
記住我




Ocular trauma is one of the most important causes of unilateral loss of vision, especially in the developing world. Corneal trauma during agricultural activity is of common occurrence.[1]
Management of corneal stromal wooden foreign bodies poses a challenge to the corneal surgeons. Complete removal of a wooden foreign body is mandatory to prevent infection in the cornea. However, the fragile nature of wooden foreign bodies makes en bloc removal extremely difficult. Removal of glass foreign body through a lamellar pocket in the corneal stroma has been described.[2] This method may be useful for the wooden foreign bodies lying horizontally, parallel to the corneal lamella. There is no method described in the literature, for complete removal of full thickness, vertical, corneal stromal wooden foreign body. The authors describe an ab-interno (intracameral) approach for such foreign bodies and demonstrate removal of three foreign bodies using this technique.
Case ReportA 28-year-old male presented with pain, redness, watering, and diminution of vision in the left eye for 3 days. He had a fall on the bush and felt as some thorn has injured his left eye. He consulted the local ophthalmologist, who prescribed topical Gatifloxacin 0.3% (Zymar Allergan India Pvt Ltd) 4 times a day and referred to a cornea specialist for removal of the foreign bodies.
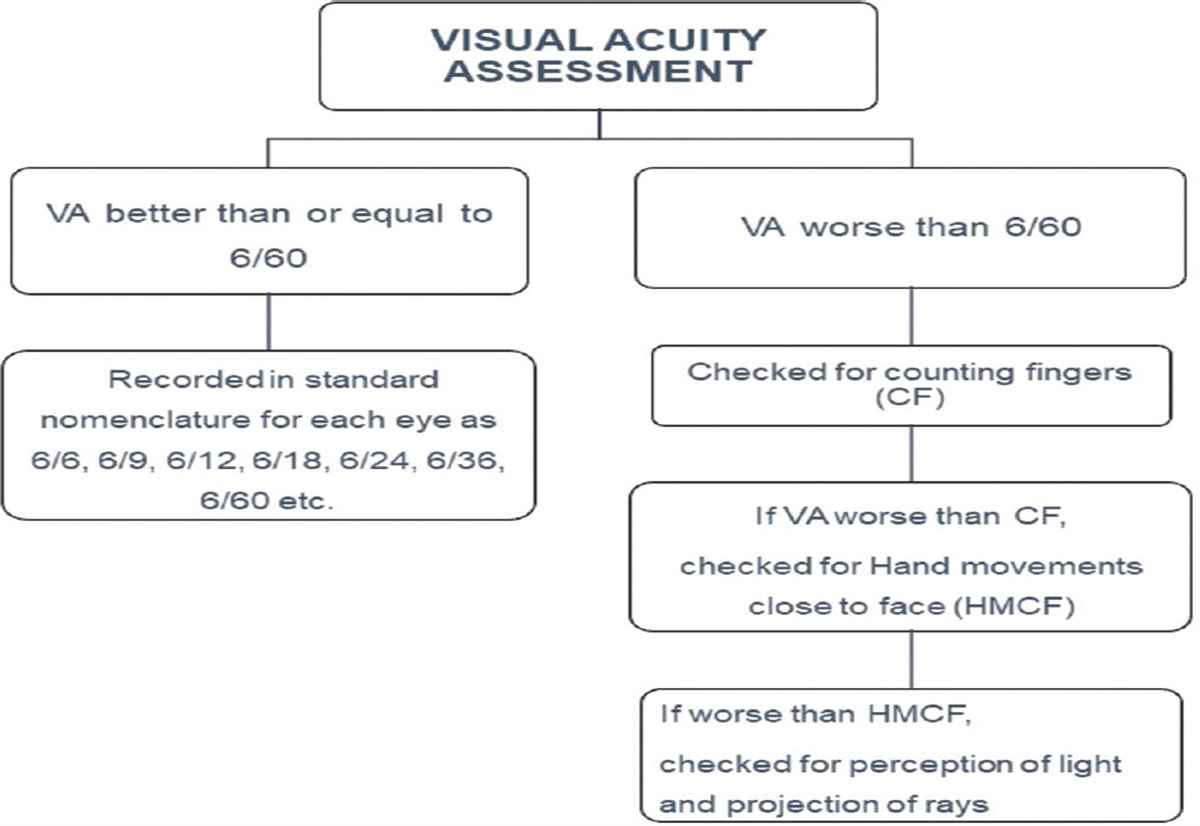
On examination, his visual acuity was 6/6 in OD and 6/18 in OS. Intraocular pressure was 16 mm Hg in the right eye. Slit-lamp examination of the left eye revealed three stromal foreign bodies lying perpendicular to the corneal lamella. One foreign body could be seen piercing the Descemet‘s membrane and the other two were in the stroma. The foreign bodies were embedded in the stroma and were not projecting above the corneal epithelial surface. Fluoroscein stain did not reveal any corneal epithelial defect or black dot against a green background indicating any of the foreign bodies projecting above the corneal surface. There were no infiltrates seen adjacent to the corneal foreign bodies. Examination of the right eye did not reveal any abnormality. The patient was prescribed topical moxifloxacin 0.5% (Vigamox, Alcon Laboratories inc. 6201 South Freeway, Fort Worth, TX 76134 United States) 4 times a day, natamycin ophthalmic suspension 5% (Natacin, Entod Pharmaceuticals Ltd. Ashirwad Building, Opposite Badi Masjid. S V Road, Bandra (West), Mumbai, 400 050, India) 4 times a day and atropine eye drops 1% (Jawa Pharmaceutical India Pvt. Ltd. E 3 Madhya Industrial area Jaipur, 302 017, Rajasthan, India) 3 times a day. The patient was advised urgent removal of corneal wooden foreign bodies.
