
記住我




The ubiquitous nature of social media is undeniable. According to Facebook, by mid-September 2012 the social networking Web site was hosting 1 billion active monthly users,1 or 14.2% of the world’s population.2 In 2012, Twitter announced its users were sending 340 million tweets per day, up 170-fold from 2 million per day in 2009.3 Social media sites and applications have also found their way into the toolboxes of medical students, residents, physicians, and medical educators across the globe.4–7 Given this, harnessing social media’s potential to enhance learning is the logical next step in the evolution of medical education technology.
Web-based tools offer several advantages over in-person/print educational tools: they can overcome physical or temporal barriers, provide searchable content, and encourage interactivity.8 Previous literature reviews have indicated that e-learning can be as efficacious as traditional teaching formats in imparting knowledge.9–12 Looking ahead, an emerging trend in medicine is the use of open-source, user-focused Web-based tools sometimes referred to as “Web 2.0.”13,14 McGee and Begg15 define Web 2.0 as a “collection of Web-based technologies that share a user-focused approach to design and functionality, where users actively participate in content creation and editing through open collaboration between members of communities of practice.”
Social media, which have emerged from this broader context, have been defined in a variety of ways.9,13,15,16 Some definitions are synonymous with those of Web 2.0, some encompass e-learning and distance learning tools, and others take a narrower focus. McGowan and colleagues7 state that:
Social media websites and applications are online environments where users contribute, retrieve, and explore content primarily generated by fellow users. As opposed to more traditional forms of information and communication technologies used in health care organizations, the content generated through social media is typically created by users for users, thus allowing knowledge and support to flow more effectively.
Social media tools have the potential to build on the interactivity of e-learning with additional features that are more learner-generated, collaborative, and engaging.17 However, use of social media by physicians and medical trainees has given rise to concerns about patient privacy and online professionalism.18–21 There is an urgent need for a synthesis of the evidence on social media use in medical education to inform educators and researchers of any demonstrated benefits that would justify the potential risks of incorporating social media tools into educational interventions. Such evidence may lessen the “cultural lag” that often accompanies the adaptation of novel technology to medical education.22
We performed a systematic review of the literature to identify and evaluate studies of educational interventions for physicians or physicians-in-training that included one or more social media tools as a key component of the teaching method. We sought to answer the following questions: (1) How have educational interventions using social media tools affected outcomes of satisfaction, knowledge, attitudes, and skills for physicians and physicians-in-training? and (2) What challenges and opportunities specific to social media use have educators encountered in implementing these interventions?
Method Literature search strategyWe searched the literature in nine databases (MEDLINE, CINAHL, ERIC, Embase, PsycINFO, ProQuest, Cochrane Library, Web of Science, and Scopus), from each database’s start date through our search date (September 12, 2011), for English-language studies on social media use in medical education published in peer-reviewed journals. We defined social media as Web-based technologies that facilitate multiuser interaction around expressive, user-generated content that goes beyond fact sharing. This definition, which was based on an examination of key articles,7,13,14 excluded online technologies that distribute static information (i.e., distance learning) in favor of identifying tools that facilitate idea sharing and evolution through collaboration, interaction, and discussion. We defined medical education as all levels of physician training: medical school, residency, fellowship, and continuing medical education.
Our key search terms were medical education, undergraduate medical education, graduate medical education, continuing medical education, medical student education, and resident education in combination with variations of the following “[All Fields]” terms: social media, social network, Facebook, Web 2.0, Web log, blog, Twitter, podcast, and Webcast. For example, we searched MEDLINE using the following strategy:
(“Facebook”[All Fields] OR “Twitter”[All Fields] OR blogging[MeSH Terms] OR “Webcast”[All Fields] OR “Webcasting”[All Fields] OR “Webcasts”[All Fields] OR “podcast”[All Fields] OR “podcasts”[All Fields] OR “podcasting”[All Fields] OR “Web 2.0”[All Fields] OR “social media”[All Fields] OR “social networks”[All Fields] OR “social networking”[All Fields]) AND (medical education[MeSH Terms] OR “resident education”[All Fields] OR “medical student education”[All Fields]).
