
記住我



A total of 43 patients were included in the analysis. Twenty patients received cryosurgery plus ADT, and the remaining 23 received ADT only. Mean age was 70.3 ± 7.5 years (range, 55‑83) in the cryosurgery group and 68.7 ± 7.2 years (range, 56‑84) in the control group (p = 0.479; Table 1). The 2 groups did not differ significantly in serum PSA, biopsy Gleason score, clinical stage, and bone metastases count. Median CTC count was 4 (IQR, 3‑6) in the cryosurgery group and 6 (IQR, 3‑7) in the control group (p = 0.475).
Table 1 Demographic and baseline characteristicsComplications after cryosurgerySurgery was completed in all 20 patients who opted to receive cryosurgery. The average operative time was 93.3 ± 12.1 min. Urinary tract infection was noted in 7 (35%) patients, but dissipated by empirical antibiotic therapy. No urinary incontinence, urethra injury, rectal injury, and recto-urethral fistulas occurred. All patients could urinate at will after removing the catheter at 3 weeks after surgery.
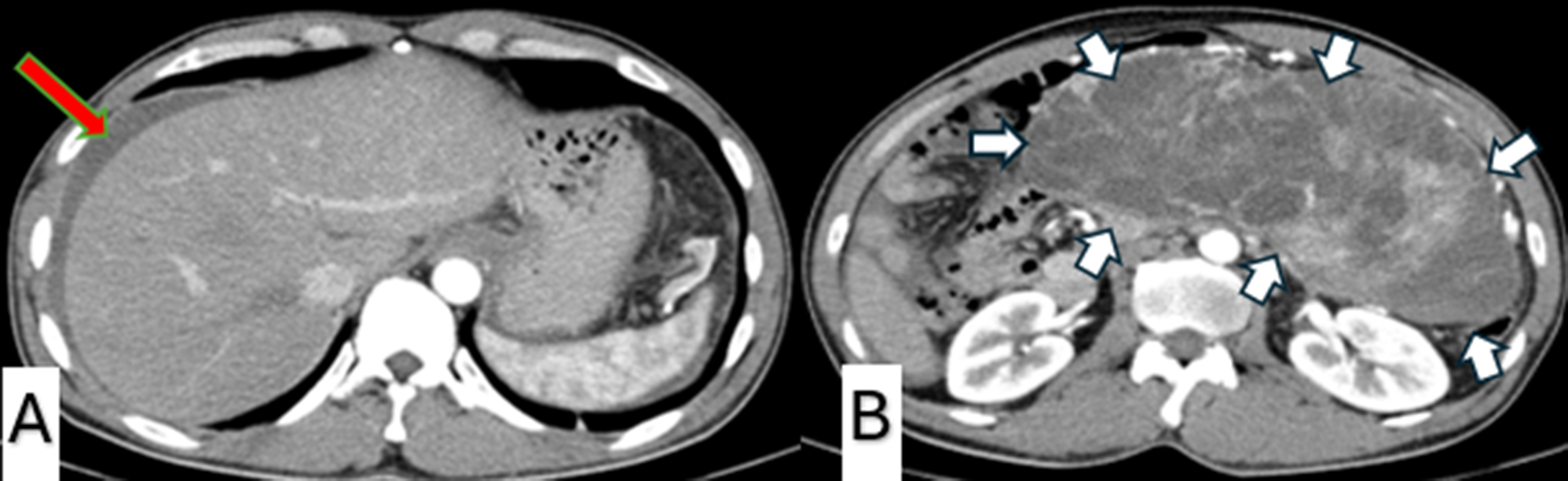
Oncological outcomesThe median follow-up was 32 months (range, 22‑36) in the control group and 36 months (range, 26‑38) in the cryosurgery group. During the follow-up period, two (8.70%) patients in the control group died of myocardial infarction; two patients developed only radiological progression (Fig. 1A, B), and 19 patients developed PSA progression. In terms of subsequent therapy in patients with mCRPC (n = 21), 5 patients (23.8%) had no second-line treatment, 10 patients (47.6%) received abiraterone, and 6 patients (28.6%) received chemotherapy with docetaxel. In the cryosurgery group, two (10%) patients died of myocardial infarction and 1 (5%) patient died of stroke; one patient developed only radiological progression (Fig. 1C), and 16 patients developed PSA progression. In terms of subsequent therapy in patients with mCRPC (n = 17), 3 (17.6%) patients had no second-line treatment, 9 (52.9%) patients received abiraterone and 5 (29.4%) patients received chemotherapy with docetaxel.
