
記住我





The word teratoma is derived from the Greek word “teratos,” which means a monster. The most common benign lesion in young women is a mature cystic teratoma. Malignant transformation is rare and seen in less than 3% of the cases.1 The chances of malignant transformation increase with age and are most common in post-menopausal women of the 4th to 5th decade.2 Mature cystic teratoma of the ovary (MCTO) can transform into squamous cell carcinoma, adenocarcinoma, and papillary carcinoma, of which squamous cell carcinoma being the most common. Previous studies have shown a poor prognosis for the malignant transformation of MCTO.3 It is nearly impossible to diagnose the malignant transformation of MCTO preoperatively due to the tumor's rarity and its similarity to MCTO.4
Furthermore, due to the condition's rarity, no standard treatment has been established for its management yet. There are several studies of malignant transformation of MCTO; however, undifferentiated carcinoma arising in the MCTO is exceedingly rare. Here, we present a rare case of undifferentiated carcinoma arising from MCTO.
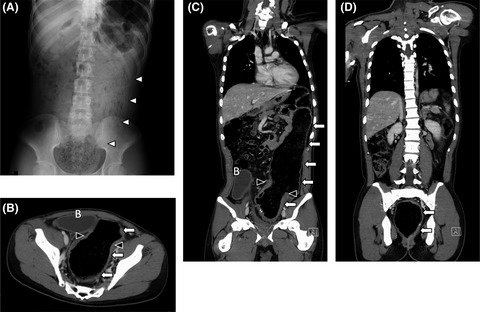
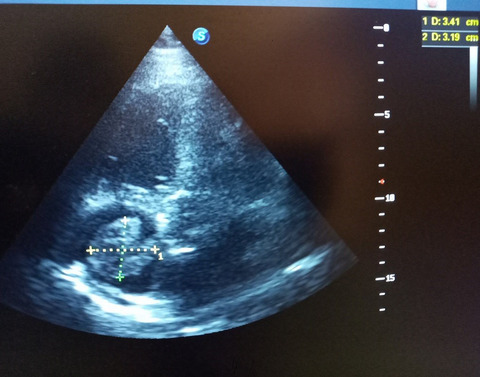
2 CASE REPORTAn 80-year-old multiparous woman presented with complaints of lower abdominal pain and back pain for 2 weeks. There was no history of weight loss and loss of appetite. Bowel and bladder habits were normal. There was no other significant clinical or family history. On abdominal examination, she had mild tenderness at the left iliac region. Per vaginal examination showed mild cervical erosion and a hard palpable mass in left adnexa and the Pouch of Douglas. Abdominal ultrasound revealed a complex adnexal cyst measuring 5.3 × 5.0 × 9.7 cm adjacent to the fundus of the uterus, likely originating from the right adnexa. The cyst had thick walls with polypoid projections and mural nodules measuring up to 15 mm in thickness. Serum CA 125 and CEA were 200 IU/ml and 63.62 IU/ml, respectively. A computerized tomography scan of the abdomen and pelvis revealed a 10 × 6 × 6 cm cystic lesion in the pelvis anterosuperior to the uterus. Multiple enlarged para-aortic lymph nodes measuring 20 × 14 mm, a few sub-centimeter-sized left external, and common iliac lymph nodes were noted. A suspicious enhancing nodule was also noted in the Pouch of Douglas. A presumptive diagnosis of advanced ovarian cancer was made. The patient underwent total abdominal hysterectomy with bilateral salpingo-oophorectomy with bilateral pelvic lymph node dissection, para-aortic lymph node dissection, total omentectomy, appendectomy, bladder peritoneal deposit removal with left Double-J stenting. Peroperative specimen shows large bosselated appearance of the left ovarian mass with intact capsule. Figure 1A, B).