To identify additional studies, we hand-searched the reference lists of the studies included in our full-text review.
Article selection and eligibility criteriaTwo of us (T.F., M.C.) reviewed the titles and abstracts of publications identified in the search and selected relevant articles for possible inclusion. We retrieved the full text of these articles for further review against our inclusion criteria, which were as follows: English language, published in peer-reviewed journals, studies of physicians or physicians-in-training, and evaluations of educational interventions (e.g., courses, training activities) that used social media tools. We excluded articles whose full text was not accessible and those that were published in conference proceedings. We resolved any disagreements through discussion until we reached consensus.
Data extraction and synthesisWe developed and piloted a form to extract data from each study that met the inclusion criteria. Data extraction for each study was performed independently by two of three authors, and any differences were resolved by the third author. Our data extraction variables included study authors, year of publication, description of intervention (content, timing, participants), intervention goals, study design (quantitative and/or qualitative), main findings, social media technology used, and opportunities and challenges identified in using this technology.
After data extraction, we reviewed, discussed, and categorized the opportunities and challenges in using social media tools reported by each article. Subsequently, one of us (C.C.) re-reviewed the extracted data to assign categories to each article.
Quality assessmentWe assessed the quality of each included study using the Medical Education Research Study Quality Instrument (MERSQI), a tool designed to evaluate quantitative educational studies.23 The 10-item MERSQI—which has a total possible score of 5 to 18, with higher scores indicating higher quality—assesses the following domains:
