
記住我






In March 2014, the World Health Organization (WHO) was notified of an outbreak of Ebola viral disease (EVD) in Guinea, shortly followed by the neighboring countries Liberia and Sierra Leone. In August 2014, the WHO declared the ongoing outbreak a “Public Health Emergency of International Concern.”1 In the Netherlands, EVD is a “group A” notifiable disease, implicating that the Centre for Infectious Disease Control (CID) of the National Institute for Public Health and the Environment (RIVM) coordinates response on a national level on behalf of the Ministry of Health. Public health services (PHSs) coordinate preparedness and response regionally. Seven regional public health consultants function in 7 regions as intermediates between CID and PHSs to identify needs among PHSs for the CID to react on and to facilitate implementation of CID policy in the PHSs regions.
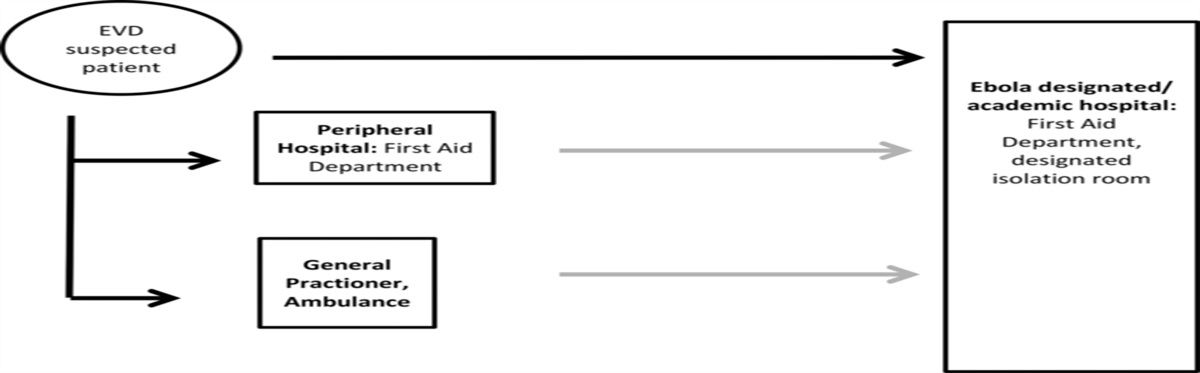
In March 2014, the CID initially alerted PHSs and other specialists in public health, infectious disease, and microbiology about the outbreak and existing Dutch EVD guidelines according to standardized procedures for the event of an EVD import patient.2,3 The expansion of the outbreak, WHO's declaration of a Public Health Emergency of International Concern, and the coinciding increased media attention led to an extended demand for intensified preparedness among curative partners involved in the chain of identification, transportation, isolation, diagnostics, and medical care of patients with possible EVD (Figure 1).3 A patient with potential EVD would consult either a general practitioner (GP) or an emergency department of a hospital, or would be attended by an ambulance (first responders). Upon suspicion of EVD, the first responder would notify the PHS and the patient would subsequently be isolated and referred to an academic hospital for clinical assessment. The CID is informed about all suspected patients, as part of the centralized case ascertainment and because of legal notification requirements by the PHS to the CID. Because of the demand for intensified preparedness among first responders, peripheral and academic hospitals, and public health specialists, the CID organized centralized expert meetings for coordination and consultation and developed elaborated guidelines for amongst others triage, diagnostic procedures, and waste management of possible and confirmed patients with EVD.
 FIGURE 1:
FIGURE 1: Chain of Care for Patient With Suspected EVD (Black Arrows: Own Initiative of Patient, No Isolation Procedures. Gray Arrows: Referral by Ambulance in Isolation) Abbreviation: EVD, Ebola virus disease.