Fig. 1
A Nuclide bone scan image of case 1 in the control: baseline vs. radiological progression. B Nuclide bone scan image of case 2 in the control: baseline vs. radiological progression. C Nuclide bone scan image of case 1 in the ADT plus cryosurgery group: baseline vs. radiological progression
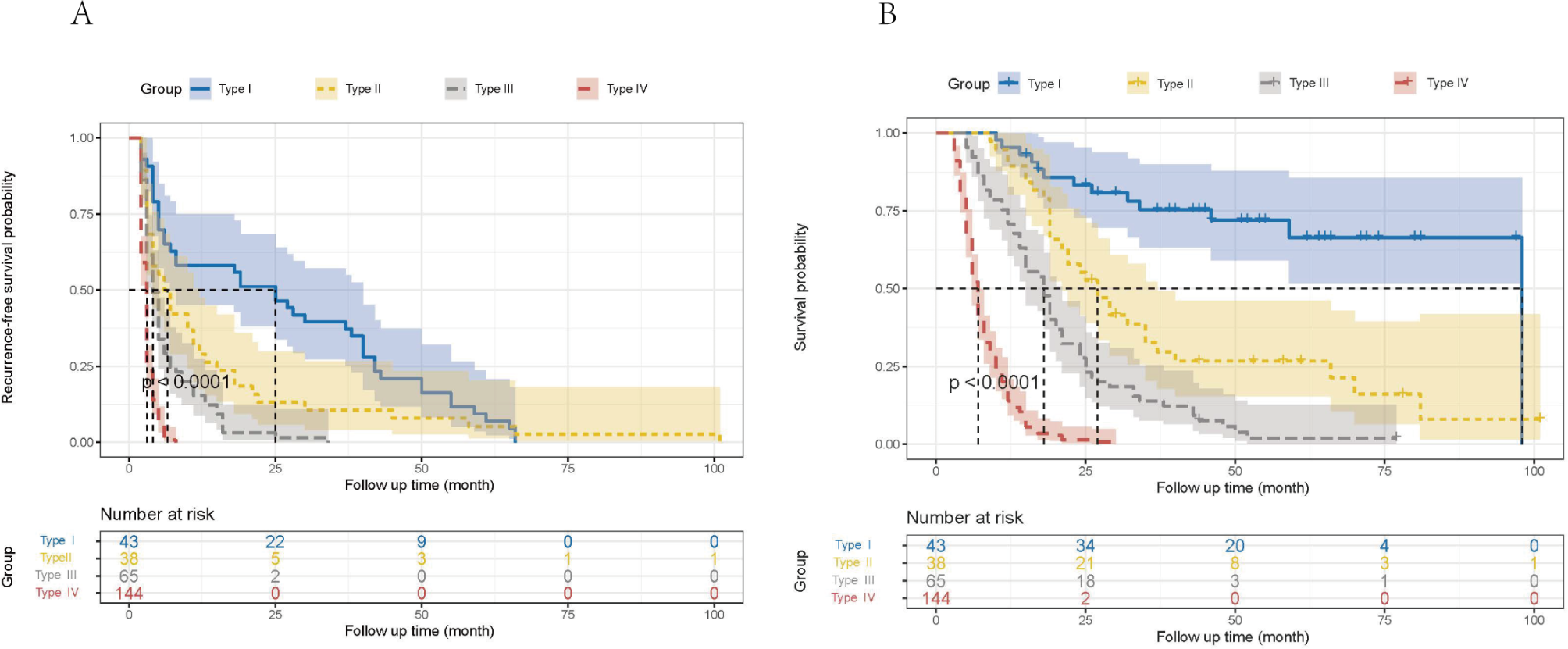
The median PFS was 35 months [interquartile range (IQR) 33‑37] in the cryosurgery group vs. 30 months (IQR 27‑32) in the control group (p < 0.001, Fig. 2A). In the multivariate Cox regression, shorter PFS was independently associated with the following variables: baseline PSA ≥ 100 ng/ml [hazard rate (HR) 6.584, 95% CI, 5.309‑8.166], biopsy Gleason score ≧ 8 (HR 2.064, 95% CI, 1.608‑2.650), clinic T stage > T2b (HR 5.021, 95% CI, 3.925‑6.421), number of bone metastases > 3 (HR 3.421, 95% CI, 2.786‑4.202), positive CTCs at 3 months post-treatment (HR 6.833, 95% CI, 5.176‑9.022), positive CTCs 1 year post-treatment (HR 6.051, 95% CI, 4.347‑8.424). Prostate cryosurgery was associated with longer PFS (HR 0.062, 95% CI, 0.048‑.080) (Table 2).
Fig. 2
A Progression-free survival: a comparison between ADT plus cryosurgery (n = 20) vs. ADT alone (n =2 3). B Sub-group analysis of progression-free survival in the patients with low metastatic volume: a comparison between ADT plus cryosurgery (n = 11) vs. ADT alone (n = 10). C Sub-group analysis of progression-free survival in the patients with high metastatic volume: a comparison between ADT plus cryosurgery (n = 9) vs. ADT alone (n = 13)
Table 2 Multivariate Cox regression of progression-free survivalCTC countCTC count was significantly lower in the cryosurgery group at both 3 months (z = 2.170, p = 0.030) and 12 months (z = 2.481; p = 0.013). The percentage of patients with > 5 CTCs per 5-ml peripheral blood was lower in the cryosurgery group at both 3 (15.5% vs. 43.5%, p = 0.030) and 12 months (0 vs. 30.4%, p = 0.013) (Table 3). In comparison to the baseline, the number of CTCs at both 3 and 12 months was lower in the cryosurgery group (p = 0.004 and p < 0.001, respectively), but not in the ADT alone group.
