Trial Design and Oversight
We conducted this investigator-initiated, randomized, head-to-head, placebo-controlled trial at Hvidovre Hospital and the University of Copenhagen, Denmark. Participants followed a low-calorie diet of 800 kcal per day (Cambridge Weight Plan) for 8 weeks. All the participants who had a weight loss of at least 5% of their baseline body weight were randomly assigned, in a 1:1:1:1 ratio, to one of the following treatment strategies for 1 year: exercise plus placebo (exercise group), liraglutide plus usual activity (liraglutide group), exercise plus liraglutide (combination group), or placebo plus usual activity (placebo group). Randomization was stratified according to sex and age (<40 years vs. ≥40 years of age) (see Methods Section A in the Supplementary Appendix, available with the full text of this article at NEJM.org).
Participants, assessors, and investigators were unaware of the trial-group assignments with regard to liraglutide or placebo. To support the maintenance of weight loss after randomization, all the participants were to attend 12 individual consultations that included measurement of body weight and dietetic support complying with the dietetic recommendations for sustained weight loss from the Danish authorities (see Methods Section B in the Supplementary Appendix). The trial was approved by the local ethics committee and the Danish Medicines Agency and was conducted according to the principles of the Declaration of Helsinki and Good Clinical Practice guidelines. All the participants provided written informed consent before the first trial visit.
Our primary trial report adheres to the CONSORT (Consolidated Standards of Reporting Trials) guidelines. The trial design has been published previously,26 and the protocol, with the statistical analysis plan, is available at NEJM.org.
Eight of the authors designed the trial, and nine authors gathered data. Statistical analyses of hypothesis-based end points (change in body weight [primary] and body-fat percentage [secondary]) were performed in a blinded manner with regard to group assignment by a statistical assessor who is an author but who was not involved in the trial design and execution. Four of the authors analyzed other end points. All the authors had full access to all the data and vouch for the accuracy and completeness of the data and for the fidelity of the trial to the protocol. The first four authors and the last author wrote the first draft of the manuscript, which all the authors edited and approved. All the authors agreed to submit the manuscript for publication.
Novo Nordisk supplied liraglutide and placebo injector pens, and Cambridge Weight Plan supplied diet-replacement products for the low-calorie-diet phase. The funding partners did not influence or take part in the execution of the trial; in the collection, analysis, ownership, or interpretation of the data; or in the communication of the trial results.
Participants
Eligible participants were adults (18 to 65 years of age) with obesity, which was defined as a body-mass index (BMI; the weight in kilograms divided by the square of the height in meters) of 32 to 43. Diabetes (type 1 or 2) was a major exclusion criterion. Full lists of the inclusion and exclusion criteria are provided in Table S1 of the Supplementary Appendix.
Interventions
The exercise program was designed to meet the World Health Organization (WHO) recommendations on physical activity for health of a minimum of 150 minutes per week of moderate-intensity aerobic physical activity, or 75 minutes per week of vigorous-intensity aerobic physical activity, or an equivalent combination of both.27 Each participant was assigned to an instructor (who had a bachelor’s or master’s degree in exercise physiology) who planned and monitored the individualized programs. After an initial 6-week ramp-up phase, participants were encouraged to attend supervised group exercise sessions (which involved 30 minutes of vigorous-intensity, interval-based indoor cycling and 15 minutes of circuit training) two times per week and to perform moderate-to-vigorous–intensity exercise individually (which mostly involved outdoor or indoor cycling, running, or brisk walking) two times per week. Heart-rate monitors were worn at all exercise sessions to determine whether the requirement regarding weekly time spent at moderate or vigorous intensity was met.
The exercise program was structured but flexible, which meant that participants could substitute group exercise with individual exercise or vice versa; participants could also reduce exercise frequency if the duration was prolonged or the intensity was increased. Modifications were made in agreement between the participant and instructor if deemed necessary in order to reach the sufficient exercise volume (duration×intensity). Adherence was based on the weekly exercise volume. A detailed program description is provided in Methods Section D in the Supplementary Appendix. Participants who were not randomly assigned to trial exercise (i.e., those in the placebo group or liraglutide group) were instructed to maintain usual physical activity.