The need for a uniform and joint preparedness among partners in the public and curative health sectors, involving isolation and diagnostic and treatment protocols, was a unique situation in the Netherlands. In the aftermath of the Ebola outbreak, the CID evaluated experiences of the EVD preparedness process among the involved stakeholders. This is in concordance with the recently developed WHO Joint External Evaluation Tool (JEE), which highlights rapid, effective response, requiring multisectoral, national, and international coordination and communication.4 Experiences of EVD preparedness and response in hospitals outside the Ebola epidemic area have been described before5–9; however, the cooperation between the curative and public health sectors in a high-income country has not been addressed. This study investigates the process of preparedness for an introduction of EVD in the Netherlands in both sectors. Second, we aim to identify experienced obstacles and needs among involved parties. Finally, we investigate timeliness of referral of patients to the hospital during the Ebola outbreak as indicator for preparedness of care. Results may be applicable to countries with comparable health systems and support the development of new standardized preparedness protocols overarching both the public health sector and the curative sector.
Methods Study designThis is a mixed-methods study using focus groups, semistructured interviews, and data from the CID records.
Study participantsSeven semistructured interviews, 5 focus groups, and 1 modified focus group were conducted with stakeholders involved in the identification, transportation, and investigation of patients with possible EVD. The interviews were conducted with representatives of national associations (ie, 2 GP networks, PHS, ambulance services, academic hospitals), the health inspectorate, and the working group for hospital infection prevention. The focus groups were conducted with regional public health consultants, PHSs, peripheral and academic hospitals, and regional ambulance services. Twelve PHSs were randomly selected from 3 geographical regions (ie, north, middle, and south) in the Netherlands (4 per region, including at least 1 PHS with experience in referring patients with suspected EVD). Random selection was also applied to ambulance services (12 of in total 25 services) and 6 peripheral hospitals (2 per geographical region). A modified focus group was conducted with 7 GPs; individual perceptions were gathered in separate interviews, which were later combined into 1 general opinion, elaborating on the (recurring) discussed themes.
ProcedureThe study participants were recruited by e-mail and/or telephone. Focus groups (duration: 2 hours) and interviews (ranging between 30 minutes and 1 hour) were conducted in November and December 2015.
The focus groups were semistructured, along 4 main themes. Participants reflected on EVD preparedness with a specific focus on1 their role and engagement in EVD preparedness,2 the process chain of managing a patient with possible EVD at regional level,3 their views on the national coordination by CID, and4 the collaboration between the CID and the curative sector. The same facilitator (A.V.O.) conducted all focus groups assisted by a CID expert in Ebola preparedness and response (dual moderator principle).
The semistructured interviews focused on the role and responsibilities of the stakeholder at the national level and on interorganizational cooperation. The interview guide was pilot tested and adjusted accordingly. The interviews were conducted face-to-face by the same facilitator.
AnalysisAll interviews and focus groups were audiotaped and transcribed verbatim. A summary was sent to the participants for approval. We performed a thematic content analysis and analyzed the transcripts by means of coding. An initial coding guide was established by the facilitator (A.V.O.) on the basis of the main topics of the interviews and focus groups and refined as sub-themes emerged during the discussions. To enhance reliability and reduce researcher bias, 2 other researchers (L.G.C.S. and A.J.) coded the transcripts independently. Afterward, the coding process was compared and differences were discussed until consensus was reached and a final coding guide was established. ATLAS.ti, version 7.5.6 was used as qualitative data analysis tool and was used to structure the coding process and analyze the content of the transcripts.
Timeliness of referral of patients with suspected EVD to academic hospitalsAccording to our national viral hemorrhagic fever guidelines,3 physicians and PHSs consult the CID for triage of patients with potential EVD and to discuss referral of those patients to an academic hospital. The CID records of all referred patients during the Ebola epidemic, March 2014 until April 2016, were collected, including date of onset of illness, first day of contact with a physician, date and time of CID consultation, date and time of decision of referral, and time of arrival at the academic hospital. Referring physicians were contacted for missing information.