1(A) Peroperative specimen of left ovarian mass having bosselated appearance and venous congestion. (B) Specimen of left ovarian mass with an intact capsule
2.1 HistopathologyOn gross examination, a left ovarian mass measuring 11 × 7.5 × 5.5 cm in diameter was identified. Cut section revealed solid and cystic areas containing thick pultaceous material. A microscopic examination from left ovarian mass showed histomorphological features of undifferentiated carcinoma (Figure 2A) and squamous cell carcinoma (Figure 3A, B) arising from mature cystic teratoma pT3N1b (FIGO stage III B). Ovarian surface involvement was not identified. Tumor deposits were noted on the serosal aspect of the left fallopian tube and bladder. Sections from the uterus, contralateral ovary, right fallopian tube, omentum, appendix, and right pelvic peritoneum showed no involvement by carcinoma. Peritoneal fluid cytology was negative for malignant cells. Out of 24 lymph nodes, three lymph nodes were involved by tumor deposit.

Histological section showing sheets of undifferentiated cells with frequent mitotic figures (A). On immunohistochemistry, undifferentiated cells are positive for CK AE1/AE3 (B) and negative for synaptophysin (C) and SALL4 (D)

Histological section shows infiltrating atypical squamoid cells in nests and clusters. (A) Keratin pearl and dyskeratotic cells noted. (B)
2.2 ImmunohistochemistryUndifferentiated tumor cells showed the following immunohistochemistry: CK (Cytokeratin): Positive (Figure 2B), P40 (marker to distinguish squamous cell carcinoma from adenocarcinoma): Negative, SALL 4 (transcription factor associated with embryonic cell pluripotency): Negative (Figure 2D), Synaptophysin: Negative (Figure 2C), Vimentin: Negative, and Desmin: Negative.
Squamous differentiated tumor area showed the following immunohistochemistry: CK: Positive (Figure 2B), P 40: Positive (Figure 4), SALL4: Negative, and Synaptophysin: Negative. The Ki67 (a marker of cell proliferation) index was 45%–50%.

