
記住我

High-frequency oscillations (HFOs), subdivided into ripples (80–250 Hz) and fast ripples (FRs; 250–500 Hz), are a promising biomarker for epileptogenic tissue. Most studies have reported results at the group level, with higher HFO rates in epileptogenic than nonepileptogenic tissue, and a better correlation between favorable outcome and removal of tissue generating HFOs than removal of tissue generating interictal spikes or that is part of the seizure onset zone (SOZ).1-3 FRs recorded after resection have been linked to seizure recurrence.4-7
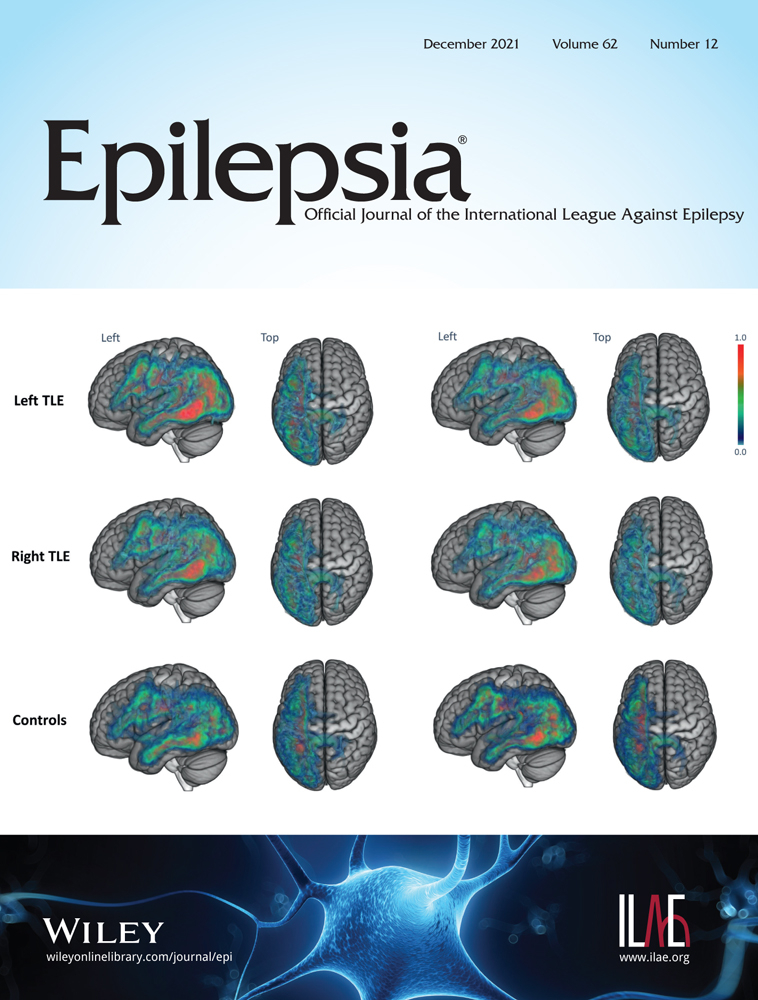
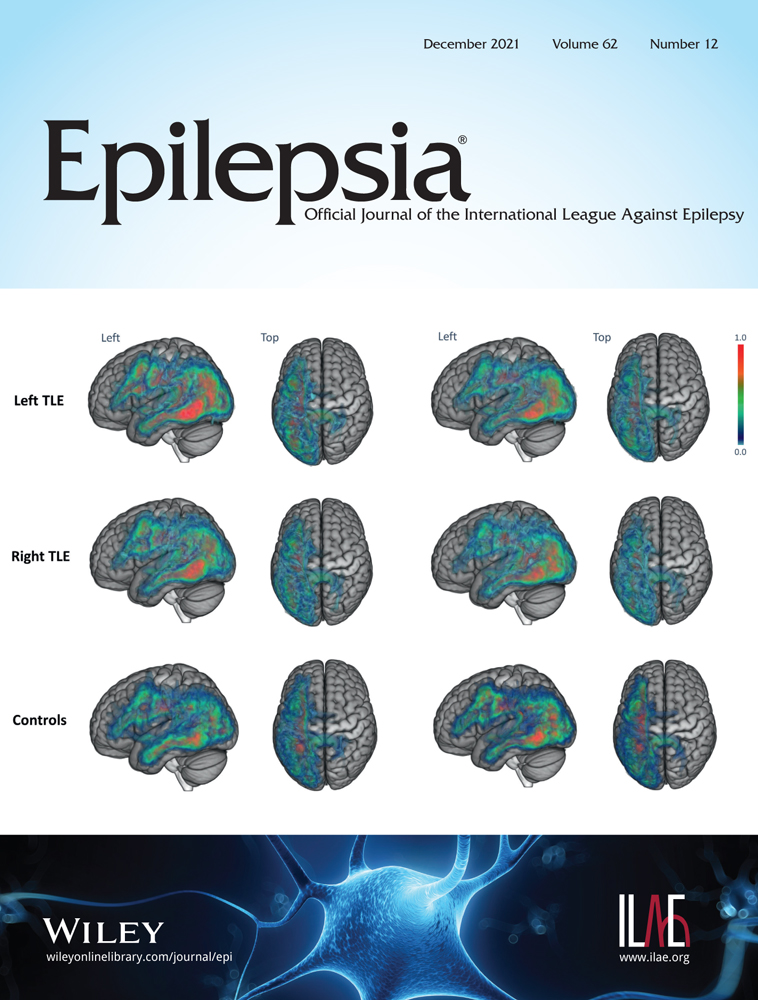
Prospective studies reported conflicting results on the performance of HFOs to identify the SOZ and predict good outcome at the individual patient level.8-10 They showed patient examples where the performance of ripples was hindered by the detection of presumably physiological ripples.8, 10 That HFOs occur under physiological conditions is a challenge when assessing their validity as a biomarker for epilepsy. Physiological HFOs occur predominantly in the ripple range, at rest and linked to cognitive processes or evoked by tasks or stimuli.11-19 Pathological and physiological HFOs largely overlap in their signal properties, and there is no reliable way to separate them.17, 20, 21 The Montreal Neurological Institute (MNI) Open iEEG Atlas project (https://mni-open-ieegatlas.research.mcgill.ca/)22, 23 studied HFOs in carefully selected stereoelectroencephalographic (SEEG) channels with normal electroencephalographic (EEG) activity.24 The rate of physiological ripples varied substantially across different regions, with the highest values in the occipital, sensorimotor, and mesiotemporal regions. Physiological FRs were rare, even in eloquent cortical areas.
This study evaluated whether "correcting" for physiological HFOs improves identification of the epileptic focus and prediction of surgical outcome. We hypothesized that using the statistical distribution of normative physiological HFO rates for each region to define rates that are too high for the physiological range, and therefore most likely to be pathological, would increase the performance of this marker. We expected the improvement to be most pronounced in patients with a focus in or close to brain areas generating high rates of physiological ripples. Because physiological FRs are rare, we expected no improvement for FRs.