Development RecommendationsThe results were presented and discussed at a final plenary meeting with all study participants to gain general consensus and develop recommendations. The names and private information of the study participants were not used in the coding procedures or in the results. Reference was solely based on the organization represented by the study participants.
ResultsIn the study, in total 48 individuals from 42 organizations participated: regional public health consultants (n = 6), PHSs (n = 8), peripheral (n = 6) and academic hospitals (n = 6), ambulance services (n = 8), 7 GPs, and 7 national associations (n = 7). In the final plenary meeting, 27 (56%) persons participated, representing all stakeholder groups. The main outcomes of the study are summarized in the Table.
TABLE - Specific Outcomes Focus Group Sessions Per Stakeholder Stakeholder Relevant Observations (Including Quotes) PHS In some regions, the academic center took the lead in regional coordination preparedness, instead of the PHS. “Clinicians commonly take the initiative for preparedness for emerging infections as EVD; however, they will not coordinate ambulance care and GP preparedness.” “As academic hospitals were responsible for treatment of suspected EVD cases, they immediately took the lead in the region.” Regional public health consultant There were different views of the role of PHSs, which the regional PH consultants tried to streamline. Geographic distribution regarding referral from peripheral hospitals to academic centers was sometimes unclear; the regional consultant helped to clarify this. “Exercises showed missing links in preparedness,” “Handling a suspected EVD patient facilitated coordination in the region.” GPs GPs perceived risk of seeing an actual patient with EVD as being low; therefore, GPs had little involvement in preparedness. “An EVD patient is mainly a concern for hospitals.” “Information provided on websites was sufficient for us.” “Besides providing information to the receptionist, no specific preparedness activities were undertaken.” “In our village, the risk for an EVD patient was considered negligible.” Ambulance Because of limited experience with and exposure of infectious disease, extensive investment in developing protocols and training in, for example, donning and doffing of personal protective equipment was necessary. “The fear of contamination, we really were afraid that the fear of EVD would cause more casualties than EVD itself.” “It took us months to install the correct personal protective equipment procedures.” Peripheral hospital Peripheral hospitals had a small role regarding triage and referral of patients with EVD, but a relative large investment was needed to be prepared adequately. Local preparation depended on own initiatives rather than regional or national coordinated planning. “There was a small risk for an actual EVD patient, but a larger risk for a patient with fever from an endemic area, being a potential EVD patient....” Academic hospital The role to advise and support peripheral hospitals, ambulances, and GPs in preparedness was new and not yet standardized. “It was a process to find out who was the initiator for the coordination in the region.” “Due to differences of peripheral hospitals and GPs between themselves, it was more difficult to connect with them than with the PHS and ambulance.”Abbreviations: CID, center for infectious disease control; GP, general practitioner; PHS, public health services.
All participants were engaged in the Ebola preparedness, except for 4 of 7 individual GPs (57%). All curative stakeholders felt the need to implement an EVD protocol, because patients with common import diseases as malaria also fit the Dutch triage criteria. Academic hospitals had a prominent role in Ebola preparedness, especially regarding supporting and advising curative partners, and in their position as knowledge center for infectious diseases. Although the likelihood of a patient with suspected EVD was considered low, peripheral hospitals and ambulances invested heavily in EVD preparedness. General practitioners did not conduct specific preparedness activities at an individual level.
Preparedness chain patient with possible EVD at regional levelThe starting point of preparedness activities differed between stakeholders, varying from February 2014 to April 2014 (academic hospitals) and July 2014 to August 2014 (ambulance sector, peripheral hospitals), or none (individual GPs). This was due to a difference in the sense of urgency between stakeholders. Preparedness took place first within organizations and then between involved organizations: “There was no crisis.... That was an important delaying factor” (peripheral hospital representative).
