
記住我

Rasmussen encephalitis (RE) is a progressive destructive disease of one cerebral hemisphere, characterized by drug-resistant focal epilepsy, progressive hemiplegia, and cognitive decline, as well as unihemispheric brain atrophy.1 This disorder is rare and mostly affects children. The peak of disease manifestation has been said to be 6 years of age.2 The term “encephalitis” indicates that immune cells infiltrate the brains of patients with active disease. Neuropathological studies of brain tissue obtained during surgery for intractable epilepsy have consistently revealed microglial activation and infiltration of round cells. These were later identified to be cytotoxic T cells directed toward neurons and astrocytes.1, 3-6 Neuroimaging studies show the sequence from magnetic resonance imaging (MRI) volume and T2/fluid-attenuated inversion recovery signal increase to atrophy and, on positron emission tomography, from hypermetabolism to hypometabolism. Such a course is typical for destructive brain inflammation.7-9 In many cases, the cerebrospinal fluid harbors cells above the normal limit, oligoclonal bands, and increased CD4+ T-cell numbers as well as elevated concentrations of tumor necrosis factor α and granzyme B.10-12 The cause of the chronic encephalitis remains unknown. A unilateral virus infection and genetic factors have been suggested as key elements in this unihemispheric disease.2
Authorities in the field have repeatedly stated that RE manifests itself in previously normal children.13-15 None of the three cases of the original description had any abnormalities prior to manifestation of the disease.1 However, in the large Montreal series (N = 48), nine patients had perinatal complications (19%), suggesting a higher burden of early problems than often assumed.16
The etiologies of brain diseases and epilepsies are often multifactorial. Genetic and environmental factors might put an individual at an increased risk of developing an inflammatory brain disease. We hypothesized that this might be the case in RE.
Here, we present a large group of 160 RE cases with demographic data and detailed information on their early history. This large number of patients offers the possibility to detect potential predisposing factors in RE patients beyond those found in other epilepsies. Therefore, we compare the RE cases to 154 patients with genetic generalized epilepsy (GGE) and 148 patients with focal cortical dysplasia (FCD) Type II.
2 MATERIALS AND METHODS 2.1 Patients with REWe retrospectively analyzed data of 244 patients with RE. Data of 160 patients were sufficiently detailed to be used for this study. Only cases and controls with data available on age at disease onset, sex, affected hemisphere, pre- and perinatal history, concomitant disease, and MRI findings were included in the study. These were patients of the Epilepsy Center Bethel, Bielefeld, Germany (n = 63), the Department of Epileptology of the University of Bonn, Germany (n = 27), or both centers (n = 30), investigated between 1991 and 2020. They were born between 1948 and 2017, mean 1996, median 1999. For the remaining cases, medical reports or file notes were sent to one of the authors (C.G.B.) to confirm the diagnosis or to obtain advice for patients’ management (n = 40). In all cases, RE was diagnosed according to the current European consensus criteria17 including Olson's addition (two Part A criteria plus criterion B3, i.e., a positive histopathology).18 The series includes surgical and nonsurgical cases; 41 patients underwent hemispherotomy, and a further nine patients lesionectomy, partial resections, or disconnections; the remaining 110 patients were not operated on.
2.2 Patients with GGEWe retrospectively analyzed the data of 154 patients with GGE. All patients with a diagnosis of GGE who were admitted to the Epilepsy Center Bethel, Bielefeld, Germany, between January 2018 and April 2020 were included. They were born between 1996 and 2012, mean 2002, median 2001. Patients born later than 2012 mainly did not fulfill the inclusion criteria. Often, they had Dravet syndrome or genetic syndromes accompanied by brain malformation, or their etiologies have not yet been clarified. Therefore, they were not considered for this study. Syndromic diagnoses were taken from the final medical reports: childhood absence epilepsy (n = 25), juvenile absence epilepsy (JAE; n = 23), absence epilepsy not further specified (n = 6), juvenile myoclonic epilepsy (JME; n = 33), genetic generalized epilepsy with generalized seizures alone (n = 16), genetic generalized epilepsy with grand mal on awakening (n = 2), epilepsy with eyelid myoclonia/Jeavons syndrome (n = 7), generalized epilepsy with febrile seizures plus (GEFS+; n = 6), myoclonic epilepsy of infancy (n = 1), myoclonic astatic epilepsy (n = 3), and GGE not further specified (n = 32).