2 MATERIALS AND METHODS 2.1 Patient selection and data acquisitionWe screened 202 consecutive patients undergoing SEEG investigation followed by resective open epilepsy surgery at Grenoble-Alpes University Hospital (CHUGA) or the MNI between January 2009 and January 2019. For selection criteria and flowchart of patients' inclusion see Figure 1. This study was approved by the MNI Institutional Review Board. All patients signed written informed consent.

Flowchart of the patient selection process. The reasons for exclusion merged in others are no report available (n = 3), no visible interictal electroencephalographic changes at seizure onset (n = 1), and premature termination of stereoelectroencephalogram (SEEG) due to self-removal of electrodes (n = 1). In nine of the 151 included patients, we could only select 20 min of non-rapid eye movement (NREM) sleep containing one or more electrographic seizure. In five, we could only select 20 min of NREM sleep <2 h away from a focal seizure. In one other patient, we could only select 10 min of NREM sleep. We decided to include these patients to be as generalizable as possible. The segments with seizures themselves were excluded. CHUGA, Grenoble-Alpes University Hospital; MNI, Montreal Neurological Institute
The MNI recordings were acquired with Harmonie (Stellate) or Nihon-Kohden EEG amplifiers at a sampling rate of 2000 Hz, using homemade MNI or commercial DIXI electrodes. The CHUGA recordings were acquired with Micromed EEG amplifiers at sampling rates of 512, 1024, or 2048 Hz, using DIXI or, in a few occasions, ALCIS electrodes.
2.2 Data selection and HFO analysisAnalogous to the MNI Open iEEG Atlas, we automatically detected HFOs in visually selected 20-min sections from non-rapid eye movement (NREM) sleep stages N2/N3,24 as this state shows the highest HFO rates25-27 and best identifies the epileptic focus in the interictal EEG.28 If possible, we chose epochs in the first sleep cycle, because it was shown to contain higher pathological HFO rates.29 We selected epochs ≥2 h away from focal or 6 h from generalized seizures. Ripples (80–250 Hz) were analyzed in all subjects. FRs (>250 Hz) were analyzed in subjects whose recordings had a sampling frequency greater than 1000 Hz. The detector is available at https://mni-open-ieegatlas.research.mcgill.ca/.12, 29, 30 It identifies increases in power with respect to the background in narrow frequency bands, with a duration longer than four oscillations plus the effective response time of the filters (equiripple finite impulse response filters of order 508). Results of HFO analysis were not used for clinical decision-making.
