
記住我


Cancer is the leading cause of death worldwide. According to the National Cancer Center of China in March 2018, breast cancer is the most common cancer occurring among Chinese females aged between 15 and 79 years old.1 This shows that breast cancer nearly affects females of all ages. Especially, adult women who experienced adolescence are considered as high-risk individuals. Breast cancer accounts for 41.82% of all types of female cancers, which means that two in every five female cancer patients may be diagnosed with breast cancer. Moreover, the incidence of breast cancer has been growing rapidly in recent years. Statistically, the incidence of breast cancer increased 3.9% during 2000 and 2011.2 Thus, breast cancer has been well-recognized as a severe public health problem and everyone should attach importance to it. Despite that breast cancer is featured by an increasing high morbidity, its mortality rate is only 70.7%, which means that the therapeutic strategies that are currently used for breast cancer are effective and patients with breast cancer generally have a favorable prognosis.3 However, the morbidity and mortality of breast cancer among Chinese females are significantly higher than the global average. Digital molybdenum mammography has been widely used as one of the most efficient methods for clinical breast examination and breast cancer screening. In China, growing patients are newly diagnosed with breast cancer every year through digital molybdenum mammography. Currently, mainstream therapeutic strategies for breast cancer include surgery (lumpectomy or mastectomy), whole breast radiation therapy, and chemotherapy. Breast cancers can be divided into four or five molecular subtypes based on the status of hormonal receptors and growth receptors, including Lumina-A/B, HER2-positive, normal-like, basal-like, et al.4 Accordingly, the molecular portraits are the key to determine the treatment strategies for breast cancers with different subtypes. Endocrine therapy and targeted therapy are common adjuvant therapeutic strategies for breast cancer. With the help of advanced detection technologies and effective therapies, the long-term survival and quality of life of breast cancer patients have been greatly improved. Five-year survival rate of breast cancer patients in developed countries has reached up to 85%–90%.5 According to the data collected between 2003 and 2005, 5-year survival rate of breast cancer patients in China was 73%.6 However, advanced breast cancer (ABC) is treatable but incurable. Currently, there are few available standard treatments for ABC. According to the fourth ESO-ESMO international consensus guidelines for ABC, ABC patients require a long-term, complex, and multidisciplinary maintenance treatment, which can help with postponing disease progression, improving patients' quality of life, and prolonging patient survival. During the course of illness and treatments, physicians should keep patients informed of their conditions, available treatment options, and supportive and palliative care. Besides, patients should be encouraged to voluntarily participate in the decision-making process about their treatments where they can share their preferences and personal medical experiences with their health care providers. Innovatively, the involvement of oncology nurse practitioners, the application of TELEMEDICINE (provides cancer patients who live in remote regions with medical advises under certain circumstances), fertility preservation, and so on are also of great significance. The combination of advanced anticancer therapies, diverse forms of supportive systems, and high-quality social care can jointly contribute to prolonging the survival of ABC patients.7 However, adverse reactions that come with anticancer treatments generally affect patients' life both physically and psychologically, especially those occurred during or after radiation and chemotherapy. Moreover, the relative-long disease course and poor compliance with treatment in patients may cause more challenges to both health care providers and patients. Thus, there is an urgent need to unite breast cancer patients, their families, our society, our government, and medical institutions to establish a health care model that could provide more customized, long-term, and comprehensive medical services for breast cancer patients, especially for those in China. The establishment of this model could help breast cancer patients benefit from survivorship care and achieve long-term survival with favorable quality of life and integrity.
