
記住我

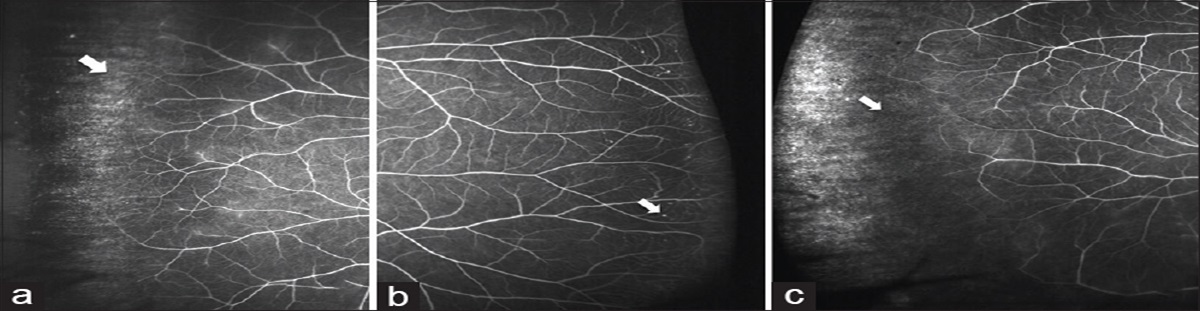



A 35-year-old woman diagnosed with cerebral venous thrombosis and left-sided sixth nerve palsy came for an eye evaluation. On detailed examination, her best-corrected visual acuity was 6/9 in right eye and 6/6 in left eye. Fundus evaluation showed papilledema secondary to raised intracranial pressure (ICP) [Fig. 1a]. The patient was started on treatment with anticoagulants for thrombosis and carbonic anhydrase inhibitors for raised ICP. Baseline visual field evaluation showed enlarged blind spot in both eyes. Ten days later, despite optimization of prothrombin time- INR by the treating neurologist, she returned with drop in vision to 6/24 in both eyes and worsening of visual fields [Fig. 2a].
 Figure 1:
Figure 1: (a) Pre-operative fundus photograph of both eyes showing papilledema. (b) Post-operative fundus photograph showing resolved disc edema with disc pallor
 Figure 2:
Figure 2: (a) Pre-operative 30-2 visual field analysis of both eyes showing constriction of visual fields. (b) Post-operative 30-2 visual field analysis of both eyes showing significant improvement in the visual fields
What is your next step? Serial lumbar punctures Optic nerve sheath decompression (ONSD) both eyes Ventriculoperitoneal shunt Step up dose of oral carbonic anhydrase inhibitors FindingsMRI brain and venogram showed peripheral filling in left proximal transverse, right sigmoid, and right transverse sinus suggestive of subacute cerebral venous thrombosis with bilateral optic nerve tortuosity and bulging of optic nerve head suggestive of papilledema.
Correct answer: B DiagnosisPapilledema secondary to cerebral venous thrombosis.
DiscussionPapilledema develops in 50% of patients with CVT.[1] In the acute phase, the first line of treatment is antithrombotic treatment with low molecular weight heparin along with carbonic anhydrase inhibitors and/or diuretics for raised ICP.[2] Sudden loss of vision despite maximum medical management, is a feature of CVT warranting regular follow-ups and ONSD whenever necessary to salvage the visual function.[3] Our report validates the sudden and progressive loss of visual function in CVT, the appropriate timing of ONSD to salvage the optic nerve with resultant improvement of vision to 6/9, resolution of disc edema [Fig. 1b] and resolution of field defect to near normal in both eyes. [Fig. 2b].
Declaration of patient consentThe authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
1. Crassard I, Bousser MG. Cerebral venous thrombosis J Neuroophthalmol. 2004;24:156–63 2. Ferro JM, Canhão P. Cerebral venous sinus thrombosis: Update on diagnosis and management Curr Cardiol Rep. 2014;16:523 3. Murdock J, Tzu JH, Schatz NJ, Lee WW. Optic nerve sheath fenestration for the treatment of papilledema secondary to cerebral venous thrombosis J Neuroophthalmol. 2014;34:67–9
留言 (0)