study design (single-group cross-sectional or posttest only, single-group pre- and posttest, two groups nonrandomized, or randomized controlled trial); sampling (number of institutions and response rate); type of data (assessment by study participant or objective measurement); validity of evaluation instrument (internal structure and content, relationships to variables); data analysis (appropriateness and complexity); and outcomes (satisfaction/attitudes/opinions, knowledge/skills, behaviors, and/or patient/health care outcomes).In prior studies, intraclass correlation coefficients have been reported at 0.72 to 0.98 for interrater and 0.78 to 0.998 for intrarater reliability.23 Criterion validity has been assessed by expert quality ratings, citation rates, and publication impact factors.23,24 For this systematic review, two of three authors scored each article independently. We resolved discrepancies by discussion. We assessed interrater reliability for each MERSQI domain by calculating a weighted Cohen kappa statistic using R Version 2.14.1.25
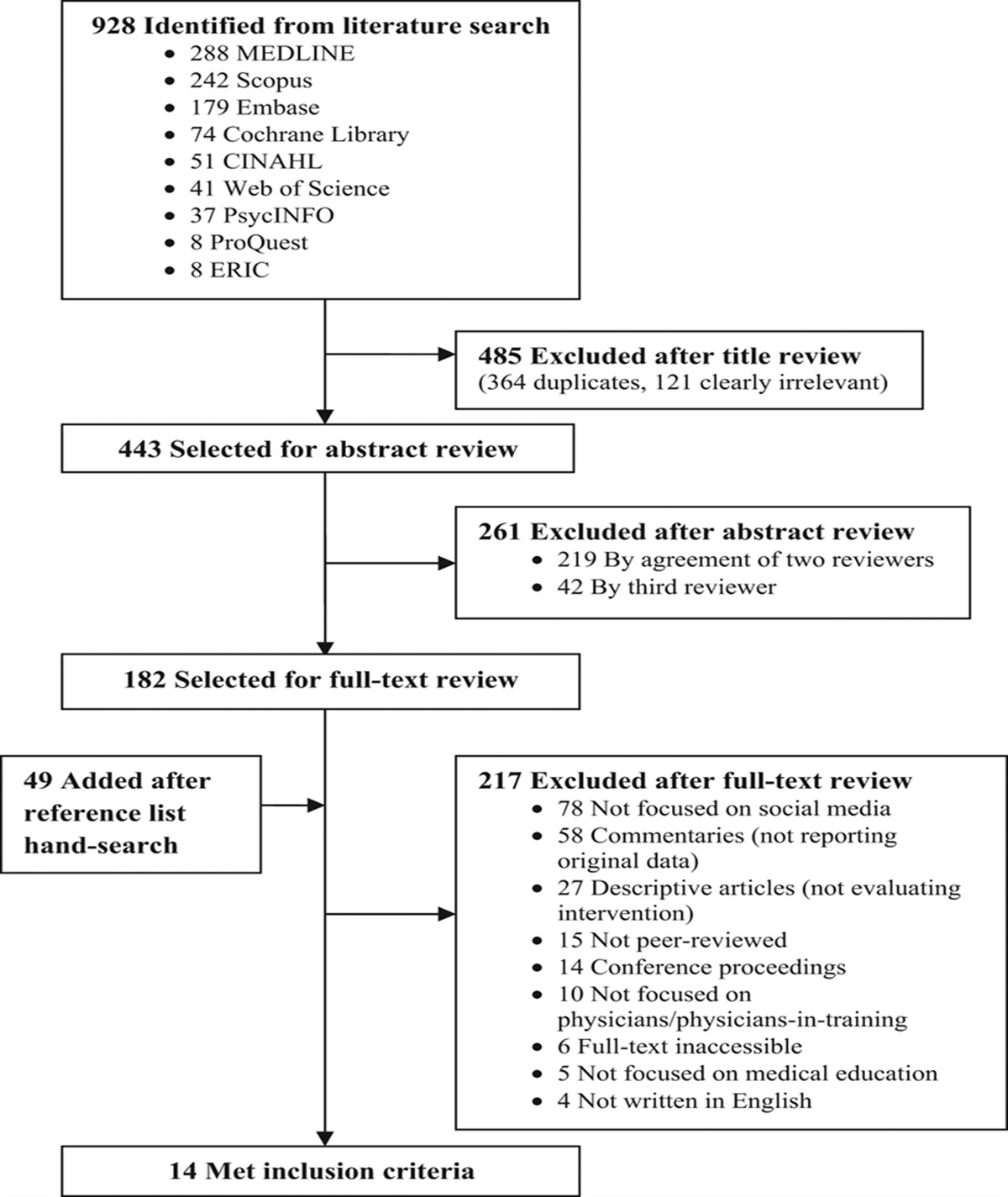
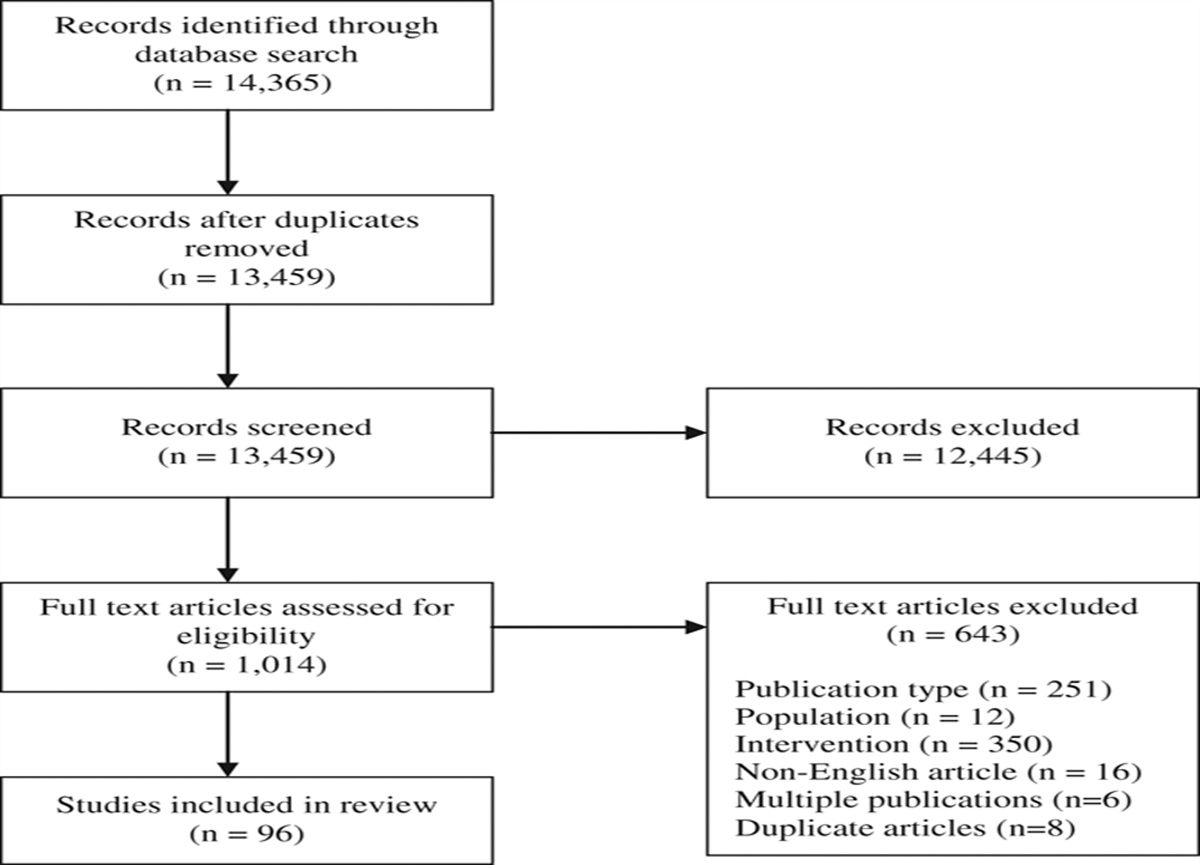
ResultsOur initial database search identified 928 titles from which we selected 443 for abstract review, after removal of duplicates and clearly irrelevant titles. After reviewing abstracts, we selected 182 articles for full-text review. We identified 49 additional articles for full-text review by hand-searching the references of these 182 articles. After full-text review, we determined that 14 studies26–39 met our inclusion criteria (Figure 1).
 Figure 1:
Figure 1: Flowchart for search strategy and review of English-language, peer-reviewed studies on educational interventions for physicians or physicians-in-training using social media tools published through September 12, 2011.
Although the earliest of the 14 articles was published in 2006,26 few studies reporting results of medical education interventions involving social media followed until 2011, when 7 (50%) of the included articles were published. Half of the included articles appeared in medical education journals. The others were published in subspecialty (e.g., nephrology, emergency medicine, dermatology; n = 4; 29%), medical librarian/informationist (n = 2; 14%), and general medicine (n = 1; 7%) journals. Most articles (n = 10; 71%) reported no funding source.