Over the past decades, health education has been provided to cancer patients mainly by caregivers in Chinese medical institutions, suggesting that cancer patients lack systematic and strategic anticancer guidance. Nowadays, how to provide breast cancer patients with comprehensive high-quality psychological and physiological care and help them recover rapidly and smoothly has received increasing attention in China. Complete case management refers to building a complete case management team consisting of senior nurses and developing individualized health care schemes for breast cancer patients based on their actual needs and individual situations, such as health education before surgery/chemotherapy/radiotherapy, customized care, follow-up calls, free clinics, online Q&A sessions, and so on. Statistically, 96.3% of Chinese breast cancer patients in the trial group reported being satisfied, while only 75.93% of patients who received traditional cancer care were satisfied with their treatments.8 Another study showed that complete case management contributed to a decline of postoperative complications from 18.41% to 5.52%, including bleeding, swelling in the affected arm, subcutaneous edema, and skin-flap necrosis. Compared with the patients with breast cancer in the control group, those in the trial group have a better understanding of the disease.9 A study published in 2005 further confirmed the significance of complete case management to breast cancer patients. This study evaluated the quality of life of breast cancer patients based on multiple dimensions, including physical condition, society/family, emotion, function, and specific factors. Results showed that compared with the patients in the control group, those in the trial group got better scores in all dimensions, which suggested that breast cancer patients who had received complete case management lived a better life.10
The complete case management that is used in China currently has shown great advantages in improving patients' quality of life and promoting patients' satisfaction with oncological care within months or even years after discharge. However, the treatments of breast cancer have been prominently improved and the survivals of breast cancer patients have been greatly prolonged in the past decades. Cancer itself and its treatments may exert multiple potential effects on patients, which may last for years or even decades. Herein, how to provide cancer survivors with proper long-term medical care is a novel problem that needs to be solved. The National Academy of Medicine of the United States released a report in 2005 entitled from cancer patient to cancer survivor: lost in transition, which concluded the problems generated during cancer survivorship care, such as long-term challenges, unmet needs, gaps, and so on.11 Such phenomenon also happened in China. Most of follow-ups may be suspended due to the failed transfer of cancer survivors from oncologists to primary care physicians, even though primary care physicians are willing to provide medical care for cancer survivors. Besides, profiles of patients after receiving different cancer therapies and specific guidelines for survivor care are still unavailable. Therefore, it is of great importance to explore and evaluate potential care models for providing breast cancer survivors with the most efficient and high-quality long-term health care. Current survivorship care guidelines are consensus-based but not evidence-based. According to a report released by the National Academy of Medicine of the United States in 2005, the key components of survivorship care included prevention of new cancers, surveillance for cancer spread, assessment, and intervention for late and long-term effects caused by cancer treatments, and coordination between specialists and primary care providers (PCPs). To meet these requirements, various models of cancer survivorship care have been developed or being developed or evaluated. This study reviews several cancer survivorship care models that have been established.
2 METHODS 2.1 Search strategyThe following search terms were used: models of survivorship care, cancer follow-up care, shared care, disease-specific care, comprehensive survivorship care or program, and follow-up of cancer survivors. The initial search was conducted using online database Pubmed, MEDLINE, and Embase.
2.2 Eligibility criteriaCancer survivorship care studies meeting the following criteria were included in this systematic review: (a) describe the characteristics of cancer survivorship care model; (b) advantages of cancer survivorship care model; (c) disadvantages of cancer survivorship care model; (d) participants involved in the cancer survivorship care model.
2.3 Study selectionTwo researchers independently reviewed titles and abstracts and selected potentially relevant articles. Then, we reviewed the full texts to confirm the eligibility and summarized descriptions, characteristics, cons, pros, participants, effectiveness, and efficiency of each care model from original studies.
3 RESULTS 3.1 Shared care modelShared care model was designed for chronic disease care based on the national conditions of Western countries like the United States. In detail, two or more clinicians who are specialized in different fields jointly offer health care to one patient.12 It is a systematic risk-stratified approach characterized by involvement, communication, and coordination between health care providers with different professional backgrounds. Several studies indicated that this model could be applied in cancer care for survivors.13-15 In this model, a PCP is mainly responsible for non-cancer care. Once a patient is diagnosed with cancer, the patient will be referred to an oncology specialist. The oncology specialist will provide expert care for the patient during the entire treatment as well as after treatment when the patient is at high-recurrence risk. After oncological treatment, the oncologist needs to write a summary of the treatment and develop an individualized survivorship care plan, which will be handed over to both the survivor and his/her PCP for exchanging the physiological condition of the survivor and ensuring his/her post-treatment survivorship care.16 Herein, both oncologists and PCPs are essential for cancer patients and survivors to stay in long-term health. Nurses and nurse practitioners are also key members of both teams of oncologists and PCPs. This model facilitates oncologists and PCPs to coordinate with each other on the follow-up of survivors, which maximizes the allocation of limited medical resources. To apply the shared care model in cancer patients successfully, cancer patients and survivors will be followed up with different frequencies and durations. Besides, risk factors will be well considered and evaluated, including recurrence risk, long-term adverse reactions of therapies, severe after-treatment effects, and psychosocial conditions.16 More importantly, oncology specialists and PCPs communicate with each other periodically to ensure timely knowledge exchange, which thereby helps PCPs to be aware of the long-term and post-treatment influences of cancer treatments.
