
記住我



Pancreatic cancer has a poor prognosis, particularly for disseminated disease1. The presence of peritoneal metastasis is often associated with ascites and intestinal obstruction, leading to malnutrition and poor performance status, which could deprive patients of the opportunity to receive chemotherapy2. Intraperitoneal chemotherapy appears advantageous owing to higher drug concentrations achieved in the peritoneal cavity, compared with systemic chemotherapy3-6.
Favourable clinical effects of intraperitoneal paclitaxel have been reported in clinical trials of patients with peritoneal metastasis, including those with ovarian3, 4, gastric5, 6 and pancreatic7 cancer. A previous phase II study8 of intravenous and intraperitoneal paclitaxel combined with S-1 for patients with pancreatic cancer and peritoneal metastasis demonstrated good outcomes, with favourable response and disease control rates. The median survival time and 1-year overall survival rate were 16·3 months and 62 per cent, and conversion surgery was performed in one-quarter of the enrolled patients8. Recently, nab-paclitaxel combined with gemcitabine was shown to be the standard treatment option for patients with pancreatic cancer and distant metastasis9.
The aims of this phase I/II study were to determine the recommended dose for the combination of intravenous nab-paclitaxel with gemcitabine and intraperitoneal paclitaxel in patients with pancreatic cancer and peritoneal metastasis, and to evaluate its clinical efficacy and safety.
MethodsThe eligibility and exclusion criteria are shown in Fig. 1. This study was conducted in accordance with the Declaration of Helsinki, and the study protocol was approved by the institutional review board of the affiliated hospital. The registration number for this clinical trial is UMIN000018878. The last follow-up date was 31 December 2019.
Table 1. Clinical responses to treatment No. of patients* (n = 46) Tumour shrinkage (%)† 20 (0–100) CA19-9 Minimum (units/ml)† 72 (4–23 700) Decreased ratio (%)† 84·4 (16·9–99·1) Normalization 12 Objective tumour responses n = 43 Best RECIST category Complete response 2 Partial response 19 Stable disease 20 Progressive disease 2 Response 21 Disease control 41 Peritoneal cytology turned negative 18 Disappearance of ascites 12 of 30 Conversion surgery 8 * Unless indicated otherwise; † values are median (range). CA19-9, carbohydrate antigen 19-9; RECIST, Response Evaluation Criteria in Solid Tumours. TreatmentIf peritoneal dissemination or positive peritoneal cytology was detected during staging laparoscopy or open laparotomy, a peritoneal access port was implanted in the lower abdomen. Intravenous nab-paclitaxel combined with gemcitabine was administered along with intraperitoneal paclitaxel on days 1, 8 and 15, followed by 1 week of rest. The treatment course was repeated every 4 weeks until unacceptable toxicity had developed, disease progression or surgery (Fig. 1). The criteria for surgical resection (conversion surgery) were: an Eastern Cooperative Oncology Group performance status of 0 or 1; marked tumour shrinkage; decrease or normalization of tumour marker levels; washing cytology via peritoneal access port turned negative (twice in a row); and disappearance of peritoneal deposits on staging laparoscopy8. To obtain a sufficient clinical effect with this regimen and avoid early peritoneal recurrence, the decision to proceed to conversion surgery was based on an interval exceeding 8 months between the initial treatment and surgical resection, which was associated with favourable prognosis in patients with initially unresectable pancreatic cancer in a previous study10.
 Study protocol and flow chart
Study protocol and flow chart
GEM, gemcitabine; PAX, paclitaxel.
Primary and secondary endpointsThe primary endpoint of phase II of the study was the 1-year overall survival rate. The secondary endpoints were antitumour effects, symptom-relieving effects, safety and overall survival.
Objective tumour responses were classified according to Response Evaluation Criteria in Solid Tumours (RECIST) guidelines version 1.111. To evaluate antitumour effects on peritoneal metastases, peritoneal washing cytology specimens were examined every 2 months.
Toxicity was monitored weekly and graded according to the National Cancer Institute–Common Terminology Criteria for Adverse Events (CTCAE) version 4.012.
Definition of dose-limiting toxicities and determination of recommended doseThe frequencies of dose-limiting toxicities were evaluated, and the recommended dose was determined during phase I of the study. Dose-limiting toxicities were determined during the first two cycles of chemotherapy. Dose-limiting toxicities were defined according to CTCAE version 4.012 based on the presence of one or more of the following events: grade 4 leucopenia or neutropenia; grade 3 neutropenia complicated by fever of at least 38°C; grade 3–4 anaemia, thrombocytopenia or non-haematological toxicities; and more than 2 weeks of drug withdrawal within one cycle. The maximum tolerated dose was determined, and the previous level was set as the recommended dose13.