Surgical TechniqueSurgical procedure: Left eye was cleaned and draped aseptically. A peribulbar injection (5 ml) containing bupivacain hydrochloride 0.5% (Bupitroy 5 mg/ml, troikaa pharmaceuticals Ltd Dehradun, Uttrakhand, India) and Lignocaine hydrochloride 2% (Lox 20 mg/ml, Neon Laboratories Ltd Mumbai, India) was given. The anterior chamber was entered from temporal side using a 15-degree blade (Alcon Laboratories inc. 6201 South Freeway Fort, Worth, TX 76134 United States). The incision was enlarged to 2.0 mm. Sodium hyaluronate was injected into the anterior chamber. An iris repositor was entered into the anterior chamber and the posterior surface of the cornea in the region of foreign bodies was pushed anteriorly. The stroma got compressed and all the three wooden foreign bodies projected above the corneal epithelial surface. Wooden foreign bodies were picked up one by one using McPherson forceps. Sodium hyaluronate was aspirated using Simcoe‘s two-way irrigation and aspiration cannula. Ringer‘s lactate solution was injected into the anterior chamber to check the site of corneal perforation. Leakage of irrigating solution through one of the foreign body tracks confirmed the presence of corneal perforation. Corneal perforation was sealed using Isoamyl 2-cyanoacrylate (Amcrylate; Concord Drugs Ltd, Hayathnagar, Andhara Pradesh India). Corneal epithelium surrounding the corneal perforation was de-epithelialized using crescent blade. Isoamyl 2-cyanoacrylate tissue adhesive was withdrawn into an insulin syringe (1 ml) and a 30 gauge disposable needle was mounted. A smallest possible drop of N butyl cyanoacrylate tissue adhesive was formed. Corneal perforation track was dried using dry Wick cell sponge and the micro drop of Isoamyl 2-cyanoacrylate tissue adhesive was directly applied to the site of perforation. Isoamyl 2-cyanoacrylate tissue adhesive was allowed to polymerize for 30 seconds. The adhesive plug was touched with wet Weck cell sponge to ensure complete polymerization. A drop of the moxifloxacin antibiotic solution was instilled. A bandage contact lens was applied. Postoperative medication included topical moxifloxacin 0.5% (VIGAMOX 5 mg/ml; Alcon Laboratories, USA, Inc.) 4 times a day, natamycin ophthalmic suspension 5% (Natamet 50 mg/ml; Sun Pharma Laboratories Ltd Uttrakhand, India) 4 times a day and atropine 1% (Atro 10 mg/ml; Intas Pharmaceutical Ltd Ahmedabad, India) 3 times a day was instituted. On the first post-operative day, mild corneal edema was noticed. Tissue adhesive plug sealed the corneal perforation very well and the bandage contact lens was in place. Corneal edema resolved within 2 weeks. The postoperative period was uneventful. Isoamyl 2-cyanoacrylate tissue adhesive plug was removed after 4 weeks. The patient had a corneal epithelial defect (3 mm x 3 mm) without any accompanying corneal infiltrate. The bandage contact lens was re-applied. Diagramatic representation of surgical procedure [Fig. 1] and actual steps of the surgical procedure [Figs. 2 and 3]. The video of the surgical procedure has been added as SDC file (mp4 format).