The shared care model not only improves communication and collaboration between health care providers but also promotes the full use of primary care and other health care professional resources. It also provides a structured mechanism, which realizes high-quality monitoring of survivors and better use of primary care resources. Notably, PCPs would share the responsibility of managing care for cancer patients with oncologists, which partly compensates for the shortage of oncologists. Certainly, a clear division of work and individual responsibilities are needed for oncologists and PCPs to streamline follow-up care for cancer survivors. Also, it is necessary to allow other health care professionals like nurse practitioners and PCPs to engage in cancer survivorship care because of the supply demand imbalance between providers and service needs.
3.2 Disease-specific modelDisease-specific survivorship care model was the earliest iteration of the model that could meet the post-treatment needs of breast cancer survivors. Oncology nurses and physicians firstly observed several complications in cancer survivors, such as lymphedema, fatigue, psychological distress, and weight gain. Then, a multidisciplinary single-disease program was developed for providing the survivors with services including assessing and addressing such problems. This model of survivorship care could either be remained within an institution/cancer center or be incorporated into an institution-wide survivorship program.17 An advantage of this model is that survivors can get access to experts who are specialized in their medical problems or symptoms. However, it generally costs a lot especially in the regions with low-disease prevalence.
3.3 Comprehensive survivor clinic modelComprehensive survivorship programs are currently used multidisciplinary programs that were created and have evolved in cancer centers, hospitals, and practices. In this adult cancer survivorship model, managers come from various academic backgrounds. The short-term goal of this program is to pilot consultative or ongoing care models that can benefit the majority of cancer survivors rather than the limited survivors inside a medical institution. Furthermore, the long-term goal is to establish a comprehensive survivor program that can serve the entire institution and improve cancer care for all survivors. Effectiveness and high efficiency of the program can be achieved by sharing survivor-related clinical and experimental resources and expert opinions inside the institution-wide program.12 Physicians, nurses, and administrators all perform their duties in the team. Psychological services and some other special services are also included in the program. Nurse practitioners are the main force of comprehensive survivorship programs. Some nurse practitioners who are specialized in oncology have gained extensive experience in oncological treatment and can help cancer patients with their on-therapy or short-term health problems. Other nurse practitioners who only have a professional background about primary care can help cancer patients with their common health problems as well. The current comprehensive survivor programs are classified into three types.
Consultative care is the basic model in which survivors are referred to the survivor-program staff that will conduct a single investigation for recording survivors' oncological medical histories and making systematic plans for supervising post-treatment effects. The most distinct advantage of this care model is that it is resource-saving and has the least influence on the long-term health of survivors.
The second type refers to nurse practitioner-dominated survivor clinics that function as an extension of care continuum and can be embedded with treatment teams. At the end of anticancer treatment, survivors will be transferred from the disease-specific group composed by oncologists to nurse practitioners who provide follow-up plans. Then, a shared care program for survivors will be launched by restoring communication between nurse practitioners and PCPs. When survivors are at low-recurrence risk and post-treatment adverse reactions are insignificant, they will be formally transferred to their PCPs. Nurse practitioners will also share the care responsibilities with PCPs by communicating with PCPs periodically and offering updated patient-specific guidelines for follow-up care. Therefore, for keeping survivors in good health and continuing survivor studies, timely effective communication between nurse practitioners and PCPs is fully necessary. Low-labor costs and money costs are the biggest strength of this model. On this basis, oncologists can focus on cancer patients that are newly diagnosed or under anticancer treatment.