Statistical analysisThe sample size was calculated for an estimated overall survival rate at 1 year after treatment initiation for patients with metastatic pancreatic cancer of 25 per cent. Assuming a null hypothesis of 25 per cent and an alternative hypothesis of 45 per cent with a one-sided type I error of 0·05 and power of 0·8, enrolment of 24 patients was required.
Continuous variables are expressed as median (range). Overall survival was defined as the interval from the start of treatment to death from any cause. Survival analysis was based on the Kaplan–Meier method, with evaluation of differences using the log rank test. A binary logistic regression model using the backward method was employed to predict the use of conversion surgery. The level of statistical significance was set at P < 0·050. All statistical analyses were done using JMP® Pro version 14.2.0 (SAS Institute, Cary, North Carolina, USA).
ResultsA total of 50 patients diagnosed with pancreatic cancer and peritoneal metastasis were enrolled in this phase I/II study from seven Japanese centres; ten patients participated in phase I and 46 (including 6 patients from phase I) in phase II (Fig. 1).
Determination of recommended doseDose levels and dose-limiting toxicities in phase I are shown in Table S1 (supporting information). At dose level 1, three of four patients experienced dose-limiting toxicities. Therefore, the next six patients were enrolled at level 0; only one patient experienced a dose-limiting toxicity (grade 4 neutropenia) at this level. Based on these results, the recommended doses for intravenous gemcitabine, intravenous nab-paclitaxel and intraperitoneal paclitaxel were 800, 75 and 20 mg/m2 respectively.
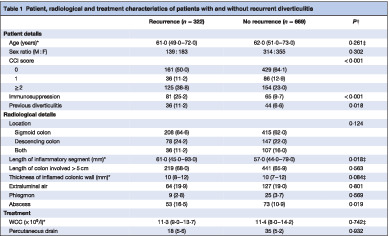
Patient characteristicsA total of 46 patients were enrolled in phase II, and drugs were administered at the recommended dose (level 0). The tumour was located in the pancreatic head in 13 patients and the body/tail in 33. Median tumour diameter was 36 (range 18–64) mm. Primary tumours were categorized as resectable in 12 patients, borderline resectable in 11, and unresectable and locally advanced in 23 patients14. Malignant ascites was observed in 30 of the 46 patients on laparoscopy or laparotomy. All patients had positive intraperitoneal cytology, and 29 had pathological confirmation of peritoneal dissemination. The median duration of treatment was 6·0 (range 0–22·6) months (Table S2, supporting information).
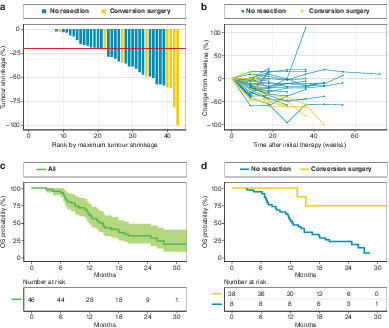
Clinical responses and survival by treatment typeDuring treatment, median primary tumour shrinkage was 20 (range 0–100) per cent (Fig. 2a,b). CA19-9 levels decreased by a median of 84·4 (range 16·9–99·1) per cent, and normalized in 12 patients. The response and disease control rates were 21 of 43 and 41 of 43 respectively. Peritoneal washing cytology turned negative in 18 of 46 patients, and malignant ascites disappeared in 12 of 30 (Table 1).
 Tumour response and survival
Tumour response and survival
a Waterfall plot of tumour shrinkage response. Median primary tumour shrinkage was 20 per cent (red line). b Spider plot showing tumour response over time. The dotted line indicates no change. c Overall survival of 46 patients with pancreatic ductal adenocarcinoma and peritoneal metastasis. The shaded area represents the 95 per cent confidence interval. d Comparison of survival between patients who underwent conversion surgery and those who did not. P = 0·004 (log rank test). OS, overall survival.