2.3 Image coregistration and localization of electrode contactsRegistration to stereotaxic space and anatomical localization of electrode contacts and channels were performed as done previously.22-24 Using MINC tools (http://www.bic.mni.mcgill.ca/ServicesSoftware/MINC) and the IBIS platform, patient-specific peri-implantation and postsurgical images were linearly registered to the preimplantation magnetic resonance imaging (MRI), and electrode positions were marked in the coregistered images. A nonlinear transformation from the preimplantation image to the ICBM152 2009c template was obtained and applied to the coordinates to represent them in the common MNI stereotaxic space. We used the same 17 regions as the MNI Open iEEG Atlas to correct for region-specific physiological HFO rates.24
2.4 Classification of channelsA bipolar channel was classified as resected if both contacts were resected on the coregistered postresection image. To account for sagging, coregistration error, and partial contact resection, contacts in or in the close vicinity (<5 mm) of the cavity were considered resected.28, 31 SOZ channels were identified by consensus of two neurophysiologists based on the first unequivocal visible signal changes at seizure onset independent of frequency content.32
To determine where each bipolar channel was recording from, we modeled each contact as a sphere of 10-mm radius and computed the percentage of each Atlas' gray matter region within this volume, assigning weights that decreased with the square of the distance from the center. We then averaged the percentages over the two contacts, and used up to three regions showing the highest percentages.
2.5 ThresholdsWe compared two thresholds for automatic HFO detection frequently used in the literature with three thresholds based on the normative values of the MNI Open iEEG Atlas.24 Studies in the literature frequently use (1) HFO rate > 1/min5-7, 10 or (2) a majority threshold relative to the total or maximum number of HFOs in a patient.8, 9, 33-42 We used HFO rate > 1/min and above a threshold of 50% relative to the total number of HFOs in a patient to compare to our new HFO Atlas-based thresholds.
We computed three thresholds using the statistical distribution of normative physiological HFO rates24: (1) a global Atlas threshold, (2) a regional Atlas threshold, and (3) a regional Atlas correction followed by a 10% threshold (regional + 10%). The global Atlas threshold was defined as the 90th percentile value of the distribution of normative HFO rates of all regions combined. This cutoff is commonly used in biomedical statistics to objectively set a threshold; using the 85th or 95th percentile did not change our results (data not shown). We subtracted this value from the automatically detected HFO rates. If the subtraction resulted in a negative value, it was set to zero. The regional Atlas threshold was defined as the region-specific 90th percentile values of the normative rates. If a bipolar channel was recording from more than one region, the threshold was obtained by a weighted average of the region-specific thresholds, the weight of each region being determined by the percentage of each region contributing to that channel. The regional + 10% threshold was calculated by removing the channels that had ≤10% of the total number of HFOs after regional correction. This was done to eliminate channels only marginally above physiological HFO levels; using a 5% or 15% cutoff did not change our results (data not shown).
Six hundred seven bipolar channels (5% total ripple channels) of 49 patients for ripples, and 299 bipolar channels (5% total FR channels) of 23 patients for FRs were also part of the MNI Open iEEG Atlas. For these patients, we recalculated the regional Atlas thresholds excluding the values from that patient, and used these corrected values for further calculation. The regional Atlas threshold for every patient included in the Atlas is therefore independent of that patient's normative values.
2.6 Surgical outcomeOutcome was determined according to the Engel classification43 from the most recent follow-up ≥1 year after surgery, and dichotomized into seizure-free (Engel IA) and non-seizure-free (Engel ≥IB).
2.7 Statistical analysesWe tested for differences in demographic information and group-level differences in event rates between resected and nonresected channels of seizure-free and non-seizure-free patients using Mann–Whitney U (MWU), chi-squared, or Fisher exact tests depending on the type and distribution of the variable.
