
記住我




I took the one less travelled by,
And that has made all the difference - Robert Frost
Despite the ambiguity in Frost‘s idea of nonconformity and individualism that tends to be debated upon till date, here is one road, less travelled over 60 years, that indeed made all the difference.
The QuestThe quest for an antidote for persistent inflammation in eyes with chronic sequelae of Stevens–Johnson syndrome was ongoing, 65 years to be precise. Maumenee, in 1956, observed continued worsening of superficial vascularization and corneal scarring in eyes of patients with Stevens–Johnson syndrome, features of progressive limbal stem cell deficiency not defined back then. In his own words, he was particularly interested in the isolated areas of keratinization of the tarsal conjunctiva in these eyes and rightly attributed the former to be caused by the latter. He compared its appearance to a dry rough parchment like surface which in certain instances appeared as if it was skin that had migrated onto the tarsal surface across the mucocutaneous junction.[1] He further sought to remedy the cause by superficially scraping off the keratinization but was dismayed to note the prompt recurrence. He went on to perform and subsequently publish the outcomes of mucous membrane grafting (MMG) from the lip following excision of the keratinized strip of tarsal conjunctiva in 13 eyes of eight patients of varied etiologies (SJS-3, eczema-1, radiation induced-1, drug reactions-3) in 1956. He lucidly explained about the mechanical abrasion caused by the tarsal keratinization on the cornea, elaborated upon the non-SJS causes of lid margin keratinization (LMK), highlighted the disappointing outcome with prior medical treatment (topical antibiotics, vitamin A, steroids, and lubricants), and stressed upon the need for what we term today as MMG for LMK. The work of this genius, that like many other innovations from that era got blurred out from the focus of Gen-X and millennial ophthalmologists, could have found the crowning spot in the tabulated literature review of cases operated upon for MMG for LMK in the review article on the subject in this issue of IJO.[2]
Thirty years later, the similar concept regarding the pathophysiology and management was lucidly presented by McCord et al. independently in 1983, highlighting the encouraging outcomes.[3] No further emphasis was placed on this over the next three decades.
The OdysseyIn our personal experience, dismayed by the outcomes of procedures commonly performed during this intervening period (punctal plugs, procedures to correct adnexal disorders, rampant use of topical steroids, limbal allograft for visual rehabilitation), and the deteriorating clinical course of the patients with SJS[4] (then unpublished data), the need for a change in approach became evident. The varying grades of keratinization along the lid margin harming the cornea noted in patient after patient of SJS piqued our scientific curiosity and the desire to act. The corneal aftermath was worse in the eyes that were dry, establishing the friction between the keratinized lid and the cornea during the blinking process to be the cause for the progressive corneal sequelae seen. It thus became imperative to modify the downhill course of the disease by addressing the mechanical causes responsible for ocular surface inflammation apart from the obvious adnexal conditions that were already being targeted. These mechanical causes, namely dry eye and LMK, in all probability negatively influenced the outcomes of procedures adopted then for visual rehabilitation. Apart from the dryness, now routinely treated with punctal cautery, LMK came to be recognized as a crucial treatable cause of blink-related micro-trauma that, if left unattended, slowly snowballed the eye toward the need for a keratoprosthesis.[4]
And almost another 30 years later, despite mucous membrane grafts being routinely used in oculoplastic procedures, but with no immediate precedence or guide to the specific described procedure of MMG for LMK, we revisited and reinitiated it.[567] In the early days, way back in 2005, when we started off by fashioning a central 10 mm mucosal graft just enough to protect the cornea, lessons learnt on the go aided us define the size, thickness, combined use of sutures and fibrin glue, the indications, the timing & the postoperative care; helping us refine the technique enabling the lucid description it finds in this issue of IJO.