Table 2. Clinical characteristics of patients who underwent conversion surgery Patient no. Age (years) Sex Tumour size (mm)* Best RECIST category CA19-9, (units/l)* Operative procedure R Evans grade Tumour stage OS (months) Status 1 74 F 46 → 18 PR 232 → 14 PD + PVR R0 IIB T1 N0 M0 13·5 Dead 2 67 F 25 → 10 PR 837 → 48 DP R0 IIA T3 N1 M0 32·7 Alive 3 75 M 38 → 25 PR 1127 → 43 DP-CAR R0 IIA T3 N0 M0 15·1 Dead 4 73 F 41 → 40 SD 59 → 47 PD + PVR R1 IIA T3 N1 M0 23·4 Alive 5 77 M 30 → 30 SD 246 → 23 DP R0 IIB T2 N1 M0 23·4 Alive 6 54 F 25 → 0 CR 167 → 12 DP R0 IV T3 N1 M0 17·7 Alive 7 74 M 52 → 10 PR 162 → 37 PD + PVR R0 III T3 N0 M0 15·4 Alive 8 77 F 46 → 23 PR 703 → 17 DP R0 III T1 N0 M0 14·2 Alive * Change from before treatment to before surgery. RECIST, Response Evaluation Criteria in Solid Tumours; CA19-9, carbohydrate antigen 19-9; OS, overall survival; PR, partial response; PD, pancreatoduodenectomy; PVR, portal vein resection; DP, distal pancreatectomy; DP-CAR, distal pancreatectomy with coeliac artery resection; SD, stable disease; CR, complete response.All eligible patients were followed up for at least 12 months. Median overall survival was 14·5 (range 11·5–19·2) months, and 1- and 2-year overall survival rates were 61 and 32 per cent respectively (Fig. 2c).
Conversion surgeryEight of the 46 patients underwent conversion surgery (Table 2). The tumour was located in the pancreatic body and tail in seven patients. Six patients had peritoneal dissemination at diagnosis, and two patients had positive peritoneal washing cytology plus unresectable locally advanced cancer before surgery. The median time to surgery was 8·8 (range 4·1–12·2) months after the initiation of chemotherapy. Seven patients underwent R0 resection. The Evans (tumour regression) grade was IIA in three patients, IIB and III in two patients each, and IV in one patient.
Concerning overall survival, patients who underwent conversion surgery survived significantly longer than those who did not (median survival not reached versus 12·4 (range 11·0–18·1) months; P = 0·004) (Fig. 2d).
Adverse event profileThe adverse events data are summarized in Table S3 (supporting information). Grade 3–4 haematological adverse events occurred in 35 of 46 patients, including leucocytopenia (22), neutropenia (32), febrile neutropenia (4), anaemia (8) and thrombocytopenia (6). Grade 3–4 non-haematological adverse events occurred in seven patients, including appetite loss (4) and nausea (2). A grade 3–4 peritoneal port problem was observed in one patient.
Prediction of conversion surgery in patients with peritoneal disseminationUnivariable analysis identified a shift to negative peritoneal cytology and normalization of CA19-9 levels as significant predictors of survival. In multivariable analysis, age (odds ratio 1·29, 95 per cent c.i. 1·04 to 1·59; P = 0·020) and a shift to negative peritoneal cytology (odds ratio 32·73, 2·71 to 395·30; P = 0·006) were significant predictors of eligibility for conversion surgery (Table S4, supporting information).
DiscussionThis trial demonstrated the clinical efficacy of a chemotherapy regimen comprising intravenous gemcitabine, intravenous nab-paclitaxel and intraperitoneal paclitaxel, with acceptable tolerability, in patients with peritoneal metastasis from pancreatic cancer. Although the clinical response and survival data did not exceed those of an S-1-based regimen in a previous study8, this strategy represents an option for treating peritoneal disease in countries where S-1 is not available.
Intraperitoneal chemotherapy enables peritoneal deposits to be exposed to high concentrations of drugs without increasing the systemic concentration to toxic levels15. The duration of effectiveness after intraperitoneal administration is determined by the molecular characteristics of the drug. In this regard, paclitaxel is a large-molecule lipophilic drug that is absorbed slowly3. In addition to this pharmacokinetic advantage, combination with systemic chemotherapy is a key variable in intraperitoneal chemotherapy. Ishigami and colleagues16 established the use of intravenous/intraperitoneal paclitaxel combined with S-1 therapy in patients with gastric cancer, and conducted the phase III PHOENIX-GC trial to compare this regimen with standard therapy. The present authors8 also reported the promising clinical efficacy and acceptable tolerability of intravenous/intraperitoneal paclitaxel combined with S-1 therapy in patients with pancreatic cancer and peritoneal metastasis. In the present study, intraperitoneal paclitaxel was added to the combination of intravenous gemcitabine and intravenous nab-paclitaxel, which has been established as a standard therapy for metastatic disease9, and its efficacy was confirmed to be similar to that reported previously for intravenous/intraperitoneal paclitaxel and S-1 therapy.