Information exchange started within sectors and among professionals and in a second phase between organizations on regional levels. Communication systems did not fulfill the need for information among all stakeholders, for example, for peripheral hospitals. Another barrier for peripheral hospitals was the lack of standardized response protocols, including a medical care protocol for patients with possible EVD for emergency departments. The peripheral hospitals needed more support and advice from the regional academic hospital in the preparation phase compared with previous infectious diseases threats. For academic hospitals, this advisory role was new. Exercises involving regional partners responding to a patient with EVD were considered very valuable. Exercises led to increased knowledge of each other's roles, responsibilities, and expertise.
Academic hospitals and PHSs mostly performed the regional coordination of EVD preparedness; this varied between regions. However, in several regions, it was not clear who coordinated, and some PHSs looked at the CID for guidance and instructions: “It is necessary that regional networks function in a better way, to be prepared for infectious diseases that may constitute a real threat for the public health” (PHS representative).
Academic hospitals proposed to develop national contingency guidelines including standardized criteria for enhanced preparedness and regional coordination. Nonetheless, they felt informed and were satisfied with the information provided by the CID regarding outbreak development in West Africa, and Dutch triage, diagnostic, and personal protective equipment guidelines.
During the Ebola outbreak, medical care for patients with confirmed Ebola was centralized in the national preparedness plans. Four of 8 academic hospitals were selected for prolonged treatment of patients with confirmed EVD. However, this measure did not achieve the intended decreased burden for preparedness for the other academic hospitals.
Other needs from participants involved requests for criteria for institutional preparedness and contingency plans, improved financial compensation for the preparedness investment, and more clearly defined regions for referral to academic hospitals to facilitate regional cooperation in preparedness.
Coordination by CID and cooperation with curative sectorThe coordinating role of the CID was generally accepted and well appreciated especially regarding timeliness and clarity. According to the participants, the CID adequately followed up on developments regarding the ongoing EVD outbreak in West Africa and the implications for the Netherlands; medical professionals were informed through electronic mailing system ([email protected]) about guidelines that provided appropriate information and which were easily accessible through the Internet. For some stakeholders (eg, the ambulance sector), cooperation with the CID was new but useful. Many stakeholders stated that more coordination at the national level is needed, for instance, in clarifying the roles and responsibilities of organizations involved in Ebola preparedness and response by arranging meetings for the exchange of information and best practices and by facilitating the development of curative guidelines. Joint expert meetings with curative and public health stakeholders at the national level were a new initiative by the CID and were considered valuable. Media coverage of the Ebola epidemic in West Africa and patients with confirmed EVD among health care workers in the United States and Europe contributed to fear for exposure among Dutch health care workers. Therefore, more information and standardization of personal protection measures (PPE) were requested, as diversity of PPE was the reason for concern among health care workers: “The PPE caused frustration amongst caretakers, as several times the type of PPE changed to a more safe and protective one” (quote FGS ambulance).
Timeliness of referred patientsBetween April 2014 and January 2016, the CID was consulted 96 times about patients with potential EVD. Thirteen patients were considered suspected patients and were referred and admitted to an academic hospital. Of those patients, 12 were transported by ambulance following isolation procedures, and 1 presented himself at the academic hospital. Delays from date of onset of illness until consultation of a physician varied between 0 and 10 days (median: 1.5 days, n = 12), and delays from physician consultation until CID consultation varied between 0 and 4 days (median: 1 day, n = 12). One patient did not consult a physician, instead a caretaker consulted the PHS directly. Median total delay from first day of illness until CID consultation was 2 days (range: 0-10 days). After decision for referral, it took 5.0 hours until ambulance arrival at the hospital (range: 2.0-7.5 hours, n = 12) (see Figures 2 and 3).
 FIGURE 2:
FIGURE 2: Delays in First Date of Illness—MD Consultation—CID/RIVM Consultation (Days) (N = 12)aaCase no. 8 directly contacted public health service.
 FIGURE 3:
FIGURE 3: Delay in Decision Referral to Academic Hospital—Arrival Hospital (Hours)**Case no. 9 presented himself directly at the academic hospital.