The Game ChangerFew procedures in the field of medicine have been weighed upon with the tag of being able to provide the oft desired “window of opportunity” to modify the course of a disease or be termed a game-changer.[8] A peep into the historical evolution of a procedure always provides insights and clarity regarding its essence, necessity, scope for refinements and in this situation, the much-needed virtual hand holding guidance. Adding this procedure to the armamentarium of management of ocular sequelae of SJS caused a paradigm shift in our clinical outcomes of these eyes.[4]
The ScienceAddressing and correcting the LMK induced microtrauma to the ocular surface improves patient comfort facilitating better eye opening* and significantly reduces punctate epitheliopathy of the cornea. This could result in an improved visual acuity and in early cases, lead to reversal of corneal vascularization. It is essential for a beginner to understand the steps of the procedure to ensure a good outcome. Several surgical nuances have been well documented and illustrated for the benefit of a beginner in this review. It is important not to be daunted by the demands of the procedure in terms of timely identification of its need and the meticulousness it warrants. The gratitude expressed by one postoperative patient would be drive enough to never turn back. The symptomatic improvement and its beneficial effect on visual acuity due to a significant change for the better in the ocular surface staining are well known.[123456] Minor variations in performing the procedure by various groups have been largely highlighted and the reader can appropriately choose and follow. Differing schools of thought, especially with respect to use of postoperative steroids, systemic and topical, have been projected to express differing viewpoints. With the disappearance of the cause for inflammation, with very limited surgically induced inflammation as evidenced over a vast reported experience,[35] the need for postoperative topical steroids has not been warranted. In the author‘s experience spanning 15 years, neither bandage contact lens nor topical steroids have found any place in the postoperative regimen with immediate abatement of inflammation in the absence of any risk factor for possible postoperative infection. Even with the impact created by correction of more than 1000 lids witnessed by us over these years, we continue to remain awestruck by the outcome of the procedure [Fig. 1], every single time. This conducive shift in the milieu of the ocular surface from pro to anti-inflammatory was very well documented in our study on tear cytokine profiling and provided insights into the bio clinical changes that occur with LMK and with MMG subsequently.[9] The long unresolved clinical feature of the lesion on the lid margin that mimics early LMK but without its deleterious effects on the surface was discerned on histopathology to be ectopic sebaceous glands, that we termed glands of Gibsan.[10]
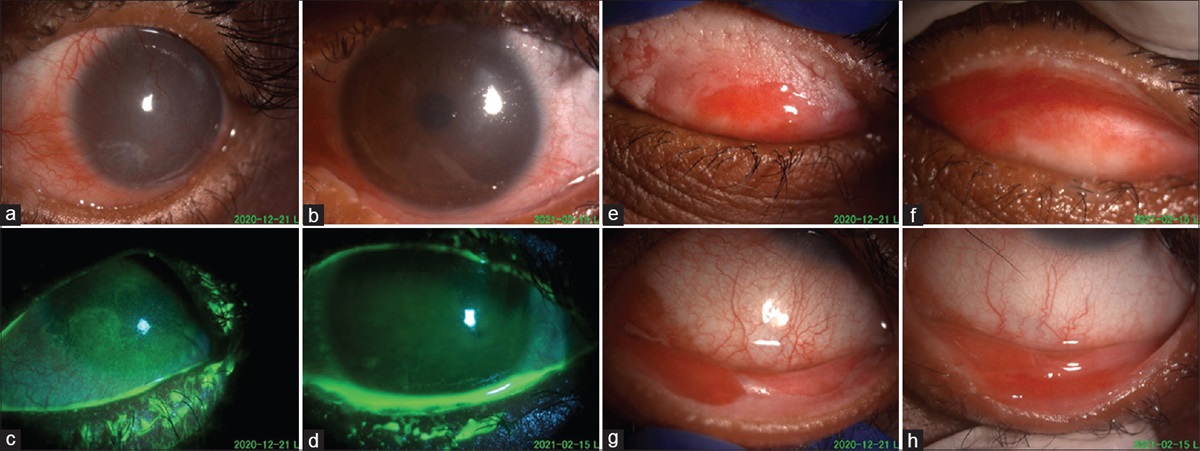
 Figure 1:
Figure 1: Pre and 2-month post-MMG for LMK in the left eye of a 9-year-old child who developed SJS 5 years back following a drug reaction. Lid suture removal was performed at 1-week post-surgery. Postoperative care included topical antibiotic ointment for 2 weeks along with antiseptic mouthwash for 1 week. Topical lubricants are being continued. No perioperative steroids in any form (topical or systemic) were administered. No bandage contact lens was used postoperatively. (a) Preoperative diffuse corneal haze and vascularization of the cornea obscuring details of anterior chamber, exotropia, and gradual decrease of vision in the past 1 year. (b) Postoperative clear cornea with regression of vascularization and restoration of corneal clarity with improvement in vision and exotropia, ready to initiate amblyopia therapy. (c and d) Preoperative diffuse corneal staining (c) completely resolved after the surgery. (e and f) Preoperative (e) diffuse upper tarsal surface keratinization; postoperative (f) well placed and vascularized mucosal graft with restoration of normal lid margin and absence of keratinization. (g and h) Preoperative (g) lower lid margin keratinization; postoperative (h) postoperative well placed and vascularized mucosal graft with restoration of normal lid margin and absence of keratinization. This highlights the effect of constant blink induced microtrauma by the LMK leading to diffuse epitheliopathy and reversible limbal damage and stress causing diffuse vascularization. Further delay in intervention would have led to irreversible limbal stem cell deficiency
The CounselWhile a well done MMG can significantly modify the course of the disease for the better, it is equally important to bear in mind that a poorly performed MMG can worsen the disease status. Hence it is crucial for beginners to read, understand and follow the details of the surgical procedure. It is also at this juncture important to stress upon the fact that MMG for LMK is not a panacea for all issues associated with SJS. It selectively addresses LMK which has manifold deleterious effects on the cornea and these could improve, but to mandate an improvement in the status of the dry eye or the vision following MMG is inappropriate. It is here that the role of punctal cautery and PROSE lenses cannot be overemphasized in association with MMG.[78] The role of MMG is to prevent further deterioration of the ocular surface status caused due to the LMK, and other non-treatable factors such as the effect of the primary insult of the disease on the limbal stem cells, dryness despite maximum management and inherent ocular surface inflammation would continue to exert their influence, albeit on a less traumatized surface. And therefore, the importance of counselling, as has been stressed upon in the review attains a place of extreme importance.
The FutureUltimately, it is but the comprehensive management of this challenging disorder, with specific emphasis on ocular surface stabilization procedures, that controls the narrative of the course of the disease. Further studies are ongoing to understand the role of altered retinoid metabolism in these eyes and its possible therapeutic implications as well as the pathophysiology in recalcitrant eyes.[11] The need of the hour however, is to constantly reinforce the need to proactively utilize the prior window of opportunity within 2 weeks of onset of SJS to perform amniotic membrane grafting that might prevent the occurrence of subsequent LMK.[12] In that scenario, and if one could be granted an even further wishful thinking of being able to prevent the occurrence of SJS, through genetic/HLA diagnostic tests, who knows, another 30 years and this procedure might be relegated back to the shelves of history, with an interesting journey of over a century!