The third type of survivorship care program is a specialized multidisciplinary survivor program that involves physicians, nurse practitioners, social workers, psychologists, administrators, and a network of consulting physicians. In this program, survivorship care is provided in a risk-based manner.17 This model originated from pediatric cancer clinics and has functioned well so far. In this model, a minority of survivors are provided with resource-intensive services by multidisciplinary specialized medical teams, which means that a single cancer survivor may face multiple health care providers simultaneously. Hence, the model is featured by a waste of medical resources and not worth being promoted as a universal adult cancer survivorship (Table 1).
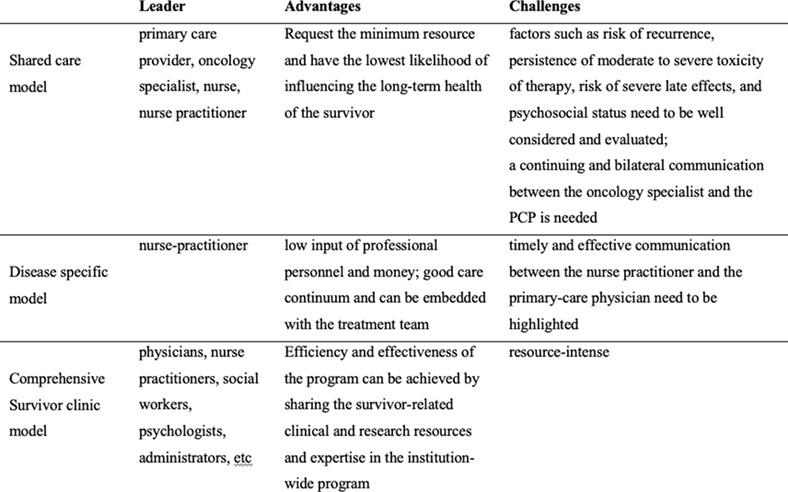
TABLE 1. Comparison of different care models Model Leader Advantages Challenges Shared care model Primary care provider, oncology specialist, nurse practitioners Request the minimum resource and have the lowest likelihood of influencing the long-term health of the survivor; partly compensates for the shortage of oncologists Factors such as risk of recurrence, persistence of moderate to severe toxicity of therapy, risk of severe late effects, and psychosocial status need to be well considered and evaluated; a continuing and bilateral communication between the oncology specialist and the PCP is needed Disease-specific model Nurse-practitioner Low input of professional personnel and money; good care continuum and can be embedded with the treatment team Timely and effective communication among nurse practitioner, physician, and members of multidisciplinary single disease program; not cost-effective in the regions with low-disease prevalence Comprehensive survivor clinic model Consultative care Survivor-program staff Resource-saving; has the least influence on the long-term health of survivors NA Shared care between nurse practitioner and PCP Nurse practitioner and PCP Low-labor costs and money costs; partly compensates for the shortage of oncologists Timely effective communication between nurse practitioners and PCPs is necessary Specialized multidisciplinary survivor program Multidisciplinary program Resource-intensive NA Abbreviation: PCP, primary care providers. 4 DISCUSSIONAll these survivorship care plans originated from Western countries. However, there are plentiful significant structural and cultural differences between Eastern and Western countries, which suggests that these care plans should not be indiscriminately imitated in China. Chinese health care system was established on an oriental background influenced by multiple factors, such as population, economy, culture, and so on. First, the large population of our country places a heavy burden on current cancer survivorship care services. Besides, many medical modes such as allocation of health care resources, ways of health care supply, medical insurances, hospital management, and structures of medical institutions are significantly different between China and other countries. Moreover, it is undeniable that the Chinese health care system has been continuously evolving and has been greatly improved. As people around the world are increasingly aware of the effectiveness and efficiency of long-term survivorship care models, it is a tremendous challenge to develop a cancer survivorship care model that accords with the medical situation of China as well as keeps up with international trends. The improvement and innovation of care models are crucial to achieve optimal clinical outcomes, reduce costs, and improve patients' quality of life and satisfaction with care outcomes.