A previous study17 reported poor overall survival following weekly paclitaxel in patients with pancreatic cancer and malignant ascites. Another study2 revealed median survival times of 8 months in patients with pancreatic cancer and peritoneal dissemination, and 13 months in those with locally advanced disease and positive peritoneal washing cytology. Considering that patients with peritoneal metastasis generally have a poor prognosis, the results of the present study may be considered encouraging. Conversely, no significant improvement was noted compared with the effects of a previous S-1-based regimen8, despite the use of state-of-the-art systemic therapy in combination with intraperitoneal paclitaxel.
Recently, multidisciplinary treatment combining chemotherapy and surgery has been used widely and regarded as a promising strategy. In particular, conversion surgery for metastatic disease has an advantage in that chemotherapy is administered to patients with a better performance status. The combination therapy used in the present study enabled eight of 46 patients to be eligible for conversion surgery. The median survival time was not reached in patients who underwent conversion surgery, which is a considerable achievement given the generally poor outcomes of patients with pancreatic cancer and peritoneal disease. Median survival time after conversion surgery for pancreatic cancer has generally been reported in the range 30–52 months10, 18-20. The present combination therapy has performed remarkably in terms of both conversion rate and survival outcome, and its potential to control both peritoneal metastasis and the primary tumour was proven. However, this investigation was conducted as a phase I/II study with a single-arm design; the bias in its clinical implications must be recognized. A phase III study is being planned to compare survival outcomes between the intraperitoneal therapy used here and standard chemotherapy.
Regarding adverse events, grade 3–4 haematological toxicities occurred in 35 of 46 patients and non-haematological adverse events in seven. In particular, the rate of haematological toxicities was high, but the incidence and severity were comparable to those of standard chemotherapy regimens9, 21 and previous findings8. In the phase II analysis, grade 4 neutropenia was noted in seven of 40 patients (18 per cent); however, these events were well managed and tolerable. Intraperitoneal port-related adverse events were less frequent than in the authors' initial experience8, which was a meaningful result for this intraperitoneal therapy.
AcknowledgementsS. Yamada and T. Yamamoto are joint first authors of this article. The authors thank S. Hirooka, H. Ryota, N. Kondo, K. Uemura, Y. Nagakawa, A. Tsuchida, A. Matsushita, Y. Nakamura, K. Asai, M. Watanabe, T. Asano, K. Wada, M. Yasunaga, Y. Takada, G. Honda, H. Shinchi, Y. Mataki, S. Shimizu, F. Miura and N. Ikeda, members of the Japan study group of pancreatic ductal adenocarcinoma with peritoneal metastasis, for their contribution to this study; and J. Barber Jr (Edanz Group; https://en-author-services.edanzgroup.com/) for editing a draft of this manuscript.
Disclosure: The authors declare no conflict of interest.
Filename Description bjs11792-sup-0001-Supinfo.docxWord 2007 document , 26.5 KBAppendix S1: Supporting information
Please note: The publisher is not responsible for the content or functionality of any supporting information supplied by the authors. Any queries (other than missing content) should be directed to the corresponding author for the article.