2.3 Patients with FCDWe retrospectively analyzed data of 148 patients with FCD Type II. All patients who underwent presurgical assessment at the Epilepsy Center Bethel, Bielefeld, Germany, between January 2017 and December 2020 with a final diagnosis of FCD Type II and sufficiently detailed information were included. Patients were born between 1959 and 2018, mean 1996, median 1998. The diagnosis of FCD Type II was histologically confirmed after epilepsy surgery (n = 114) or diagnosed by MRI criteria (n = 34; blurred gray–white matter transition, cortical thickening, and transmantle sign, i.e., FCD IIB).
2.4 Analyzed parameters S.F. extracted all data from the patients´ medical reports and file notes, which were accessible in full to all authors from Mara Hospital. In a descriptive manner, we characterized the three groups regarding these demographic and laterality parameters: Age at disease onset. “Onset” was defined as the point in time that the treating clinicians considered the best approximation of the first signs of the disease; in the GGE and FCD patients, it was the date of the first seizure. Age is given in years as whole numbers (first year of life = 1, second year of life = 2, and so on). Sex. Affected hemisphere. In the RE cases, this was the one with dominant atrophy, producing the dominant lateralizing semiological elements and the dominant abnormal electroencephalographic features. No patient was diagnosed as having bilateral disease. Single cases did not become seizure-free despite anatomical or complete functional hemispherectomy (according to postoperative MRI). In these cases, it remains open whether they had bilateral (even though asymmetrical) RE or whether they had developed a secondary independent epileptic focus in the contralateral hemisphere. In the FCD cases, this was the hemisphere harboring the lesion. In the GGE patients, no affected hemisphere was noted. As potential risk factors, we studied the following parameters: Acquired factors: o At least one of the following pre- or perinatal problems: twin pregnancy premature birth (≤36 weeks) comorbid early acquired intracerebral lesions, documented by MRI and not specifically related to RE o Fever-associated disease onset (maximal latency 1 month). This was not evaluated in the GGE group because it could not be clearly separated in these conditions (e.g., in GEFS+). o Febrile seizures (febrile convulsions years before the epilepsy started). Genetic factors a Autoimmune diathesis: history of autoimmune diseases and allergies as documented in the medical records 2.5 Statistical analyses, ethicsPearson chi-squared test was used to compare the potential risk factors between patients with RE, GGE, and FCD (IBM SPSS Statistics Subscription 11–2018). To account for six tests, the significance level of p < .05 was corrected to p < .008 according to Bonferroni.
For this retrospective report of patients studied personally by the authors, informed consent from the patients or their representatives was waived by the ethics committee in Münster (MS 2017-431-f-S) in accordance with the Health Data Protection Law of the Federal State of North Rhine Westphalia.
