstructive symptoms. The patient underwent laparoscopic surgical excision of the mass and had an uneventful recovery.
Regarding patients with a history of splenic injury or surgery, with a parenchymal mass in the abdominal cavity, the diagnosis of splenosis should always be considered. Following CT scan, the density of splenosis is similar to normal splenic tissue,10 except from the arterial phase of the imaging where the normal spleen tissue is unevenly contrast enhanced, in contrast to the homogeneous enhancement of splenosis.2 The ultrasonic inspection, computed tomography, and magnetic resonance imaging have limited value in diagnosing splenosis. FNA is usually unable to distinguish splenosis from a lymphoproliferative disease and is usually inconclusive.9 FNB can provide a more definitive diagnosis. CD8 immunostaining of cell block or core biopsy material highlights unique splenic endothelial cells and confirms the diagnosis of splenosis.11 This marker has been reported to provide the diagnosis of accessory spleen in the pancreas thru EUS-guided FNA in a limited series of patients.12
Another sensitive method to diagnose splenosis is scintigraphy with sensitive technetium-99 m-labeled heat-denatured red blood cells (Tc-99 m-DRBC); this is the most specific and efficient diagnostic method for splenosis.14 Except for Tc-99 m-DRBC and FNB, the rest of the aforementioned examinations have little to offer in diagnosing splenosis. Only combining the medical history of the patient, imaging examination and radioisotope scanning the diagnosis can be made with some surety. The diagnosis of splenosis in asymptomatic patients does not require surgical resection and can be treated without any intervention. However, most of the cases with splenosis that have been reported were treated invasively, including biopsy and surgical resection. Splenosis may be beneficial in patients who have undergone splenectomy, since it can replace part of the immunologic function of the removed spleen.15 Hence, conservative treatment is strongly recommended for asymptomatic splenosis, except for certain occasions, such as in idiopathic thrombocytopenic purpura and Felty syndrome. However, if splenosis causes acute intestinal obstruction, gastrointestinal hemorrhage, or it cannot be distinguished from an abdominal malignant tumor, surgery is required.13 The inter-operative frozen section pathological examination is the gold standard for the diagnosis of splenosis. The surgeon should avoid excessively wide excision, in order to avoid damage to healthy tissue.9
4 CONCLUSIONSplenosis should be included in the differential diagnosis in patients with incidental findings of an abdominal lesion and prior history of splenectomy. EUS-guided biopsy and Tc-99 m-DRBC can lead to a definitive diagnosis, which may alter the management plan, since asymptomatic patients do not need surgical intervention or surveillance and seem to benefit from the functional ectopic splenic tissue in the absence of spleen. In cases of intestinal obstruction, hemorrhage, or difficulties in the medical differentiation, surgical excision can provide a definitive diagnosis and solution.
CONFLICT OF INTERESTThe authors declare that they have no competing interests.
AUTHOR CONTRIBUTIONSAP, AR, DT, and DK have contributed to drafting the manuscript. E.S. contributed to the pathology report. AP is the senior author of the study who conceived the study and edited the manuscript.
CONSENTWritten informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
留言 (0)