Appendix 1 presents an overview of the 14 included studies’ MERSQI scores, social media tools, participants, aims, evaluation methods, and major findings. The mean MERSQI score was 8.89 (SD: 3.39; range: 5–15.5). Mean domain scores were highest for data analysis (2.00 of 3) and lowest for validity (0.93 of 3). Our mean interrater reliability for all domains was 0.846, indicating excellent agreement.
 Appendix 1:
Appendix 1: Summary of 14 Studies Evaluating the Use of Social Media Tools in Medical Education Interventions, Included in a Systematic Review of the English-Language Peer-Reviewed Literature Published Through September 12, 2011
Social media tools usedBlogs were the most commonly employed social media tool (n = 10; 71%), followed by wikis (n = 3; 21%), Twitter (n = 2; 14%), and Facebook (n = 2; 14%). Seven studies (50%) used a single tool, one study (7%) used two, and three studies (21%) used three or more. One study employed a custom online learning environment, similar to a blog, in which student groups uploaded user-generated content to address questions surrounding clinical cases and posted related comments or questions.29 Another study used Google Maps Application Programming Interface (API) technology to enable students to post annotations to virtual microscopy slides and to provide a social networking component.39 Complementary tools included video conferencing (Skype), media sharing sites (YouTube or Flickr), podcasts, and online modules.30,32,37
Study participantsEleven studies (79%) involved undergraduate medical students only, whereas the other three included practicing physicians,32 staff members,35 or a combination of undergraduates, residents, fellows, and practicing physicians.34
Study aims and designThe main aims of the included studies were to promote empathy, reflection, or professionalism (n = 5; 36%), to enhance clinical skills or knowledge (n = 7; 50%), and to increase interest ina field (n = 2; 14%).