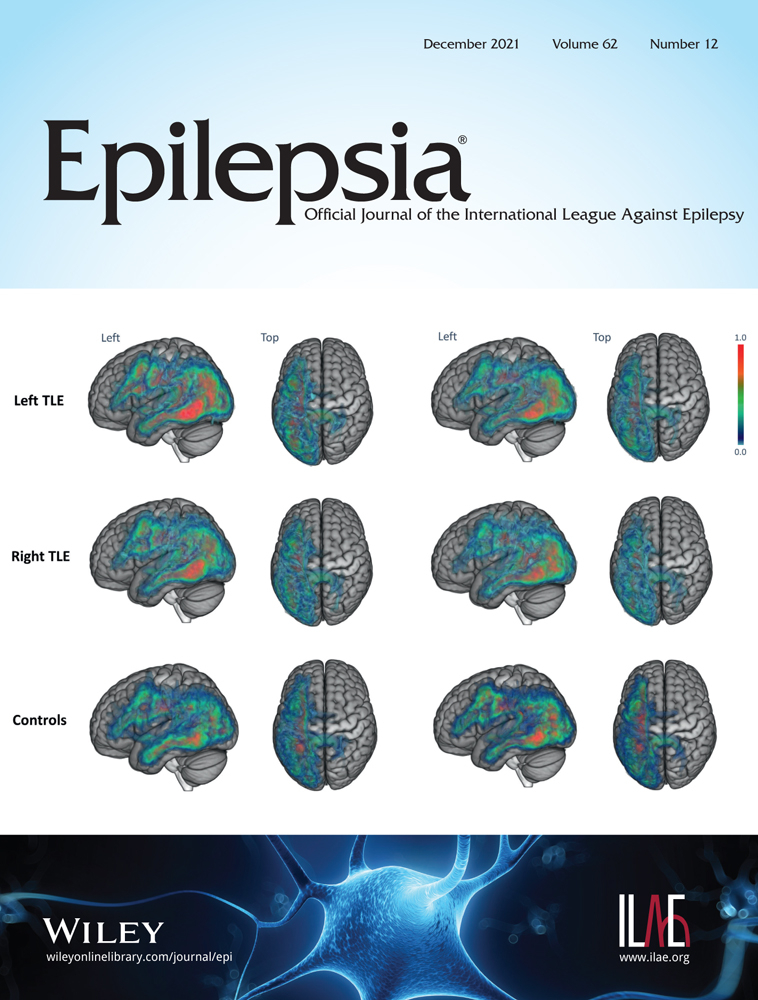
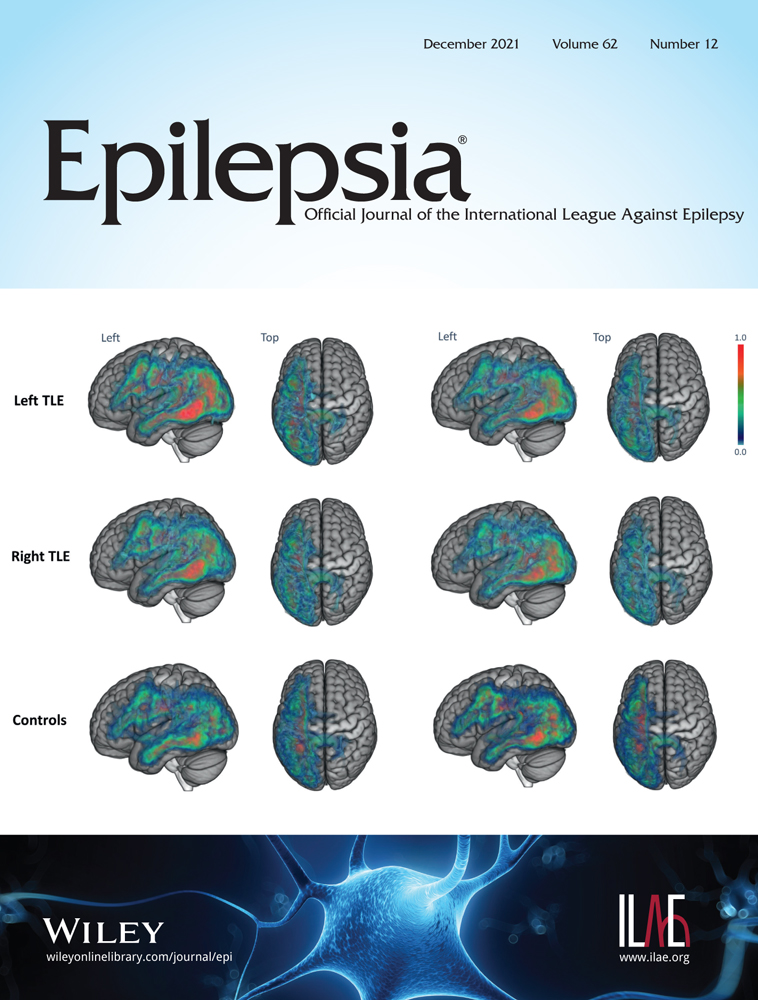
3 RESULTS 3.1 Age at onset, sex distribution, affected hemispheresAge at symptom onset ranged from 1 to 53 years, median 7 years, mean 10 years. The patients were younger than those with GGE and older than those with FCD at disease manifestation (Table 1, Figure 1). Females were more frequently affected in both RE and GGE (58.1% and 55.8%, respectively). In FCD patients, there were slightly more males (52.0%). The sex distribution in RE was not the same across all age groups. In patients with onset before the age of 7 years, it was balanced. In patients with later onset (>7 years), females predominated (female:male = 54:25 = 2.2:1). A similar age-related sex distribution was seen in our GGE group. The female sex predominated in patients with seizure onset between 10 to 17 years (female:male = 56:34 = 1.6:1). In this age group, the syndromes JME and JAE were common. In FCD patients, sex distribution was not age related (Figure 1). In the RE group, the left hemisphere was more often affected (65.6%) than in FCD patients (46.6%).
TABLE 1. Age at symptom onset, affected hemispheres, and sex distribution Characteristic RE, n = 160 GGE, n = 154 FCD, n = 148 Age, years Median 7 12 4 Mean, SD 10 ± 8 10 ± 5 6 ± 7 Range 1–53 1–21 0–50 Left hemisphere 105 (65.6%) – 69 (46.6%) Female sex 93 (58.1%) 86 (55.8%) 71 (48.0%) Abbreviations: FCD, focal cortical dysplasia; GGE, genetic generalized epilepsy; RE, Rasmussen encephalitis.