Liraglutide (at a concentration of 6 mg per milliliter) or volume-matched placebo was injected subcutaneously, starting at a dose of 0.6 mg per day, with supervised weekly increments of 0.6 mg per day; the dose was intended to eventually reach 3.0 mg per day. Participants who had unacceptable adverse effects at a given dose received the maximum dose at which they did not have such effects. Participants remained enrolled in the trial if the use of liraglutide or placebo was discontinued (see Methods Section C in the Supplementary Appendix).
End Points
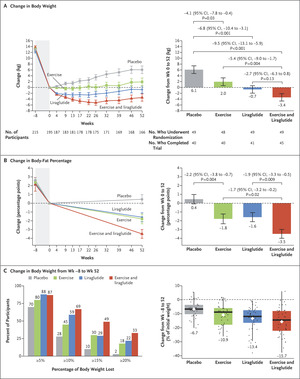
The primary end point was the change in body weight (in kilograms) from randomization to week 52. The secondary end point was the change in the percentage of body fat (calculated as the fat mass [in kilograms] divided by the body weight [in kilograms], times 100) from randomization to week 52. Body weight was measured before the prerandomization low-calorie diet was started, at randomization, and at weeks 1, 2, 4, 9, 13, 17, 22, 26, 32, 39, 46, and 52. The percentage of body fat was measured by means of dual-energy x-ray absorptiometry (Hologic Discovery) before the low-calorie diet was started, at randomization, and at week 52.
Prespecified metabolic health-related end points included changes from randomization to week 52 in fat mass, lean mass, cardiorespiratory fitness, glycated hemoglobin level, indexes of insulin resistance during fasting (liver insulin resistance, as assessed by the homeostatic model assessment of insulin resistance [HOMA-IR]) and during meal intake (whole-body insulin resistance, as assessed by the Matsuda index28), lipid levels, quality of life, waist and hip circumferences, waist-to-hip ratio, blood pressure, and resting heart rate (see Methods Section G in the Supplementary Appendix). Adverse events and the dose of liraglutide or placebo were reported and registered at all visits.
Statistical Analysis
We estimated that a sample of 30 participants in each group would provide the trial with 80% power to detect a minimal clinically important difference in the primary end point, the change in body weight, of 4.0 kg at an alpha level of 0.05.11,21 For the secondary end point, the change in body-fat percentage, we estimated that a sample of 32 participants in each group would provide the trial with 80% power to detect a minimal clinically important difference of 1.5 percentage points at an alpha level of 0.05.13 We anticipated that 68% of the participants would complete the trial (see item 11 in the statistical analysis plan, which is available with the protocol).
In accordance with the prespecified statistical analysis plan, eight hypotheses for the primary and secondary end points were tested hierarchically (see the Hypotheses: Analysis Results and Claims section in the Supplementary Appendix and items 8 and 16 through 18 in the statistical analysis plan). The analyses were performed in the intention-to-treat population.
End points were analyzed with the use of a repeated-measures linear regression model, which included time (factorial), trial group, sex, age group (<40 years vs. ≥40 years), and a time–group interaction as explanatory variables and a repeated effect for visit. A multivariate normal error structure was assumed in the model. All missing data were assumed to be missing at random. Three prespecified supplementary analyses were performed regarding body weight and body-fat percentage — a per-protocol analysis (which excluded participants who had deviations from the protocol), an analysis with adjustment for initial weight loss during the low-calorie diet (to assess the effect of missing data by incorporating further information), and an analysis that used multiple imputations (under the assumption that participants who were lost to follow-up would have a response as if they received placebo, in order to challenge the assumption that data were missing at random) (see items 27 and 28 in the statistical analysis plan). Prespecified end points without hypotheses are reported as point estimates with 95% confidence intervals that were unadjusted for multiple testing, so definite inferences cannot be made regarding those end points.


留言 (0)