Nine studies (64%) used a single-group cross-sectional or posttest-only design, whereas four studies (29%) employed a two-group nonrandomized design. Only one study (7%) was a randomized controlled trial.29 Nine studies (64%) administered a postintervention survey on user satisfaction and attitudes, whereas two (14%) implemented both pre- and postintervention surveys on technology use, student preferences and satisfaction, or demographics. Seven studies (50%) extracted technology usage data using tools such as Web site hit counters or access history. Four studies (29%) evaluated knowledge using exam scores, three (21%) conducted interviews or focus groups, and two (14%) conducted postintervention analysis of the depth of reflection in student blog entries. One study (7%) measured change in empathy over time using a validated survey instrument.38
Study outcomesLearner satisfaction with social media interventions was described as positive, although in most studies no comparison group was offered.26,33–35 The results of studies that assessed more than one intervention were mixed. For example, students generally favored blogging over essay writing for reflection,36 but they favored in-person problem-based learning (PBL) over virtual collaborative learning for improvement of clinical reasoning skills.29
Interventions to improve knowledge demonstrated equivalent test scores for students who did and did not use social media tools.29,39 However, students who actively participated in a blog-based discussion forum had higher grades than students who posted less often.30 One study reported high knowledge scores on postintervention tests but did not compare participants’ scores with those from nonintervention groups.28 Another study reported quantitative assessment of empathy using the Jefferson Scale of Physician Empathy–Medical Student version.38 It showed that third-year medical students who participated in a humanism and professionalism course that included a blog showed no decline in empathy during their yearlong clerkships; in contrast, previous studies showed a significant decline in empathy among third-year medical students.38 Students reported that the most useful components of the course were the small-group discussions and blog participation, but the effects of activities were not analyzed separately in the study.
In one study, participation in faculty-moderated course blogs and traditional small-group discussions with essay writing were equally effective in fostering medical students’ reflective writing skills.36 Another study found that 169 (95%) of 177 student entries to a faculty-moderated blog were deemed “reflective” and that instructor feedback could stimulate further reflection.27
Most studies did not report intervention costs, but one described changes in resource use,39 including reductions in faculty time and lab session hours, after implementation of a virtual microscopy system for histology teaching. Another study reported cost as a potential barrier to providing portable devices for learners, but this was not quantified.32 No studies evaluated patient outcomes.
Challenges and opportunities specific to social media use ChallengesTechnical challenges in the use of social media were reported by six (43%) of the included studies. For example, signing all students up to participate in a course blog was more time-consuming than expected.27 Another study noted that students initially had trouble posting due to a problem with security settings, but this issue was easily corrected.33 Faculty also encountered technical difficulties in facilitating online discussions.36
Variable levels of learner participation were reported as a challenge in six (43%) of the studies. For example, some groups of students were more active than others on a course wiki, and some students only read others’ posts without contributing their own.31 In another study, 29.0% of students reported that they did not read other students’ posts, and 40.6% indicated that they lost interest in the online component during the course.29
None of the studies reported any adverse events (e.g., breaches of professionalism, compromised patient privacy) during the interventions. Four studies (29%) mentioned specific measures that were considered during design and implementation to address potential privacy concerns, such as including security settings on course blogs to avoid student posts being accessible by anyone outside the course.27,36
Demands on time were also cited as a possible challenge in three (21%) of the studies. Students participating in online PBL groups spent more time on clinical reasoning cases than did students in in-person PBL discussion groups.29 Blog facilitation required more faculty time than did traditional discussion groups, but facilitators reported that this time was well spent and that sharing comments added value to the assignments.36 In contrast, one study found that moving from traditional to virtual microscopy saved faculty time and shortened laboratory sessions.39
OpportunitiesTen studies (71%) reported learner engagement as an important benefit of social media use. By stimulating interaction and learner-generated content, social media tools appeared to promote active learning. Students’ active participation in a course blog correlated with improved grades.30 In addition, the flexibility of online tools allowed customization of learning to fit learners’ needs.28
An advantage of social media tools over traditional teaching methods was that social media tools provided opportunities for more feedback, as reported in eight (57%) of the studies. Social media facilitated faculty and peer feedback to learners on their performance.33 Peer review of posts also overcame potential concerns that students might share inaccurate information.39
Other opportunities included enhanced collaboration (n = 5; 36%), professional development (n = 5; 36%), career advancement/networking (n = 3; 21%), and supportive learning communities (n = 2; 14%). In addition, social media tools were popular with learners (n = 3; 21%), particularly medical students. In four studies (29%), social media tools provided a valuable means of connecting learners to resources and activities to which their access would otherwise be limited by geographic distance or scheduling barriers.