Tumor cells exhibiting squamous differentiation show nuclear positivity for p40 on immunohistochemistry
After the cumulative information from clinical, radiological, histomorphological, and immunohistochemical studies, the diagnosis of undifferentiated carcinoma and squamous cell carcinoma arising in the background of MCTO was made. The patient was discharged without any postoperative complications. The patient is under adjuvant chemotherapy with Paclitaxel and carboplatin once a three-weekly cycle. She is tolerating the chemotherapy well and is stable without any complaints at two months of follow-up.
3 DISCUSSIONCystic teratoma is a common benign tumor found in 10%–20% of women in their lifetime.5 However, in rare cases, it might transform into a malignant form. The most common malignant transformation is squamous cell carcinoma with an incidence of around 0.2%–0.8%.6 We here discuss a case of the 80-year-old woman where mature cystic teratoma has been transformed into undifferentiated carcinoma.
Any of the three germ layers—ectoderm, mesoderm, and endoderm—can be the point of development of ovarian teratoma.7 So, malignant transformation may occur from any of the three germ layers into different histological tumor types such as adenocarcinoma, squamous cell carcinoma, melanoma, sarcoma, and adenosquamous carcinoma. The most common malignant transformation from MCT is squamous cell carcinoma, which is around 80% of all the cases of transformations.8
Clinically, the patient with cystic teratoma usually presents with an increase in abdominal girth, abdominal pain, abdominal distension, or palpable pelvic or abdominal mass. Sometimes, the patient remains asymptomatic until the complication occurs. The most common complications are ovarian torsion, rupture of the peritoneum, and invasion of the adjacent structures.9 The gastrointestinal or urinary symptoms may arise if the tumor has invaded the adjacent organs in the pelvic cavity.10 In our case, the patient presented with lower abdominal pain for two weeks and mild tenderness in the left iliac region on physical examination.
Preoperative identification of the malignant transformation of the mature cystic teratoma is difficult. Only 1%–2% of the SCC cases can be diagnosed preoperatively.10 Multiple criteria have been proposed to identify it. The criteria such as age greater than 55, large tumor size >10 cm, and radiological signs within revascularization are most likely to represent the malignant transformation of the cystic teratoma.11 So, CT scan and MRI are essential in identifying the preoperative malignant transformation with the features such as necrosis, cystic wall growth, invasion to adjacent peritoneal organs, or metastasis to the pelvic organs.12
Histologically, the undifferentiated tumor may show mesenchymal and epithelial differentiation features and may show the immune reactivity for markers such as cytokeratin, vimentin, and epithelial membrane antigen.13 In the present case, the undifferentiated area of the tumor exhibited round to oval cells and did not take immunohistochemical reagents such as P40, SALL 4, synaptophysin, desmin, <>vimentin, and CD20 except for cytokeratin. So, we consider our tumor to be an undifferentiated type with features of epithelial differentiation. However, cytokeratin and P40 were positive in the squamoid differentiated areas of carcinoma. Therefore, considering the histomorphological features and immunohistochemical findings, a final diagnosis of malignant transformation of MCT into undifferentiated carcinoma and squamous cell carcinoma was made.
The malignant transformation may be associated with the HPV infection or due to the alternation in the tumor suppressor gene such as p53 and p16.5, 14 The malignant transformation usually has an association with the level of tumor markers. Therefore, the tumor markers such as SCC antigen, CA125, CA19-9, and CEA are likely to be increased in patients with this transformation. However, the FIGO stage and tumor size do not determine the level of these markers. In our case, the level of serum CA125 was 200 IU/ml, and CEA was 63.62 µg/L.10
The standard treatment of malignant transformation of MCTO is radical surgery and chemotherapy. There is no fixed protocol for optimal adjuvant therapy due to the rarity of the disease. Surgical treatment is usually performed by hysterectomy with bilateral salpingo-oophorectomy, omentectomy, peritoneal biopsy, and para-aortic lymph node dissection. For chemotherapy, a wide range of therapeutic agents such as anthracyclines, alkylating agents, antimetabolites, platinum agents, and vinca alkaloids are used.12 Some scholars report the combination of paclitaxel with alkylating agents will improve the survival of the patients with this transformation.5 In the present case, the patient underwent surgical treatment and adjuvant chemotherapy with paclitaxel and carboplatin thrice weekly (L1Cl completed).
The prognosis of the malignant transformation depends on factors such as age >55 years, large tumor size, high cancer grade, and advanced stage of the disease. The cytoreductive surgery in combination with chemotherapy is likely to improve the prognosis.12
4 CONCLUSIONMalignant transformation of mature cystic teratoma into undifferentiated carcinoma is rare. Post-menopausal women presenting with giant tumors must raise suspicion for malignancy since preoperative diagnosis is often impossible. An intraoperative diagnosis aids in the diagnosis and determine the extent of surgical treatment. Immunohistochemistry can help differentiate the type of carcinoma, which can further determine the treatment and prognosis. There are no fixed guidelines for treating malignant transformation of MCTO; surgery followed by chemotherapy is usually the standard of treatment. Diagnosis in the early stages improves survival. Hence, early detection and proper evaluation of the type of carcinoma can affect survival.
ACKNOWLEDGEMENTWe gratefully acknowledge the work of members of our hospital and the patient.
CONFLICT OF INTERESTThe authors declare that there is no potential conflict of interest with respect to the research, authorship, and /or publication of this article.
AUTHOR CONTRIBUTIONSVA, RM, and AM collected the required case information, images, slides, reports, and contributed to writing manuscripts. HPD and MS examined and interpreted the pathology. AB was involved in the description of the case, counseling, and treatment of the patient. VA, RM, AM, AB, MS, and HPD reviewed the literature and contributed to writing and editing the manuscript. All authors read and approved the final manuscript.
ETHICAL APPROVALThe hospital research board (HRB) of Nepal Cancer Hospital and Research Center, Harisiddhi, Lalitpur, Nepal, provided approval.
CONSENTWritten informed consent was obtained from the patient before the submission of the report. The signed institutional consent form is on file.
留言 (0)