1 INTRODUCTION
Studies estimate that approximately 25 million individuals worldwide, including one million people in the United States, identify as transgender.1-4 In recent years, more widespread access to surgery and improved insurance coverage have resulted in increasing numbers of transgender individuals pursuing surgical interventions.5 In a 2019 study, 28% of transgender women reported undergoing gender-affirming surgical procedures, with 5−13% of these surgeries involving genital surgery.6 Of the transgender women who had not undergone gender-affirming surgery, 45–54% of individuals reported that they hope to do so in the future.6
For many individuals, gender-affirming surgery helps to alleviate gender dysphoria and improve quality of life. Gender-affirming surgery is generally safe, effective, and medically necessary. Although complications can occur, many are self-limited and are commensurate with complication rates of complex genitourinary reconstruction performed for other diagnoses (ie, oncological and congenital).7-13 This article will provide a thorough analysis of post-operative outcomes following penile inversion vaginoplasty, including topics related to patient satisfaction and adverse events.
2 PENILE INVERSION VAGINOPLASTY
When reviewing the literature and assessing the data pertaining to vaginoplasty, it is important to recognize that surgical techniques vary between surgeons. In addition, terminology used to describe procedures and/or complications and outcomes also differs. Vaginoplasty typically involves penectomy, orchiectomy, clitoroplasty, vulvoplasty, and the construction of a vaginal canal. Most often, the surgical goals include a cosmetically appealing and sensate vulva and clitoris, and a vagina capable of receptive intercourse. Various surgical techniques are used to create the vagina and its lining, with the most common being a skin-lined neovagina. Other methods include pedicled intestinal flaps, skin grafts from other anatomic sites (abdomen, flanks, buttocks, etc.), and/or peritoneal tissue. The penile inversion vaginoplasty is generally favored by most surgeons and involves the use of penile skin flaps often in conjunction with supplemental scrotal skin grafts.14-17 This article focuses on penile inversion vaginoplasty.
3 COMPLICATIONS FOLLOWING VAGINOPLASTY
Rates of complications following penile inversion vaginoplasty range from 20% to 70%,18-25 with most complications occurring within the first four months after surgery.19, 23 Most complications are minor and self-limited in nature, (ie, minor wound healing disruptions) and are managed non-operatively or with minor secondary surgical procedures.23, 24, 26 Ferrando reported that greater than 50% of the complications occurring during the first 30 days following vaginoplasty consisted of dehiscence or separation of the surgical incision.24 Massie et al20 cite granulation tissue as the most common minor post-operative complication (26% of patients). Ives et al22 noted that 35.6% of their complications were minor. However, their definition of “minor complication” included rectal or urethral injury managed intraoperatively without further sequalae (in the opinion of the senior author, these complications are not considered minor). Ferrando and Whynott did not find an association between surgeon experience and complications that occurred in the immediate post-operative period; the authors postulated that early complications are “common and inherent” to the procedure.24, 27
Most studies show that the rate of serious complications following vaginoplasty is low and comparable to complications of other genitourinary reconstruction surgeries.17, 19, 23, 24 Reported rates of adverse intraoperative complications, such as rectal or genitourinary injury or need for intraoperative blood transfusion, range from 1.5% to 2.6%.19, 24 Ives et al22 reported major complications in 16.8% of their patients, with 5% of patients requiring reoperation for bleeding, 7.9% requiring reoperation for wound complications, 2% requiring readmission without reoperation, and 1% developing a venous thromboembolism (VTE). Their relatively high complication rate may be attributable to their broader inclusion criteria for “major complication” compared with other authors. Gaither et al19 reported no complications greater than Clavien-Dindo IIIB. They concluded that vaginoplasty is considered a safe operation.19
3.1 Predicting complications
When assessing preoperative risk factors, several studies have shown that age, body mass index (BMI), diabetes, and smoking history are associated with complications following vaginoplasty.15, 20 In contrast, Ives et al22 found that these risk factors were not associated with major, minor, total, or urethral complications following vaginoplasty, but the study lacked power because of a relatively small sample size (101 transgender women).
Data suggest that non-compliance with post-operative protocols, including dilation instructions and activity restrictions, has been associated with post-operative complications both 30 and 90 days after surgery.23 Levy et al. reported that non-compliance was the only factor that reached statistical significance when examining rates of revision and reoperation.23 Below is a discussion of the main complications of vaginoplasty (Table 1).