Age and sex at symptom onset. FCD, focal cortical dysplasia; GGE, genetic generalized epilepsy; RE, Rasmussen encephalitis
3.2 Potential risk factorsDetailed data are given in Table 2.
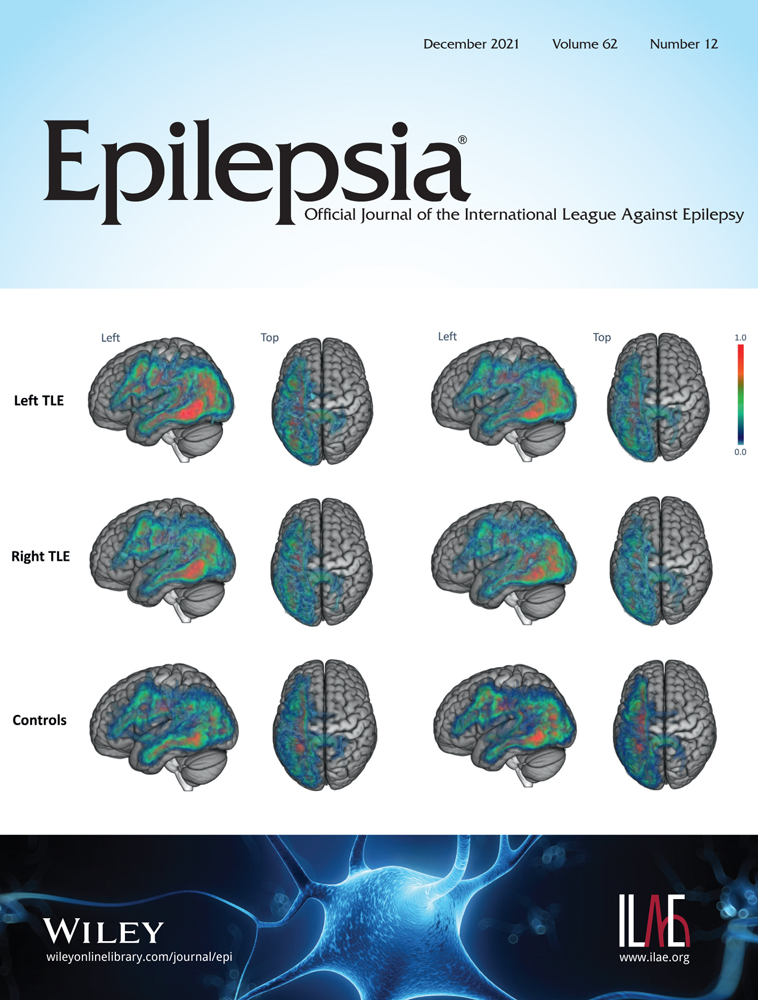
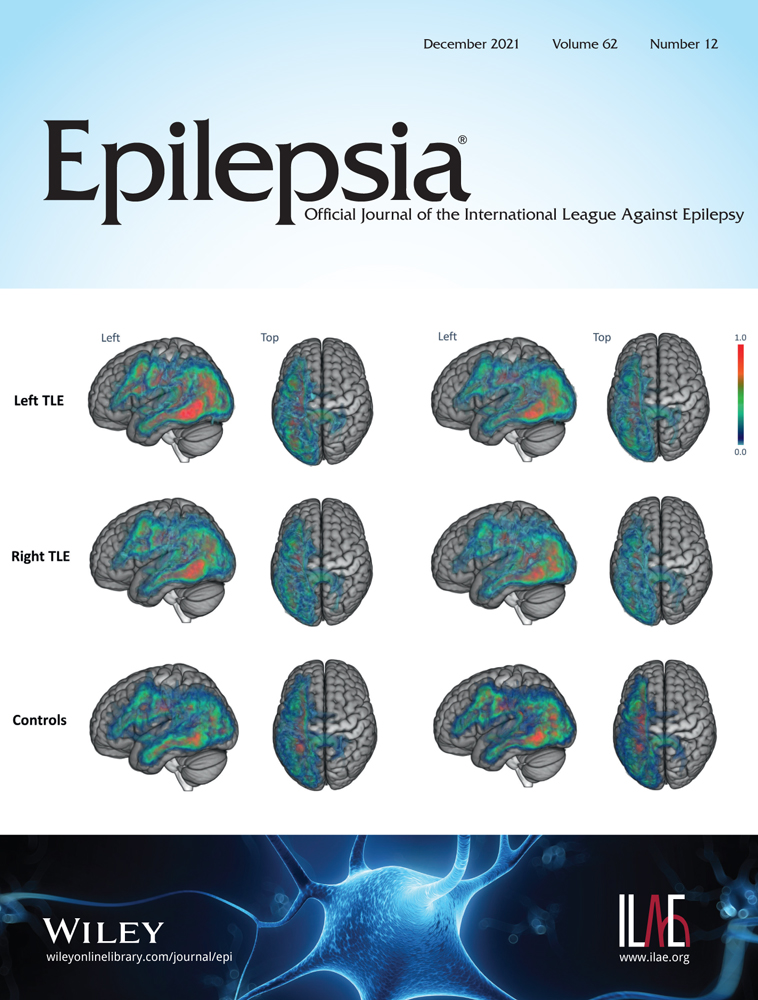
TABLE 2. Potential predisposing factors in RE patients compared to GGE and FCD patients Factor RE, n = 160 GGE, n = 154 FCD, n = 148 Acquired factors Early pre- or perinatal problems 26 (16.3%) 5 (3.2%) <.001a 4 (2.7%) <.001a Fever-associated disease manifestation 24 (15.0%) –b –b 0 <.001a Febrile seizure 5 (3.1%) 21 (13.6%) .001a 5 (3.4%) .576 Genetic factors Autoimmune diathesis 39 (24.4%) 37 (24.0%) .942 26 (17.6%) .208 Abbrevations: FCD, focal cortical dysplasia; GGE, genetic generalized epilepsy; RE, Rasmussen encephalitis. a Significant after Bonferroni correction (p < .008). b See Materials and Methods section for explanation. 3.2.1 Early pre- or perinatal problemsEarly pre- or perinatal problems were significantly more frequent in RE than in GGE or FCD patients. More specifically, twin pregnancies were reported in 12 RE patients (7.5%), whereas there were no twins in the FCD group and only three (1.9%) in the GGE group. Early comorbid structural lesions were seen on MRI in 12 (7.5%) RE patients, which was more common than in GGE (n = 1, .6%) or FCD (n = 3, 2.0%). The etiology of comorbid lesions in RE patients was as