The EVD laboratory tests were negative for all patients, and alternative confirmed diagnoses were malaria (n = 7), bacterial sepsis (1), norovirus (1), and no diagnosis (4).
The results of the interviews and focus groups, as well as timeliness of referrals were presented at the final plenary meeting. After discussions, it was concluded that more centralized support is needed to guide regional coordination and that a clear regional referral system is needed covering the whole country comprehensively. The value of exercises at regional level, both small and large-scale, was emphasized, using existing exercise structures and financial reserves. Developing national contingency guidelines for institutional preparedness was recommended, including regional coordination, roles, and responsibilities of stakeholders and criteria for up- and downscaling in crises. This would secure preparedness between the public health sector and the curative sector.
DiscussionThe intensified preparedness for patients with potential EVD among public health and curative stakeholders created a unique situation requiring not only close cooperation between these sectors but also national coordination of the preparedness to ensure timeliness and uniformity in the management of suspected patients. This study showed the need among stakeholders for a more coherent multisectoral preparedness at the regional level, as well as enhanced guidance from the national level. Interestingly, this approach also has been demonstrated of value in EVD response in low-resource settings such as Nigeria, where an emergency operation center involved a multisectoral and multidisciplinary approach.10 A WHO assessment on Ebola virus preparedness in WHO Southeast Asia region showed that multilevel and multisectoral collaboration and coordination structures were most advanced aspects in preparedness, as a result from pandemic preparedness.11 Van Beneden et al12 also describes US Centers for Disease Control and Prevention outreach to clinicians, including assisting clinicians managing patients with Ebola, sharing updated information with the clinical community, and coordinating information sharing among clinicians managing patients with Ebola in the United States and Europe. We conclude that the multisectoral approach for EVD preparedness has been experienced widely.
Although the likelihood for patients with actual EVD in the Netherlands was considered low, first responders were occasionally confronted with patients with potential EVD. While the CID was consulted on 96 patients with potential EVD, this number is likely higher at the regional level. As every first responder could be confronted with a patient with potential EVD, given the nonspecific symptoms in the early stage of illness and number of travelers to Ebola endemic areas visiting relatives and friends, the CID developed additional triage standards for early detection for first responders. The CID also stimulated regional coordination for referral and isolation procedures.3,6,13 We conclude that in the Netherlands the intensity of preparedness for EVD was at a high level. Nevertheless, the high mortality rate and risk of contamination by contact with symptomatic patients triggered fear among first responders. This finding was reflected in the results of the focus groups' sessions, in which the need for more extensive and explicit guidelines was emphasized, especially regarding the type and use of PPE and specific referral procedures.
In October 2014, the decision was made to centralize prolonged care of patients with EVD in 4 of 8 academic hospitals, in line with other countries.14,15 The anticipated lower burden of preparedness for the 4 not selected hospitals was not achieved, as they all still needed to be able to assess, isolate, and perform laboratory testing of suspected patients. Further centralization, including patient assessments, must be explored.
Participants requested national and interorganizational standardization of type and use of PPE. While national guidelines provided minimum standards, during the course of the Ebola epidemic, several hospitals increased the safety level of PPE. Health care workers did not feel safe when other institutes installed higher PPE standards. In the United Kingdom, it was also observed that clinical staff preferred to use higher levels of PPE than recommended in the guidelines of the Advisory Committee on Dangerous Pathogens.7 Although it is difficult to monitor the implementation of PPE guidelines, the CID can facilitate better exchange of best practices.