To evaluate whether physiological HFO correction improved identification of the epileptic focus, we compared the HFO region to the resection cavity. We defined channels with HFOs above threshold that were or were not resected as true positive (TP) or false positive (FP), and channels without HFOs or with HFOs below threshold that were or were not resected as false negative (FN) or true negative (TN). We assessed the performance of ripples and FRs above threshold to identify the resection cavity by computing accuracy ([TP + TN]/[TP + TN + FP + FN]), sensitivity (TP/[TP + FN]), specificity (TN/[TN + FP]), positive predictive value (PPV; TP/[TP + FP]), and negative predictive value (NPV; TN/[TN + FN]). Because only in Engel IA outcome is the epileptic focus entirely inside the resection cavity, we separatly analyzed seizure-free and non-seizure-free patients. We tested for differences in performance measures between thresholds, by applying a Wilcoxon signed-rank test to the performance measures of all pairs of different thresholds within the two outcome groups and corrected for multiple comparisons (false discovery rate [FDR] < 0.05 corrected for 50 comparisons: 10 threshold-pairs times five performance measures). We tested for differences in performance measures between seizure-free and non-seizure-free patients using an MWU test (FDR < 0.05, five comparisons: five performance measures). We expected that correcting for region-specific rates of physiological ripples would increase specificity and PPV for identification of the focus. We expected a larger increase in PPV in seizure-free patients.
To evaluate whether physiological HFO correction improved prediction of seizure-free outcome, we allowed residual HFOs in a maximum of 5% of the nonresected channels. We used definitions analogous to the ones described above, but now defined them at the patient level. Patients without HFOs above threshold and good or poor outcome were considered FN or FP, respectively. To test for differences in performance measures between thresholds, we applied a Cochran Q test to the proportions of true and false predictions with different thresholds. If the Cochran Q test was significant after correcting for multiple comparisons (p < .05, five comparisons: five performance measures), we performed post hoc McNemar tests to identify which pairs of thresholds were significantly different. We expected that correcting for region-specific rates of physiological ripples would increase sensitivity and NPV at the outcome level.
We expected greater improvement in performance in patients with a focus in areas generating high rates of physiological ripples according to the MNI Open iEEG Atlas (namely occipital, sensorimotor, and mesiotemporal regions, referred to as ripple-rich cortex) than in patients with a focus in areas generating low rates of physiological ripples (ripple-poor cortex).24 Therefore, we compared tissue and outcome-level predictions between patients with a focus in ripple-rich and ripple-poor cortex using Cochran Q combined with McNemar and Fisher exact tests corrected for multiple comparisons.
The current gold standard to define the area to resect is the SOZ. As a last step, we compared the performance of the best corrected HFO measure to the performance of the SOZ on tissue and outcome level.
3 RESULTSThe study sample consisted of 151 patients (Table S1). Figure 2 displays the different thresholds examined and the group-level results for ripples. It shows the ripple rates in resected and nonresected channels of seizure-free and non-seizure-free patients, and indicates the data used when evaluating the different thresholds. In both seizure-free and non-seizure-free patients, the majority of channels with high ripple rates were resected. In non-seizure-free patients there were more nonresected channels with ripples above the 50% and regional + 10% threshold than in seizure-free patients. Table S2 provides the median values and p-values.

Visualization of the different thresholds examined in this study. Violin plots show the raw ripple rates (A, C, E) and ripple rates relative to a patient's total ripples (B, D) in resected (dark color) and nonresected (light color) tissue in seizure-free (SF; teal) and non-seizure-free (nonSF; red) outcome patients. The colored blocks cover the data points used when evaluating the thresholds (indicated with colored dashed lines) examined in this study: raw ripple rate > 1/min (A; dark blue), 50% of the patient's total ripple rate (B; light blue), the global Atlas threshold (C; yellow), the regional Atlas threshold (E; green), and 10% of the patient's total ripple rate remaining after regional Atlas correction (D; orange). The global Atlas threshold is calculated as the 90th percentile value of the normative rates of all 17 high-frequency oscillation (HFO) Atlas regions combined. The regional Atlas threshold is calculated as the weighted average of the region-specific 90th percentile value of the normative rates obtained from the Montreal Neurological Institute Open iEEG Atlas Project from which an electrode channel is recording. The 17 HFO Atlas regions are indicated on the x-axis in E. SOZ, seizure onset zone
3.1 Ripples 3.1.1 Identification of the resected tissueThe application of any threshold significantly improved accuracy, specificity, and PPV to identify the resected tissue compared to ripple rate > 1/min (Figure 3A, Table 1A). Using the regional + 10% threshold resulted in the highest accuracy, specificity, and PPV in both outcome groups (seizure-free group: accuracy = 77.3%, specificity = 97.1%, PPV = 80.6%; non-seizure-free group: accuracy = 75.4%, specificity = 93.3%, PPV = 42.9%). In seizure-free patients, this was a 1.1% increase in accuracy (p < .001), and a 17.0% increase in PPV (p < .001) compared to the 50% threshold (Table 1A). In non-seizure-free patients, this corresponded to a 4.6% increase in specificity (p = .047), and no difference in accuracy and PPV compared to the 50% threshold. Accuracy using ripple rate > 1/min, specificity using the 50% and regional + 10% thresholds, and PPV using all thresholds were higher in seizure-free compared to non-seizure-free patients (Figure 3A).