 Figure 1:
Figure 1: Diagramatic presentation of ab-interno surgical procedure, (a) Three full thickness stromal wooden foreign bodies. (b) Paracenetsis. (c) Sodium hylauronate into the anterior chamber. (d) Iris repositor into anterior chamber and cornea being pushed by iris repositor. (e) Foreign bodies projected above cornea surface and picked up with forceps. (f) Cornea after foreign body removal with three foreign bodies shown in the inset
 Figure 2:
Figure 2: Surgical steps of ab-interno surgical procedure. (a) Three full thickness stromal wooden foreign bodies. (b) Paracenetsis. (c) Sodium hylauronate into the anterior chamber. (d) Iris repositor into anterior chamber. (e) Cornea pushed by iris repositor and foreign bodies projected above cornea surface. (f) Foreign bodies picked up with forceps
 Figure 3:
Figure 3: Surgical steps of ab-interno surgical procedure. (a) Corneal perforation detected due to gush of irrigating solution coming out of track of one of the foreign body. (b) Corneal perforation after drying of surface. (c) Cyanoacrylate glue application to the corneal perforation. (d) After Cyanoacrylate glue application. (e) Bandage contact lens application. (f) Three wooden foreign bodies removed
Patient was advised to instill topical moxifloxacin 0.5% (VIGAMOX 5 mg/Ml; Alcon Laboratories, USA, Inc.) 2 times a day and sodium carboxymethyl cellulose 1% (Refresh Liquigel 10 mg/Ml; Allergan USA, Inc) 6 times daily. Treatment was continued for 2 more weeks. After 2 weeks corneal epithelial defect healed and the bandage contact lens was removed and discontinued. The patient achieved unaided visual acuity of 6/9 at 8 weeks follow-up. At 18 months follow up patient did not have any corneal edema and had a best corrected visual acuity of 6/9.
DiscussionThe role of preventive strategies like eye protection during agricultural activities has been well established.[3] Antibiotic prophylaxis at the time of primary care in corneal trauma is also important.[4] However full-thickness corneal foreign body needs urgent referral to a cornea surgeon and can be a surgical challenge.
It is important to ascertain the depth of the wooden corneal stromal foreign body. Fluoroscein stain did not indicate that any of the foreign bodies projected above the corneal surface. The depth of the corneal foreign bodies were clearly visible on direct focal examination on slit-lamp biomicroscopy. Anterior segment OCT is a useful tool to delineate the extent of the corneal wooden foreign bodies. We did not perform the anterior segment OCT as the extent of the corneal foreign bodies were clearly visible.
This case demonstrates that for en bloc removal of full-thickness corneal stromal wooden foreign bodies oriented vertical to corneal lamella, intracameral approach is safe and effective. A localized push from endothelial side compressed the corneal stroma and foreign bodies projected above the corneal epithelial surface. We used the iris repositor to push cornea, but any thinner instrument with round blunt end can be used. The wooden foreign bodies could be picked up with McPherson forceps. The patient developed mild corneal edema which disappeared within 2 weeks. Patients after removal of full-thickness stromal wooden foreign body should always be checked for corneal perforation. In our case corneal perforation was detected and Isoamyl 2-cyanoacrylate tissue adhesive was applied.[5] Fibrin glue would have been a better option. Advantages of fibrin glue include a clearer visual axis, rapid healing and lower risk of corneal vascularization.[5] Patient was prescribed prophylactic antifungal and did not develop fungal keratitis. Foreign body tracks healed, resulting macular corneal opacities. The patient did not have significant corneal endothelial damage and did not develop corneal edema during 18 months follow up. The authors did not find any report on a technique of removal of full-thickness stromal wooden foreign bodies. Authors pushed localized area of foreign bodies from endothelial side that compressed the corneal stroma and pushed the foreign bodies above the corneal epithelial surface.
External approach is safer compared to ab-interno technique. But in our patient external approach was not possible as foreign bodies did not project above the corneal surface. In cases where ab-externo approach is not possible ab-interno technique is a viable option. In this technique, we just touched and pushed anteriorly the area harboring foreign bodies. Corneal stroma got compressed and the wooden foreign bodies projected well above the corneal surface. Wooden foreign bodies being fragile are likely to break resulting incomplete removal, if not firmly held. Corneal wooden foreign bodies need to removed en bloc. In our patient, even after corneal epithelial and stromal scraping we would not have been able to hold stromal foreign bodies firmly. In case, wooden foreign body breaks and incomplete removal occur, the only option left would be lamellar corneal dissection and foreign body removal.[2]
ConclusionIn the author‘s experience the ab-interno (intracameral) approach is a safe and viable option for the removal of full-thickness stromal wooden foreign bodies, which can‘t be removed with ab-externo (external) approach.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
1. Thylefors B. Epidemiological patterns of ocular trauma Aust N Z J Ophthalmol. 1992;20:95–8 2. Au YK, Libby C, Patel JS. Removal of a corneal foreign body through a lamellar corneal pocket Ophthalmic Surg Lasers. 1996;27:471–2 3. Chatterjee S, Agrawal D. Primary prevention of ocular injury in agricultural workers with safety eyewear Indian J Ophthalmol. 2017;65:859–64 4. Upadhyay MP, Karmacharya PC, Koirala S, Shah D, Shakya S, Shrestha J, et al The Bhaktapur eye study: Ocular trauma and antibiotic prophylaxis for the prevention of corneal ulceration in Nepal Br J Ophthalmol. 2001;85:388–92 5. Sharma A, Kaur R, Kumar S, Gupta P, Pandav S, Patnaik B, et al Fibrin glue versus N-butyl-2-cyanoacrylate in corneal perforations Ophthalmology. 2003;110:291–8
留言 (0)