The timeliness of detection and referral of patients with potential EVD varied. None of them fully complied with the case definition of a probable case when strictly applying the clinical, epidemiological, and high-risk exposure criteria.3 Only 1 patient had high exposure contact with a patient with confirmed EVD. Absence of high-risk exposure influences the sense of urgency among patient and physician, affecting the delay between first date of illness and CID consultation (median 2 days, range: 0-10 days). The median referral delay was also extensive (5.0 hours, in 10 of 12 patients over 3 hours) and can be attributed to the preparations needed for the ambulance and isolation facility in the academic hospital. Referral delays should be reduced, as the patient might be in need of acute medical care. Morgan et al9 describe a delay in care delivery and even 1 death in the United States because of EVD precautions. Regional multisectorial simulation exercises will lead to shorter referral delays. In addition, a centralized “stand-by” ambulance with an intensively trained, dedicated ambulance team should be considered, as distances and, therefore, traveling times are limited in the Netherlands. In the WHO JEE-Tool, in order to assess one's country capacity to prevent, detect, and rapidly respond to public health threats, R.2.4. indicator in emergency response operation states “Case management procedures are implemented for IHR relevant hazards.”4 Although our health professionals have achieved “case management, patient referral and transportation, and management and transport of potentially infectious patients according to guidelines and/or SOPs,” in our opinion, quantitative indicators as timeliness of procedures are essential to evaluate the functioning of the response in reality. Finally, the question is which delays are relevant to evaluate preparedness for this infection with low incidence but high impact. Referral delay not only affects patients care, it also has public health relevance, as hectic situations around a patient in the public domain easily lead to media attention, and delayed response will harm the public's confidence in health authorities. As most of the patients with suspected EVD actually proved to have malaria, short patient and doctor delay is also essential to install proper lifesaving treatment immediately. Furthermore, in patients with suspicion of a highly contagious disease (such as Ebola), referral delay hampers institution of prompt isolation precautions. For this reason, we consider timeliness of referral to be a relevant indicator for defining preparedness. However, as this might be different for other diseases, indicators for preparedness need to be chosen per event.
A limitation of our study is the selection process of participants in the focus group sessions. This bias was attempted to be reduced by at random selection covering all geographic regions in the Netherlands and including participants representing organizations that experienced handling a patient with suspected EVD. A potential selection bias might have occurred during the coding process, despite an analyzing process by 3 independent researchers. To minimize this bias and to maximize the generalizability, results of this study were presented at a final plenary meeting. Nevertheless, outcomes of this study might not directly be applicable for other countries, as health systems and preparedness procedures vary between countries. The study was performed a year after the main increase of preparations, which can be seen as another limitation as this might have led to recall bias among participants. To mitigate such bias, experiences among participants were recollected during the focus group sessions.
As executers of this study, the CID was not included as stakeholder in the study. A focus group for the CID was performed separately; these results were not included in the earlier described results. The main outcomes, however, were comparable with outcomes of the study. An additional outcome was the question on the role of the regional medical emergency preparedness and planning offices (GHOR) in the Netherlands. In the plenary meeting, their role, especially regarding organizing exercises, was discussed. It was concluded that this stakeholder should be incorporated in the multisectorial preparedness guidelines.
Preparedness for the possible introduction of a patient with suspected EVD was a major effort for both the curative sector and the public health sector on regional and central levels. This evaluation study provides a unique opportunity to share regional and national experiences between these sectors on a national level and provides a stepping stone to reach a common agenda for future contingency planning for emerging infections. Our study shows that coordination between the public health sector and the curative sector requires improvement by standardizing preparedness and response practices to reduce delay in patient management. As a result of this study, in the Netherlands, a national platform for preparedness is established, in which both the curative sector and the public health sector participate to implement the outcomes of this study. Guidelines for institutional preparedness and blueprints for regional and national coordination will be developed, as preparedness for emerging infectious diseases is a multidisciplinary exercise overarching both the public health sector and the curative sector.