follows: ipsilateral peri- or intraventricular pre-/peripartal bleeding (n = 3), ipsilateral small paraventricular infarction (n = 2), ipsilateral enlarged lateral ventricle with peripartal hypoxia (n = 2), ipsilateral cerebellar cortical defects (n = 2), bilateral periventricular leukoencephalopathy (n = 2), and sagittal craniosynostosis (n = 1). Figure 2 depicts examples of patients with early comorbid lesions. Sometimes, the clinical history supported the presence of the lesion very early in life, years before RE manifestation. An example is given in the legend to Figure 2C,D, Patient 23. Interestingly, in nine patients with lateralized lesions, all the lesions were in the same hemisphere as the encephalitis (the other three lesions were bilateral).

Examples of early comorbid lesions. Patient 64: This male patient has suffered from left-hemispheric Rasmussen encephalitis (RE) since he was 6 years old. (A) First magnetic resonance imaging (MRI) was performed 1 month after epilepsy (i.e., RE) manifestation. It showed an old left cerebellar gliotic defect (large arrow) and a small hyperintense lesion in the left posterior putamen (small arrow). (B) Three years later, there was a distinct atrophy with increased T2 signal of the left striatum (small arrows) and the left pallium. The gliotic cerebellar lesion (large arrow) was unchanged during the complete follow-up. Patient 23: After a complicated pregnancy, this female patient was born at term. At