Performance of (normalized) ripples, fast ripple (FR) rate of >1/min, and the seizure onset zone (SOZ) to identify the resected tissue (A) or to predict seizure freedom (B). (A) Violin plots of the accuracy (1), specificity (2), and positive predictive value (PPV; 3) of ripples above different thresholds and the SOZ (x-axis) to delineate the resected tissue in seizure-free (teal) and non-seizure-free (red) patients. The dots represent the performance values of the individual patients. The black dots in the thicker blue or red lines show the median and interquartile range. Significant differences in performance values between the thresholds within the seizure-free or non-seizure-free outcome groups are indicated with teal or red significance bars. Significant differences in performance values between seizure-free and non-seizure-free patients are indicated with black significance bars. The number of filled circles indicates the level of significance: one = p < .05, two = p < .01, and three = p < .001. A tilde indicates a trend: p = .05–.1. (B) Line plot indicating the change in accuracy (red), sensitivity (blue), specificity (green), PPV (purple), and negative predictive value (NPV; orange) of ripples with increasingly sophisticated degrees of thresholding and the SOZ (x-axis) to predict seizure-free outcome for all patients (1), and separately for patients with a focus in ripple-rich (2A) and ripple-poor (2B) cortex. Significant differences in performance values between thresholds are indicated with colored significance bars. The number of filled circles indicates the level of significance: one = p < .05, two = p < .01, and three = p < .001. A tilde indicates a trend: p = .05–.1
TABLE 1. Median values of performance measures of ripples above the different thresholds, FR rate > 1/min (B), or SOZ (C) for predicting the resected tissue in seizure-free and non-seizure-free patients, overall and grouped by location of the epileptogenic focus in ripple-rich versus ripple-poor cortex Performance measure Subgroup Accuracy Sensitivity Specificity PPV NPV SF nSF p, SF vs. nSF SF nSF p, SF vs. nSF SF nSF p, SF vs. nSF SF nSF p, SF vs. nSF SF nSF p, SF vs. nSF Ripples above the different thresholds Rate > 1/min All 56.8 48.1 .043a 85.2 83.3 .714 47.7 39.2 .077b 37.3 25.8 .016a 91.1 89.5 .958 RRC 54.0 47.8 .187 65.2 80.0 .907 52.6 43.0 .317 37.8 22.7 .007a 78.6 90.5 .140 RPC 57.7 48.7 .042a 90.0 87.7 .919 45.5 39.0 .138 36.7 27.9 .339 92.0 88.9 .561 50% All 76.2 74.3 .355 27.3 24.2 .682 94.3 88.7 .002a 63.6 41.2 .002a 77.5 81.0 .958 RRC 72.5 76.2 .067b 20.0 25.0 .907 94.5 91.9 .083b 60.0 40.0 .023a 70.3 83.0 .012a RPC 78.8 71.7 .042a 29.4 23.7 .216 94.1 86.9 .008a 66.7 42.0 .017a 82.7 79.4 .622 Global All 77.0 75.5 .355 25.7 20.0 .099b 95.5 92.1 .063b 62.8 41.7 .004a 78.9 81.8 .958 RRC 72.1 77.8 .129 21.4 20.0 .907 94.6 93.1 .317 66.7 46.7 .047a 75.8 83.7 .012a RPC 78.0 72.5 .042a 29.4 19.1 .119 95.9 91.5 .087b 60.0 33.3 .023a 82.6 78.3 .484 Regional All 77.3 71.6 .287 36.1 27.8 .114 92.6 87.9 .063b 66.7 40.0 <.001a 80.6 82.0 .958 RRC 73.5 72.0 .242 16.7 20.0 .907 96.4 92.9 .275 66.7 43.8 .002a 74.6 85.0 .021a RPC 81.2 70.0 .042a 43.8 33.3 .147 90.9 84.8 .044a 65.2 40.0 .002a 86.7 80.6 .484 Regional + 10% All 77.3 75.4 .355 27.0 17.1 .079b 97.1 93.3 .004a 80.6 42.9 <.001a 78.2 80.0 .958 RRC 73.0 77.6 .129 13.0 16.7 .907 100 96.6 .083b 100 33.3 <.001a 73.2 83.3 .016a RPC 80.0 73.4 .042a
留言 (0)