DiscussionTo the best of our knowledge, this systematic review represents the first synthesis of the English-language peer-reviewed literature evaluating the use of social media tools in medical education. In the 14 studies of medical education interventions included in this review, blogs were the most commonly assessed social media tool, and undergraduate medical students were the most commonly targeted population. The included studies demonstrated favorable results related to learner satisfaction, knowledge, attitudes, and skills. Although most of the studies were not of high quality—based on their MERSQI scores (which took into account the studies’ lack of randomization, comparison groups, or validated evaluation instruments)—this is a new area of inquiry, and, thus, it is encouraging to see that several relatively rigorous studies have emerged so early.
Whereas prior reviews have explored the advantages of e-learning over traditional teaching methods in medical education,9–12 we investigated newer social media tools’ potential to enhance learning among physicians and physicians-in-training. Social media tools offer opportunities to foster collaborative learning and engagement. Although privacy breaches are legitimate concerns, none of the studies reported any adverse events. (This may be due to reluctance to share these events or risk minimization through supervision of learners.) Our findings suggest that social media tools can be used safely in medical education settings and that their use may have a positive impact on learner outcomes. These findings have exciting implications for educators and researchers.
For educators, this systematic review presents the small—but growing—body of evidence for the efficacy of social media tools in enhancing medical education. In developing and implementing future interventions, educators should consider ways to maximize the opportunities provided by social media, such as active learning through engagement in user-generated content, facilitation of communication and feedback, collaboration, and access to resources and interaction without physical location restrictions. In addition, they should take into account the challenges reported in the studies reviewed here, including technical issues, varying learner participation, and tools’ security settings. Although the use of social media components in courses and other learning activities can save time by increasing efficiency, it can also be time-consuming. The time spent by faculty and learners on social media should add value to face-to-face instruction if these tools are to be incorporated successfully into medical education curricula.
Researchers should be assured that social media use is a legitimate topic of scientific study.40–42 The body of literature evaluating use of social media in medical education holds ample room for further inquiry. We found there to be a lack of high-quality evidence (e.g., only one randomized controlled trial), infrequent assessment of skill- or behavior-based outcomes, and no assessment of patient-based outcomes in the studies included in this review. New technologies evolve rapidly, often faster than sound evidence for their effectiveness can be established. Although this presents a challenge to researchers, the pace of change can also offer opportunities for innovation, such as engaging learners in curricular development.
Since conducting our literature search, we have endeavored to remain up-to-date in this expanding literature through ongoing reading, discussions with experts in the field, and publication alerts from the MEDLINE and Scopus databases. To our knowledge, two relevant studies have been published since the end date of our search. One study used Twitter and Facebook to share important concepts in a yearlong elective ultrasound course for fourth-year medical students.43 Of the 27 participants who completed the study’s follow-up survey, 88.9% found these social media tools to be user-friendly, and 81.5% found the educational content to be useful. The second study used a social networking portal compatible with low-bandwidth Internet connections to deliver dermatology instruction to eight medical students and interns in Somaliland and to allow participants to interact in real time with a tutor in the United Kingdom.44 All six of the trainees who completed the feedback questionnaire indicated that the interactive format was more useful than textbook reading for learning the material, and four reported that they felt more confident in describing rashes after completing the tutorial.
This systematic review has several limitations. Given the recent rapid growth in this literature, relevant articles have continued to be published since we conducted our search, as discussed above. In addition, articles identified in our search did not always clearly define the form or content of social media technology used, so some may have been inappropriately excluded from this review. Publication bias favoring articles demonstrating benefits of social media use versus those demonstrating equivalence or negative results must be recognized, as in the context of any systematic review. Finally, the studies included in this review were too heterogeneous to perform sensitivity, subgroup, or meta-analyses.