TABLE 1.
Common complications of penile inversion vaginoplasty, the reported incidence of each complication in the literature, and management options
Complication
Incidence
Management options
Minor wound healing issues
3.3–33%
19,
22-
25,
27-
32
Local wound care
32
Tissue necrosis
0.6–24.6%
15,
27,
32,
33
Local wound care, surgical debridement
28,
32
Granulation tissue
7–26%
19,
20,
27,
30,
32
Silver nitrate
32
Infection
0–27%
15,
20,
22,
24-
27,
30,
34
Antibiotics, surgical drainage, suture removal
15,
26,
28
Neovaginal stenosis
0–12%
14,
15,
18,
20,
23,
24,
26-
32,
36
Dilation, lateral wall incisions, Z-plasty, revision with recreation of the neovaginal canal, and re-lining with new graft or local flap
28,
29,
32,
42
Introital stenosis
2.5–15%
14,
15,
20,
24,
28,
32
Dilation, surgical revision
28,
42
Inadequate vaginal depth
0–12%
14,
26,
28,
29,
32,
37
Revision procedure with skin grafting or local flap
28,
32
Neovaginal prolapse
0–5%
14,
15,
20,
23-
28,
32,
34,
36,
37,
39
Sacrocolpopexy, reinsertion of neovagina with fibrin glue
28,
32
Excessive post-operative bleeding
3.2–12%
14,
29,
31,
32,
35,
39
Blood transfusion, conservative management, operative exploration
29,
42
Hematoma
1.6–21%
15,
20,
23,
27,
28,
30,
32,
35
Pressure dressings, local cooling, operative evacuation
27,
28,
37
Pelvic and/or genital pain
1.3–20%
14,
20,
24,
28,
32,
36
Topical anesthetic, neuropathic oral pain medications, pain management specialist referral, physical therapy
28,
42
Dyspareunia
2–8%
20,
28,
30
Larger dilators, relaxation techniques, physiotherapy
28,
32,
45
Secondary operation for cosmetic revision
20–54.2%
14,
18,
20,
29,
30,
32,
39
Labiaplasty/labial reduction, labial lipofilling, clitoral repositioning, clitoral hood reduction, perineoplasty, scar revision
18,
27,
29,
30,
37
Loss of clitoral sensation
2.7%
26
Conservative management
Clitoral necrosis
0.5–3%
14,
28,
30,
34,
36,
37
Local wound care
32
Clitoral hypersensitivity
1–14%
20,
26,
28
Topical anesthetic, conservative management, excision of neoclitoris
26,
28
Divergent/spraying urinary stream
5.6–33%
15,
24,
26,
27,
36
Conservative management, secondary urethroplasty
22
Urinary tract infection
4.4–7%
15,
20,
30
Antibiotics
15
Urinary incontinence
4–16%
28,
39,
47
Conservative management, pelvic floor physiotherapy, anticholinergics, bulking of the bladder neck
28,
39
Urethral or meatal stenosis
0–6%
19,
20,
23,
25,
27,
30,
31
Urethral dilation, urethroplasty, meatotomy, V-Y meatoplasty
28,
42
Urinary retention
0–12.8%
15,
20,
24,
25
Conservative management with dilation versus versus urgent decompression with suprapubic or urethral catheterization paired with urethroplasty or meatoplasty
28,
32
Urethral injury
0–1.1%
15,
20,
24,
30
Surgical repair
28