Currently, multidisciplinary-team management model is widely used in breast cancer survivorship care in China.18 However, this model can only provide care after patients' discharge from hospital in a certain period of time instead of the whole lifecycle. The continuity of care is hardly to achieve without enormous human resource in this model. Rehabilitation clinic lead by case managers is also established in China and some promising results was reported but some free service (health consulting, guidance of rehabilitation exercises, etc) are surprisingly time consuming and could affecting work enthusiasm of case managers.19 It was clearly pointed out that it is necessary to work on the follow-ups after the discharge of patients from hospital and provide transitional care in Outline of Nursing Development Plan in China (2011-2015). And it will be gradually established and improved the long-term nursing care system which is “supported by institutions, based on home care, and relied on community” said in the 12th Five-Year Plan. In the system, people will be provided with long-term care, rehabilitation, health education, and palliative care when is needed.20 According to national conditions, it is suggested to train professionals working on the survivorship care in the future, develop professional theoretic guidelines, build multidisciplinary-team, and emphasize the role of family caregivers to help patients to achieve better quality of life.21
Thus, it can be seen that we are still far from developing a cancer survivorship care plan that is efficient and suitable for the Chinese health care system. Notably, innovative technologies can boost the development of the care model. For example, electronic medical records (EMRs), personal records, real-time capture of biological and self-report data, and electronic platforms for providing interventions are the products of science and technology. Health IT technologies also provide health care team members with access to survivors' health information, which then enhances team cooperation. However, most of the current electronic record systems are proprietary systems that are solely open to the caregivers within a same health care network, which makes it difficult for providers from different health care networks to coordinate with each other. Therefore, it is of great necessity to connect various incompatible EMR systems and provide cancer survivors with follow-up care of high quality and high efficiency.22 In recent years, mobile health (mHealth) has been developed. For survivors, mHealth keeps survivors informed of the latest information about their diseases and functions and promotes their self-management. Meanwhile, health care providers can monitor the symptoms and performances of patients and communicate with patients in real time via mHealth. Nevertheless, innovative technologies have several limitations. First, elderly patients may have difficulties in surfing on the Internet and using smartphones. Second, the reliability and validity of self-report data collected via mHeath technology need to be testified. Therefore, persistent efforts and collaboration among academic institutions, information technology companies, and oncology specialists from diverse communities are needed for maintaining platforms, devices, and applications that can reflect patients' needs and provide better support for cancer survivorship care.23
5 CONCLUSIONThe development of detection technologies for early breast cancer prominently increases the diagnostic rate of breast cancer and saves a lot of time for anticancer treatment. Meanwhile, effective anticancer treatments help patients survive longer. Accordingly, there is a growing population of long-term breast cancer survivors, which causes an increase in survivor demand for a durable comprehensive survivorship care model. Although the validity and reliability of many cancer survivorship care models have been testified by clinicians from Western countries, whether these models could be applied in China is uncertain because of the differences in economic, cultural, population, medical structures, and resource aspects between our country and other countries. In terms of limitations, the universal problems that come with cancer survivorship care models like shortage of human resources can be solved with the help of innovative technologies. With the development of health care services, Health IT technologies such as EMR and mHealth have been used as adjuvant resource-saving tools for efficiently improving the continuity and integrity of survivorship care, which can better meet the needs of increasing breast cancer survivors when compared with traditional face-to-face visits.
Optimal survivorship care constructs are still being explored and developed. The establishment and evaluation of care models have just begun. It should be noted that no survivorship care model can be a “one size fits all” model, which means that there are no models suitable for all medical settings and proper combination of certain models may function best under some conditions. Thus, every model needs to be adjusted based on various factors. Both collaboration among health care providers (oncologists, nurse practitioners, PCPs, etc.) and involvement of nurses in cancer survivorship care are key points to ensure better cancer care for survivors. Future researches should be focused on how to develop best care models for cancer survivors and provide continuous integrated survivorship care models for breast cancer survivors.
CONFLICT OF INTERESTThe authors declare no conflicts of interest.
AUTHOR CONTRIBUTIONSDejing Xu contributed to the conception of the study and helped perform the analysis with constructive discussions. Shuchang Lou performed the experiment and performed the data analyses and wrote the manuscript. Jun Li contributed significantly to analysis and manuscript preparation.
ETHICS STATEMENTThe study was approved by the insititutional review board (CWO) of Jiangsu Cancer Hospital, China. All patients provided written informed consent.
留言 (0)