Despite these limitations, this systematic review offers a foundation for future research and guidance for incorporating social media tools into medical curricula. Future scholarship in this new field should include clear definitions of social media technologies and their components to allow appropriate comparisons and data synthesis. In addition, it would be helpful to compare social media use with other educational methods, explore a variety of learner populations, and examine skill- or behavior-based outcomes. Additional, higher-quality research is needed to establish best practices in the development of social media technology to enhance medical education.
Acknowledgments: The authors would like to thank Cheri Smith, MLS, at Johns Hopkins Bayview Medical Center for assistance in the design of the search strategy; Scott Wright, MD, at Johns Hopkins University School of Medicine for review of an earlier version of the manuscript; and Sarah B. Peskoe, ScM, at the Johns Hopkins University Bloomberg School of Public Health, for assistance with statistical analysis.
Funding/Support: None.
Other disclosures: Dr. Flickinger had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Ethical approval: Not applicable.
Previous presentations: An earlier version of this review was presented as a poster at Medicine 2.0’12, Boston, Massachusetts, September 2012.
References 2. . U.S. Census Bureau. WorldPOP clock projection. http://www.census.gov/population/popclockworld.html. Accessed November 27, 2012 3. . Twitter. What is Twitter? Twitter for business. https://business.twitter.com/basics/what-is-twitter/. Accessed November 27, 2012 4. Gray K, Annabell L, Kennedy G. Medical students’ use of Facebook to support learning: Insights from four case studies. Med Teach. 2010;32:971–976 5. Lee KL, Ho MJ. Online social networking versus medical professionalism. Med Educ. 2011;45:523 6. Sandars J, Morrison C. What is the Net Generation? The challenge for future medical education. Med Teach. 2007;29:85–88 7. McGowan BS, Wasko M, Vartabedian BS, Miller RS, Freiherr DD, Abdolrasulnia M. Understanding the factors that influence the adoption and meaningful use of social media by physicians to share medical information. J Med Internet Res. 2012;14:e117 8. Chu LF, Chan BK. Evolution of Web site design: Implications for medical education on the Internet. Comput Biol Med. 1998;28:459–472 9. Wutoh R, Boren SA, Balas EA. eLearning: A review of Internet-based continuing medical education. J Contin Educ Health Prof. 2004;24:20–30 10. Cook DA, Garside S, Levinson AJ, Dupras DM, Montori VM. What do we mean by Web-based learning? A systematic review of the variability of interventions. Med Educ. 2010;44:765–774 11. Cook DA, Levinson AJ, Garside S, Dupras DM, Erwin PJ, Montori VM. Internet-based learning in the health professions: A meta-analysis. JAMA. 2008;300:1181–1196 12. Ruiz JG, Mintzer MJ, Leipzig RM. The impact of E-learning in medical education. Acad Med. 2006;81:207–212 13. Hughes B, Joshi I, Wareham J. Health 2.0 and Medicine 2.0: Tensions and controversies in the field. J Med Internet Res. 2008;10:e23 14. Eysenbach G. Medicine 2.0: Social networking, collaboration, participation, apomediation, and openness. J Med Internet Res. 2008;10:e22 15. McGee JB, Begg M. What medical educators need to know about “Web 2.0.” Med Teach. 2008;30:164–169 16. Tajer CD. Scientific journals, collective intelligence and digital prosumers. Cardiology in the era of social networks. Rev Argent Microbiol. 2009;77:439–448 17. Larvin M. E-learning in surgical education and training. ANZ J Surg. 2009;79:133–137 18. Gabbard GO, Kassaw KA, Perez-Garcia G. Professional boundaries in the era of the Internet. Acad Psychiatry. 2011;35:168–174 19. Guseh JS, Brendel RW, Brendel DH. Medical professionalism in the age of online social networking. J Med Ethics. 