the age of 8 weeks, pyramidal tract signs with right-sided pathologically increased muscle reflexes became evident. Moreover, language development was delayed from the beginning. (C) An MRI was performed at the age of 4 years with epilepsy onset (i.e., left-sided RE) and already showed a shrunken putamen on the left side, predominantly in the posterior part (large arrow); the claustrum was no longer discernable (small arrow). In the following years, she developed a progressive right-sided hemiparesis. (D) At the age of 14 years, MRI showed a loss of the striatum (caudate nucleus and putamen) and a perisylvian atrophy (small arrows) on the left. Moreover, left-hemispheric atrophy (large arrows) was seen
3.2.2 Fever-associated disease onsetFever-associated disease manifestation was significantly more common in RE than in FCD patients. In RE patients, we observed a decreasing frequency of febrile onset with increasing age at onset (ages 1–6 years: febrile onset in 15/68 [22%]; ages 7–15: febrile onset in 8/70 [11%]; ages 16–53: febrile onset in 1/22 [5%]).
3.2.3 Febrile seizuresIn the RE patients, febrile seizures (years before disease manifestation) were reported in only five patients (3.1%). There was no significant difference compared with FCD patients. The proportion of 3% lies within the 2%–5% range of the incidence of febrile seizures in the Western world.19 By contrast, significantly more GGE patients (21/154, 13.6%) had febrile seizures.