Implications for Policy & Practice Preparedness for patients with EVD required intensive cooperation between the public health sector and the curative sector, both on national and on local levels, which was a unique experience in the Netherlands. Median delay in 13 referred patients with suspected EVD to an isolation ward in an academic hospital within the Netherlands was 5 hours (range: 2-7.5 hours), which needs to be reduced by a.o. standardized protocols, more extensive exercises, or a centralized ambulance system. Focus group sessions and semistructured interviews among both public health and curative stakeholders revealed a need for more standardized coordination and operational procedures at regional and national levels, as well as a uniform approach toward institutional contingency planning. Guidelines for institutional preparedness and blueprints for regional and national coordination need to be developed, as preparedness for emerging infectious diseases is a multidisciplinary exercise overarching both the public health sector and the curative sector. References 1. World Health Organization. WHO statement on the 1st meeting of the IHR Emergency Committee on the 2014 Ebola outbreak in West Africa. 2014. http://www.who.int/mediacentre/news/statements/2014/ebola-20140808/en/. Accessed May 4, 2016. 2. European Centre for Disease Prevention and Control. Rapid risk assessment. outbreak of Ebola viral disease in West Africa. http://ecdc.europa.eu/en/publications/Publications/ebola-outbreak-west-africa-1-august-2014.pdf. Updated August 2014. Accessed May 4, 2016. 4. World Health Organization. Joint external evaluation tool: International Health Regulations (2005). http://apps.who.int/iris/bitstream/10665/204368/1/9789241510172_eng.pdf?ua=1. Published 2016. Accessed July 7, 2016. 5. Haverkort JJ, Minderhoud AL, Wind JD, Leenen LP, Hoepelman AI, Ellerbroek PM. Hospital preparations for viral hemorrhagic fever patients and experience gained from admission of an Ebola patient. Emerg Infect Dis. 2016;22(2):184–191. 6. Suwantarat N, Apisarnthanarak A. Risks to healthcare workers with emerging diseases: lessons from MERS-CoV, Ebola, SARS, and avian flu. Curr Opin Infect Dis. 2015;28(4):349–361. 7. Martin TC, Chand MA, Bogue P, et al. Cross-sectional study of Ebola virus disease preparedness among National Health Service hospital trusts in England. J Hosp Infect. 2015;91(1):11–18. 8. Tartari E, Allegranzi B, Ang B, et al. Preparedness of institutions around the world for managing patients with Ebola virus disease: an infection control readiness checklist. Antimicrob Resist Infect Control. 2015;4:22. 9. Morgan DJ, Braun B, Milstone AM, et al. Lessons learned from hospital Ebola preparation. Infect Control Hosp Epidemiol. 2015;36(6):627–631. 10. Shuaib FM, Musa PF, Muhammad A, et al. Containment of Ebola and polio in low-resource settings using principles and practices of emergency operations centers in public health. J Public Health Manag Pract. 2017;23(1):3–10. 11. Vong S, Samuel R, Gould P, et al. Assessment of Ebola virus disease preparedness in the WHO South-East Asia Region. Bull World Health Organ. 2016;94(12):913–924. 12. Van Beneden CA, Pietz H, Kirkcaldy RD, et al. Early identification and prevention of the spread of Ebola—United States. MMWR Suppl. 2016;65(3):75–84. 13. Chea N, Perz JF, Srinivasan A, Laufer AS, Pollack LA. Identify, isolate, inform: background and considerations for Ebola virus disease preparedness in U.S. ambulatory care settings. Am J Infect Control. 2015;43(11):1244–1245. 14. Saito T. Public health challenges and legacies of Japan's response to the Ebola virus disease outbreak in West Africa 2014 to 2015. Euro Surveill. 2015;20(44). http://www.eurosurveillance.org/images/dynamic/EE/V20N44/art21292.pdf. Accessed March 21, 2017. 15. Brosh-Nissimov T, Poles L, Kassirer M, et al. Preparing for imported Ebola cases in Israel, 2014 to 2015. Euro Surveill. 2015;20(44). http://www.eurosurveillance.org/images/dynamic/EE/V20N44/art21290.pdf. Accessed March 21, 2017.
留言 (0)