2009;35:584–586 20. Chretien KC, Greysen SR, Chretien JP, Kind T. Online posting of unprofessional content by medical students. JAMA. 2009;302:1309–1315 21. Mansfield SJ, Morrison SG, Stephens HO, et al. Social media and the medical profession. Med J Aust. 2011;194:642–644 22. Association of American Medical Colleges, AAMC Institution for Improving Medical Education.Effective Use of Educational Technology in Medical Education. Colloquium on Educational Technology: Recommendations and Guidelines for Medical Educators. 2007 Washington, DC Association of American Medical Colleges https://members.aamc.org/eweb/upload/Effective%20Use%20of%20Educational.pdf. Accessed February 19, 2013 23. Reed DA, Cook DA, Beckman TJ, Levine RB, Kern DE, Wright SM. Association between funding and quality of published medical education research. JAMA. 2007;298:1002–1009 24. Beckman TJ, Cook DA, Mandrekar JN. What is the validity evidence for assessments of clinical teaching? J Gen Intern Med. 2005;20:1159–1164 25. R Development Core Team. R: A language and environment for statistical computing (version 2.14.1) [computer software]. 2011 Vienna, Austria R Foundation for Statistical Computing http://www.R-project.org. Accessed November 27, 2012 26. Poonawalla T, Wagner RF Jr. Assessment of a blog as a medium for dermatology education. Dermatol Online J. 2006;12:5 27. Chretien K, Goldman E, Faselis C. The reflective writing class blog: Using technology to promote reflection and professional development. J Gen Intern Med. 2008;23:2066–2070 28. Geyer EM, Irish DE. Isolated to integrated: An evolving medical informatics curriculum. Med Ref Serv Q. 2008;27:451–461 29. Raupach T, Muenscher C, Anders S, et al. Web-based collaborative training of clinical reasoning: A randomized trial. Med Teach. 2009;31:e431–e437 30. Carvas M, Imamura M, Hsing W, Dewey-Platt L, Fregni F. An innovative method of global clinical research training using collaborative learning with Web 2.0 tools. Med Teach. 2010;32:270 31. Varga-Atkins T, Dangerfield P, Brigden D. Developing professionalism through the use of wikis: A study with first-year undergraduate medical students. Med Teach. 2010;32:824–829 32. Zolfo M, Iglesias D, Kiyan C, et al. Mobile learning for HIV/AIDS healthcare worker training in resource-limited settings. AIDS Res Ther. 2010;7:35 33. Abate LE, Gomes A, Linton A. Engaging students in active learning: Use of a blog and audience response system. Med Ref Serv Q. 2011;30:12–18 34. Calderon KR, Vij RS, Mattana J, Jhaveri KD. Innovative teaching tools in nephrology. Kidney Int. 2011;79:797–799 35. Dinh M, Tan T, Bein K, Hayman J, Wong YK, Dinh D. Emergency department knowledge management in the age of Web 2.0: Evaluation of a new concept. Emerg Med Australas. 2011;23:46–53 36. Fischer MA, Haley HL, Saarinen CL, Chretien KC. Comparison of blogged and written reflections in two medicine clerkships. Med Educ. 2011;45:166–175 37. George DR, Dellasega C. Use of social media in graduate-level medical humanities education: Two pilot studies from Penn State College of Medicine. Med Teach. 2011;33:e429–e434 38. Rosenthal S, Howard B, Schlussel YR, et al. Humanism at heart: Preserving empathy in third-year medical students. Acad Med. 2011;86:350–358 39. Triola MM, Holloway WJ. Enhanced virtual microscopy for collaborative education. BMC Med Educ. 2011;11:4 40. Mollett A, Moran D, Dunleavy P Using Twitter in University Research, Teaching and Impact Activities: A Guide for Academics and Researchers. 2011 London, UK London School of Economics and Political Science, LSE Public Policy Group 41. Priem J, Costello KL. How and why scholars cite on Twitter. Proc Am Soc Inf Sci Technol. 2010;47(1):1–4 42. Mandavilli A. Peer review: Trial by Twitter. Nature. 2011;469:286–287 43. Bahner DP, Adkins E, Patel N, Donley C, Nagel R, Kman NE. How we use social media to supplement a novel curriculum in medical education. Med Teach. 2012;34:439–444 44. Ali FR, Bowen JS, Strachan JM, Handuleh J, Finlayson AE. Letter: Real-time, intercontinental dermatology teaching of trainee physicians in Somaliland using a dedicated social networking portal. Dermatol Online J. 2012;18:16
留言 (0)