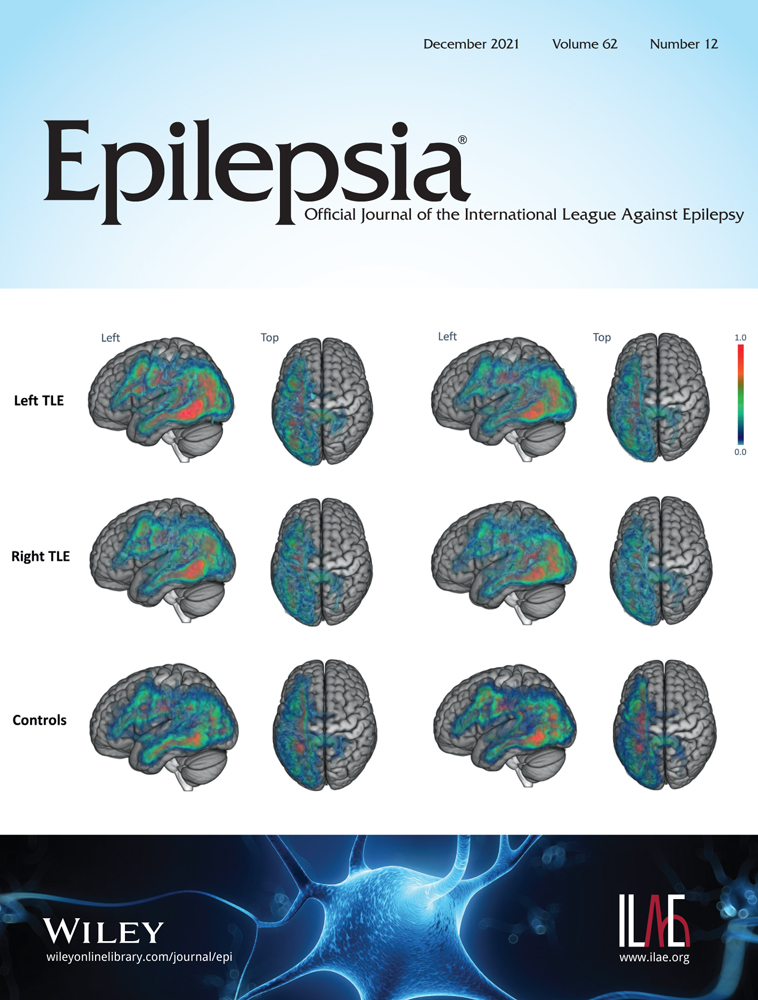
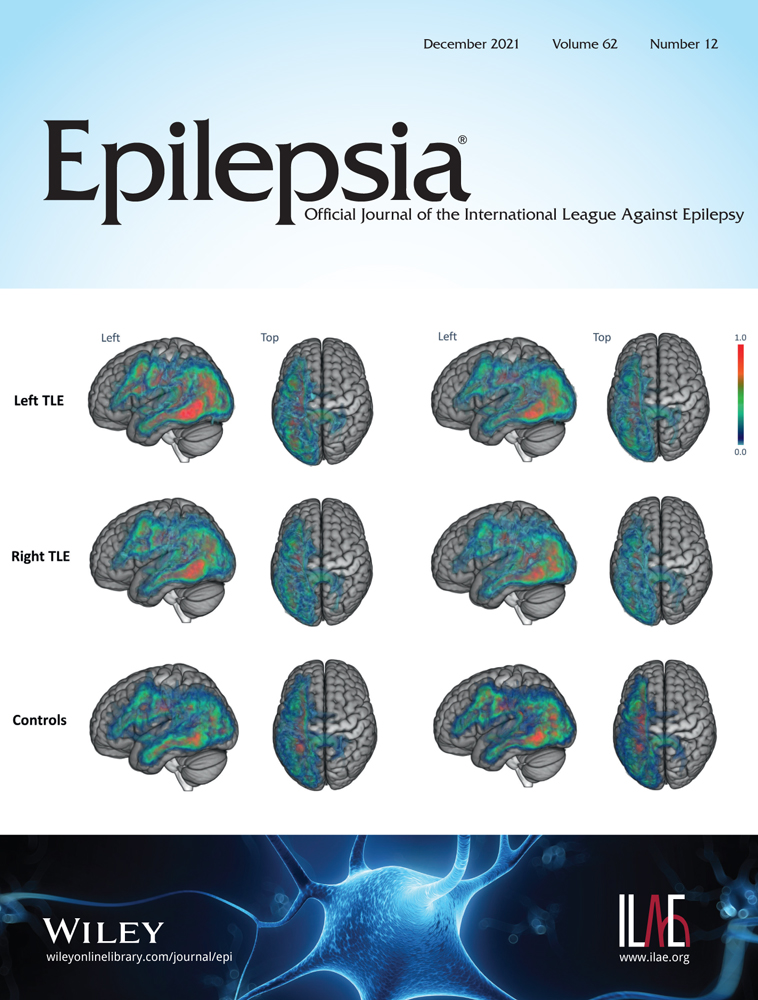
3.2.4 Autoimmune diathesisOverall, there was no significant difference in the frequency of autoimmune diseases or allergies in general between the different groups. However, scleroderma en coup de sabre (n = 9), uveitis (n = 1), and chorioretinitis (n = 1) were seen exclusively in 11 RE patients (6.8%). These lateralized conditions occurred ipsilaterally to the hemisphere affected by RE in all cases. They always preceded the cerebral manifestation. Patients with scleroderma en coup de sabre often had additional ipsilateral facial atrophy (Parry–Romberg syndrome). The scleroderma patients were characterized by a late onset of cerebral symptoms (between 7 and 12 years).
Figure 3 shows a patient with scleroderma en coup de sabre, ipsilateral T-cell-dominated encephalitis, and progressive cerebral hemiatrophy.

Example of comorbid facial autoimmune condition. Patient 148: In this male patient, right-hemispheric Rasmussen encephalitis manifested itself at age 22 years. (A) At the age of 10 years, he developed scleroderma en coup de sabre with right-sided lateralization (the scarlike lesion bulges out to the right at the superior end and terminates at the medial aspect of the right eyebrow, arrows). (B) Magnetic resonance imaging (MRI) at the age of 23 years showed a right temporo-occipital lesion. After lesionectomy, histology showed T-lymphocytic infiltrates. (C) The MRI after lesionectomy at the age of 24 years revealed no clear atrophy. (D) At the age of 39 years, right-sided hemiatrophy is discernable
3.3 Combinations of potential predisposing factorsPerinatal complications, facial autoimmunity, and a fever-associated disease onset occurred isolated in 42 and in combination in 11 patients. Altogether, there were 53 of 160 RE patients with potential predisposing factors (33.1%). Table 3 summarizes the patients with comorbidity factors.
TABLE 3. Summary of Rasmussen encephalitis patients with potential risk factors Patient ID Age at onset, years Scleroderma (S)/uveitis (U)/chorioretinitis (C) Twins Premature birth, ≤36 weeks Structural early brain lesion Fever-associated disease onset or infection 1 1 + 3 1 + 4 2 + 14 3 + (U) + 16 3 + + + + 18 3 + + + + 19 3 + 20 3 + 21 3 + + + 23 4 + + 27 4 + + + 32 4 + + + 34 4 + 37 4 + 39 4 + 43 5 + 46 5 + 49 5 + 50 5 + 51 5 + 54 5 + 55 6 + 57 6 + 59 6 + + 60 6 + 64 6 + 70 7 + 73 7 + 75 7 + (S) 82 8 + 87 8 + 88 8 + 89 8 + 95 9 + 96 9 + 103 9 + (S) 105 9 + 107 9 + 111 10 + 112 10 + (S) 116 11 + 117 11 + (S) + + 122 11 + (S) 123 11 + 128 13 + 131 14 + + 135 14 + (S) 136 15 + 141 18 + + 148
留言 (0)