About the authorDr Geetha Iyer, FRCS (Glasgow), FRCS (Ed), FRCOphth
Geetha Iyer completed her training in Ophthalmology and Fellowship in Cornea and External Disease from Sankara Nethralaya, Chennai, India in 2003. She is actively involved in the management of ocular surface disorders and is currently working as Senior Consultant at the Ocular Surface Clinic and the Cornea Services, Sankara Nethralaya. She is currently the President of the Cornea Society of India. She is the Indian Ambassador for the International Tear Film and Ocular Surface Society. She is a Steering Member of the International Kpro Study Group. She is on the Editorial Board of the prestigious Indian Journal of Ophthalmology and The Ocular Surface journals. She was trained by Prof Giancarlo Falcinelli in performing the MOOKP procedure. She has done a short-term observership in Ocular Surface Disorders with Dr Scheffer C G Tseng, Miami, USA and in the Boston Type 1 keratoprosthesis with Prof Claes H Dohlman in 2006. She has so far done more than 250 keratoprosthesis surgeries (MOOKP, Boston Type 1 and 2 Kpro and osteo Kpro). She has several publications and book chapters to her credit. Her work in the management of chronic ocular sequelae of Stevens–Johnson syndrome has been extensive with an aim to preventing the occurrence and deterioration of the sequelae as well as understanding better the immunopathology of the ocular disease. So also, has been her involvement in ocular chemical injuries, their prevention, and management. IJO is proud to have Dr Iyer share her thoughts on eyelid mucous membrane graft - she has played a significant role in refining, teaching and popularizing it.
1. Maumenee AE. Keratitis secondary to keratinization of the tarsal conjunctiva Am J Ophthalmol. 1956;41:477–87 2. Shanbhag SS, Singh S, Koshy PG, Donthineni PR, Basu S. A beginner‘s guide to mucous membrane grafting for lid margin keratinization: Review of indications, surgical technique and clinical outcomes Indian J Ophthalmol. 2021;69:794–805 3. McCord CD Jr, Chen WP. Tarsal polishing and mucous membrane grafting for cicatricial entropion, trichiasis and epidermalization Ophthalmic Surg. 1983;14:1021–5 4. Iyer G, Srinivasan B, Agarwal S, Pillai VS, Ahuja A. Treatment modalities and clinical outcomes in ocular sequelae of Stevens-Johnson syndrome over 25 years--a paradigm shift Cornea. 2016;35:46–50 5. Iyer G, Pillai VS, Srinivasan B, Guruswami S, Padmanabhan P. Mucous membrane grafting for lid margin keratinization in Stevens–Johnson syndrome: Results Cornea. 2010;29:146–51 6. Fu Y, Liu J, Tseng SCG. Oral mucosal graft to correct lid margin pathologic features in cicatricial ocular surface diseases Am J Ophthalmol. 2011;152:600–8 7. Iyer G, Srinivasan B, Agarwal S, Kamala Muralidharan S, Arumugam S. Comprehensive approach to ocular consequences of Stevens Johnson Syndrome - the aftermath of a systemic condition Graefes Arch Clin Exp Ophthalmol. 2014;252:457–67 8. Kohanim S, Palioura S, Saeed HN, Akpek EK, Amescua G, Basu S, et al Acute and chronic ophthalmic involvement in Stevens-Johnson syndrome/toxic epidermal necrolysis - A comprehensive review and guide to therapy. II. Ophthalmic disease Ocul Surf. 2016;14:168–88 9. Gurumurthy S, Iyer G, Srinivasan B, Agarwal S, Angayarkanni N. Ocular surface cytokine profile in chronic Stevens-Johnson syndrome and its response to mucous membrane grafting for lid margin keratinisation Br J Ophthalmol. 2018;102:169–76 10. Srividya G, Angayarkanni N, Iyer G, Srinivasan B, Agarwal S. Altered retinoid metabolism gene expression in chronic Stevens-Johnson syndrome Br J Ophthalmol. 2019;103:1015–23 11. Iyer G, Srinivasan B, Agarwal S, Subramanian K. Ectopic sebaceous glands of Gibsan in eyelid margin- A novel manifestation in Stevens Johnson Syndrome & proposed nomenclature based on an observational case series Ocul Surf. 2020;18:523–5 12. Gregory D. New grading system and treatment guidelines for the acute ocular manifestations of stevens Johnson Syndrome Ophthalmology. 2016;123:1653–8
留言 (0)