References
1Thomassen I, Lemmens VE, Nienhuijs SW, Luyer MD, Klaver YL, de Hingh IH. Incidence, prognosis, and possible treatment strategies of peritoneal carcinomatosis of pancreatic origin: a population-based study. Pancreas 2013; 42: 72– 75. 2Satoi S, Yanagimoto H, Yamamoto T, Toyokawa H, Hirooka S, Yamaki S et al. A clinical role of staging laparoscopy in patients with radiographically defined locally advanced pancreatic ductal adenocarcinoma. World J Surg Oncol 2016; 14: 14. 3Markman M, Brady MF, Spirtos NM, Hanjani P, Rubin SC. Phase II trial of intraperitoneal paclitaxel in carcinoma of the ovary, tube, and peritoneum: a Gynecologic Oncology Group Study. J Clin Oncol 1998; 16: 2620– 2624. 4Armstrong DK, Bundy B, Wenzel L, Huang HQ, Baergen R, Lele S et al.; Gynecologic Oncology Group. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med 2006; 354: 34– 43. 5Ishigami H, Kitayama J, Kaisaki S, Hidemura A, Kato M, Otani K et al. Phase II study of weekly intravenous and intraperitoneal paclitaxel combined with S-1 for advanced gastric cancer with peritoneal metastasis. Ann Oncol 2010; 21: 67– 70. 6Kodera Y, Imano M, Yoshikawa T, Takahashi N, Tsuburaya A, Miyashita Y et al. A randomized phase II trial to test the efficacy of intra-peritoneal paclitaxel for gastric cancer with high risk for the peritoneal metastasis (INPACT trial). Jpn J Clin Oncol 2011; 41: 283– 286. 7Takahara N, Isayama H, Nakai Y, Sasaki T, Ishigami H, Yamashita H et al. Intravenous and intraperitoneal paclitaxel with S-1 for refractory pancreatic cancer with malignant ascites: an interim analysis. J Gastrointest Cancer 2014; 45: 307– 311. 8Satoi S, Fujii T, Yanagimoto H, Motoi F, Kurata M, Takahara N et al. Multicenter phase II study of intravenous and intraperitoneal paclitaxel with S-1 for pancreatic ductal adenocarcinoma patients with peritoneal metastasis. Ann Surg 2016; 265: 397– 401. 9Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med 2013; 369: 1691– 1703. 10Satoi S, Yamaue H, Kato K, Takahashi S, Hirono S, Takeda S et al. Role of adjuvant surgery for patients with initially unresectable pancreatic cancer with a long-term favorable response to non-surgical anti-cancer treatments: results of a project study for pancreatic surgery by the Japanese Society of Hepato-Biliary-Pancreatic Surgery. J Hepatobiliary Pancreat Sci 2013; 20: 590– 600. 11Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009; 45: 228– 247. 12 Common Terminology Criteria for Adverse Event 4.0. http//evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06 [accessed 14 June 2010]. 13Yamada S, Fujii T, Yokoyama Y, Kawashima H, Maeda O, Suzuki K et al. Phase I study of chemoradiotherapy using gemcitabine plus nab-paclitaxel for unresectable locally advanced pancreatic cancer. Cancer Chemother Pharmacol 2018; 81: 815– 821. 14National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology. NCCN: Plymouth Meeting, PA, 2016. 15Ishigami H, Kitayama J, Otani K, Kamei T, Soma D, Miyato H et al. Phase I pharmacokinetic study of weekly intravenous and intraperitoneal paclitaxel combined with S-1 for advanced gastric cancer. Oncology 2009; 76: 311– 314. 16Ishigami H, Fujiwara Y, Fukushima R, Nashimoto A, Yabusaki H, Imano M et al. Phase III trial comparing intraperitoneal and intravenous paclitaxel plus S-1 versus cisplatin Plus S-1 in patients with gastric cancer with peritoneal metastasis: PHOENIX-GC trial. J Clin Oncol 2018; 36: 1922– 1929. 17Shukuya T, Yasui H, Boku N, Onozawa Y, Fukutomi A, Yamazaki K et al. Weekly paclitaxel after failure of gemcitabine in pancreatic cancer patients with malignant ascites: a retrospective study. Jpn J Clin Oncol 2010; 40: 1135– 1138. 18Donahue TR, Isacoff WH, Hines OJ, Tomlinson JS, Farrell JJ, Bhat YM et al. Downstaging chemotherapy and alteration in the classic computed tomography/magnetic resonance imaging signs of vascular involvement in patients with pancreaticobiliary malignant tumors: influence on patient selection for surgery. Arch Surg 2011; 146: 836– 843. 19Katz MH, Fleming JB, Bhosale P, Varadhachary G, Lee JE, Wolff R et al. Response of borderline resectable pancreatic cancer to neoadjuvant therapy is not reflected by radiographic indicators. Cancer 2012; 118: 5749– 5756. 20Satoi S, Yamamoto T, Yamaki S, Sakaguchi T, Sekimoto M. Surgical indication for and desirable outcomes of conversion surgery in patients with initially unresectable pancreatic ductal adenocarcinoma. Ann Gastroenterol Surg 2019; 4: 6– 13. 21Ueno H, Ikeda M, Ueno M, Mizuno N, Ioka T, Omuro Y et al. Phase I/II study of nab-paclitaxel plus gemcitabine for chemotherapy-naive Japanese patients with metastatic pancreatic cancer. Cancer Chemother Pharmacol 2016; 77: 595– 603.
留言 (0)