Table 3 Number/percentage of the patients with different number of CTCs count at baseline, 3 months, and 12 months after treatmentSubgroup analysisAmong the 43 patients, 21 patients had low metastatic volume, and 22 patients had high metastatic volume. In the 21 patients with low metastatic volume, 11 received ADT plus cryosurgery group, and the remaining 10 received ADT alone. In the 22 patients with high metastatic volume, 9 patients received ADT plus cryosurgery, and the remaining 13 received ADT alone. Median baseline bone metastases count was 2 (IQR 1‑3) vs. 8 (IQR 6‑11) in patients with low vs. high metastatic volume (p < 0.001). Median baseline CTC count was 3 (IQR 3‑4) vs. 7 (IQR 6‑8) in patients with low vs. high metastatic volume (p < 0.001).
In the subgroup analysis that included the 21 patients with low metastatic volume only, CTC count was significantly lower in the cryosurgery group at both 3 months (z = 1.969, p = 0.049) and 12 months (z = 2.622, p = 0.009) (Table 4). The median PFS was 37 months (IQR 35‑37) in cryosurgery vs. 30 months (IQR 27‑32) in the control group (p = 0.004; Fig. 2B).
Table 4 Sub-group analysis of CTC count in patients with low metastatic volumeIn the subgroup analysis that included the 22 patients with high metastatic volume only, CTC count did not differ between the 2 groups at any time point (Table 5). The median PFS was 33 months (IQR 28‑35) in cryosurgery vs. 29 months (IQR 24‑32) in the control group (p = 0.076; Fig. 2C).
Table 5 Sub-group analysis of CTCs count in patients with high metastatic volume
留言 (0)