Urethroneovaginal fistula
0–4%
15,
19,
24,
25,
28,
34,
37
Fistula resection with primary closure versus tissue interposition
32
Rectal injury
0–6.7%
15,
18-
20,
23-
31,
34,
37,
39,
48
Primary closure, colostomy if severe
28
Rectoneovaginal fistula
0–17%
15,
19,
20,
23,
24,
28-
30,
32,
36,
38,
39,
48,
49
Fistula resection with primary closure versus tissue mobilization and interposition (eg, omentum); if minor, conservative management with low residual diet; if severe, colostomy and trans-neovaginal reconstruction
28,
32,
42
Venous thromboembolism
0–6%
15,
19,
26,
37,
54
Risk reduction with minimizing operative time, sequential compression devices, early post-operative ambulation, and chemoprophylaxis; perioperative hormone cessation controversial
87
3.2 Wound disruption and tissue loss
Minor wound healing issues are commonly reported following vaginoplasty (range 3.3%–33%),19, 22-25, 27-32 and many resolve without the need for surgical intervention.23 Wound dehiscence, especially in areas of increased tissue tension (ie, introitus and labia majora),28 most commonly occurs within the first month following surgery.19, 32 Ferrando reported that of the 17% of their patients (n = 76 patients) who experienced complications, more than 50% of these complications involved wound dehiscence or wound separation.24 Despite this, none of the patients experienced serious sequelae.24 Most studies consistently report that post-operative wound dehiscence is treated with local wound care and do not require surgical intervention.28, 29, 32
Tissue loss may be associated with wound dehiscence, and most often occurs at points of maximum tissue tension, such as at the vaginal introitus.20 The reported incidence of tissue necrosis ranges from 0.6% to 24.6%,15, 27, 32, 33 with minor tissue necrosis (ie, resolved without reoperation under general anesthesia) accounting for the higher reported incidence in some studies.15 Minor cases of tissue necrosis can often be treated with local wound care,32 whereas more major tissue loss may require surgical debridement.28 Massie et al20 noted their most common major complication (17%) was tissue necrosis along the inferior wound edge. Whynott et al27 reported that of the patients who required reoperation, 25% were related to tissue necrosis. Preoperative patient optimization (ie, smoking cessation, diabetic control, and cardiopulmonary status) is important, as these co-occurring conditions may be independent predictors of post-operative tissue necrosis.20, 32
3.3 Granulation tissue
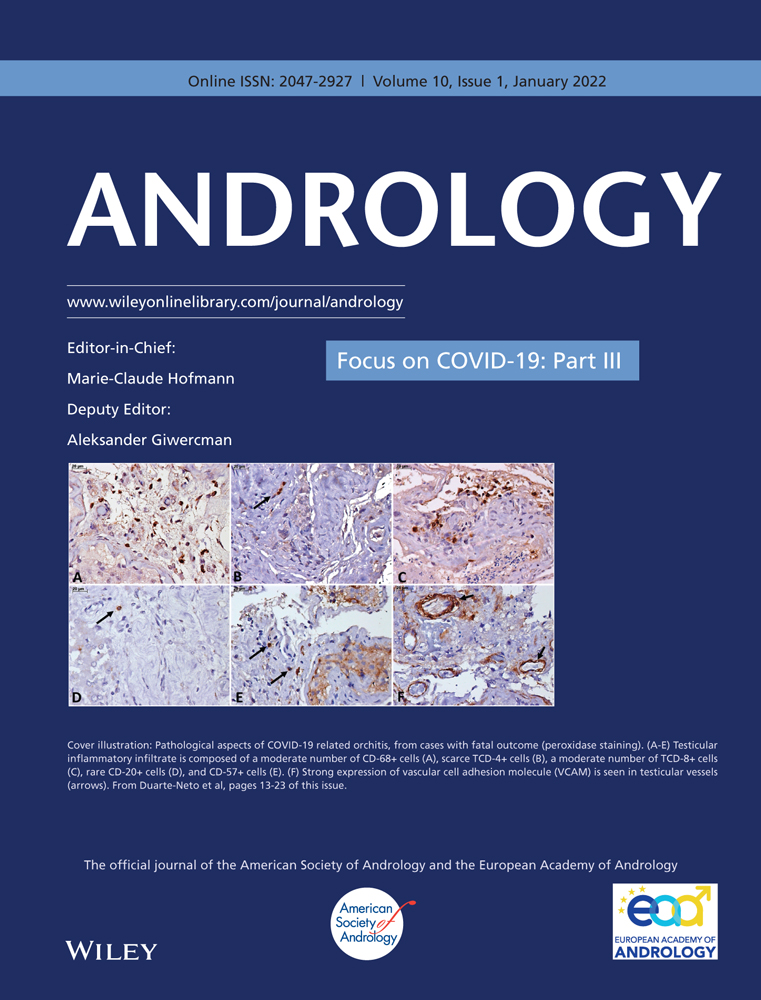
Granulation tissue, either of the perineum or within the neovagina, is common after vaginoplasty (Figure 1).19-21, 32 The incidence ranges from 7% to 26%19, 20, 27, 30,

留言 (0)