
記住我
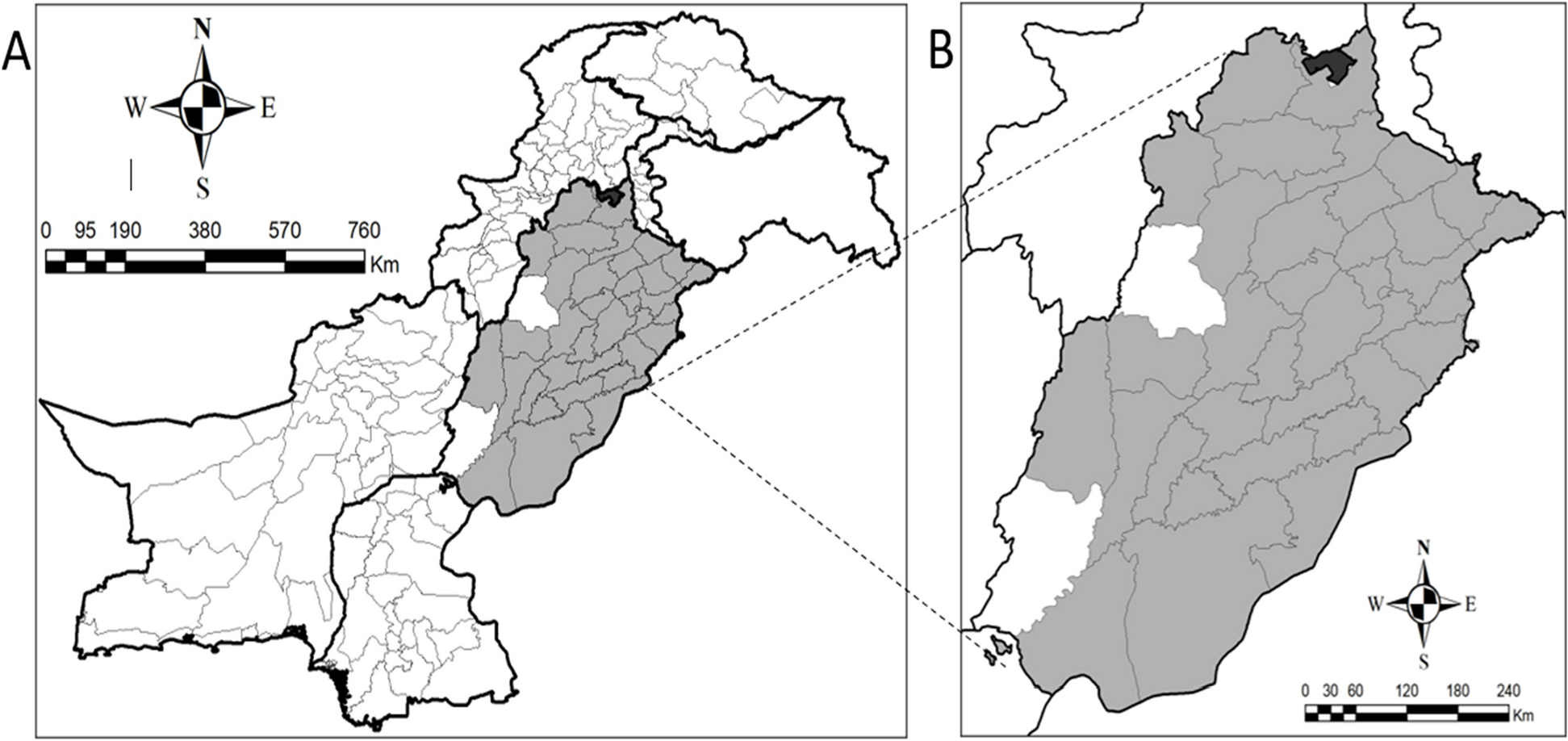

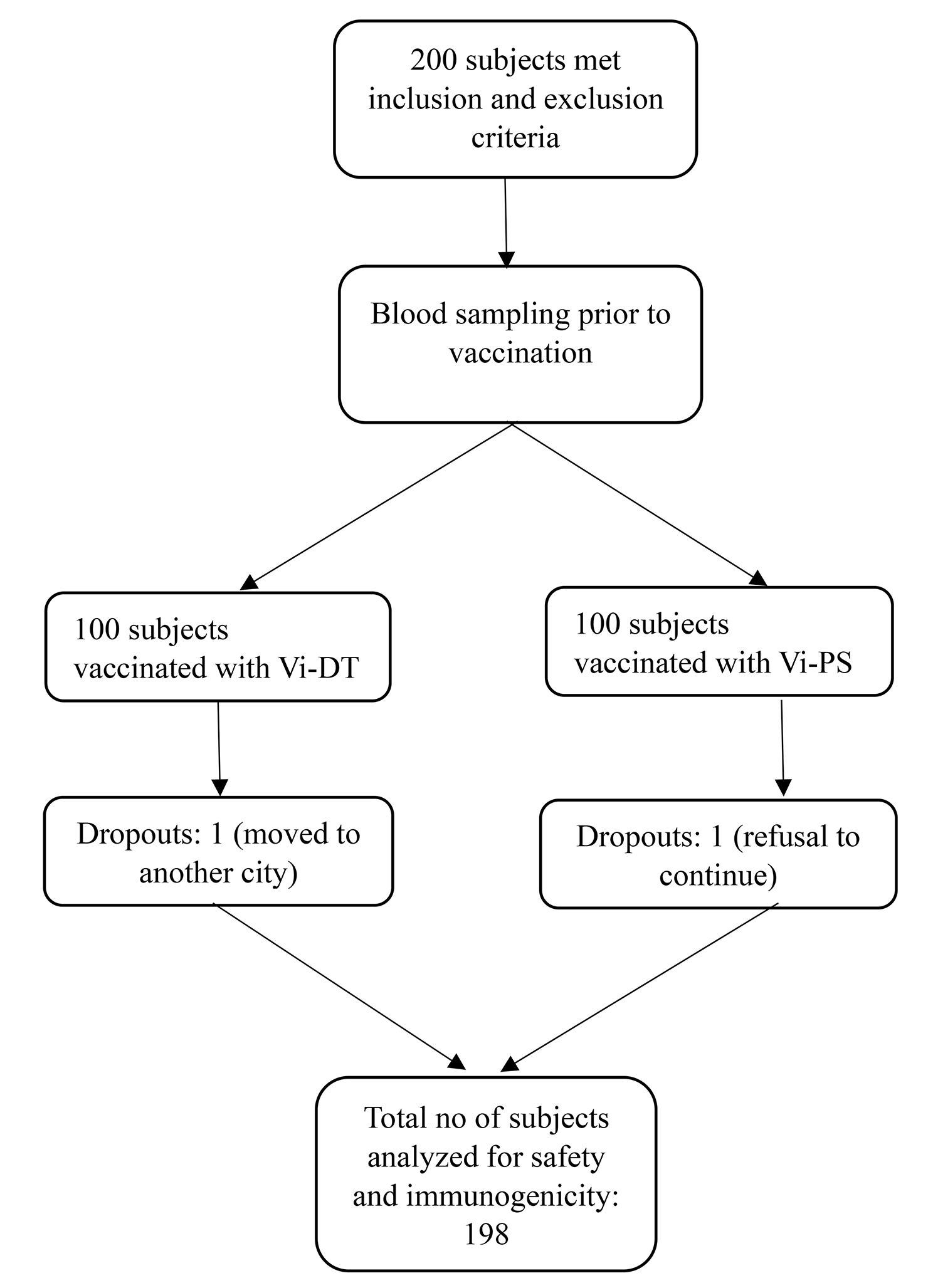

The total number of participating travelers in the study was 411. Data were then rechecked and validated; 12 travelers were excluded because they had traveled back to Thailand for > 90 days. Therefore, a total of 399 participants were included for data analysis. The site of data collection is displayed in Additional file 1.
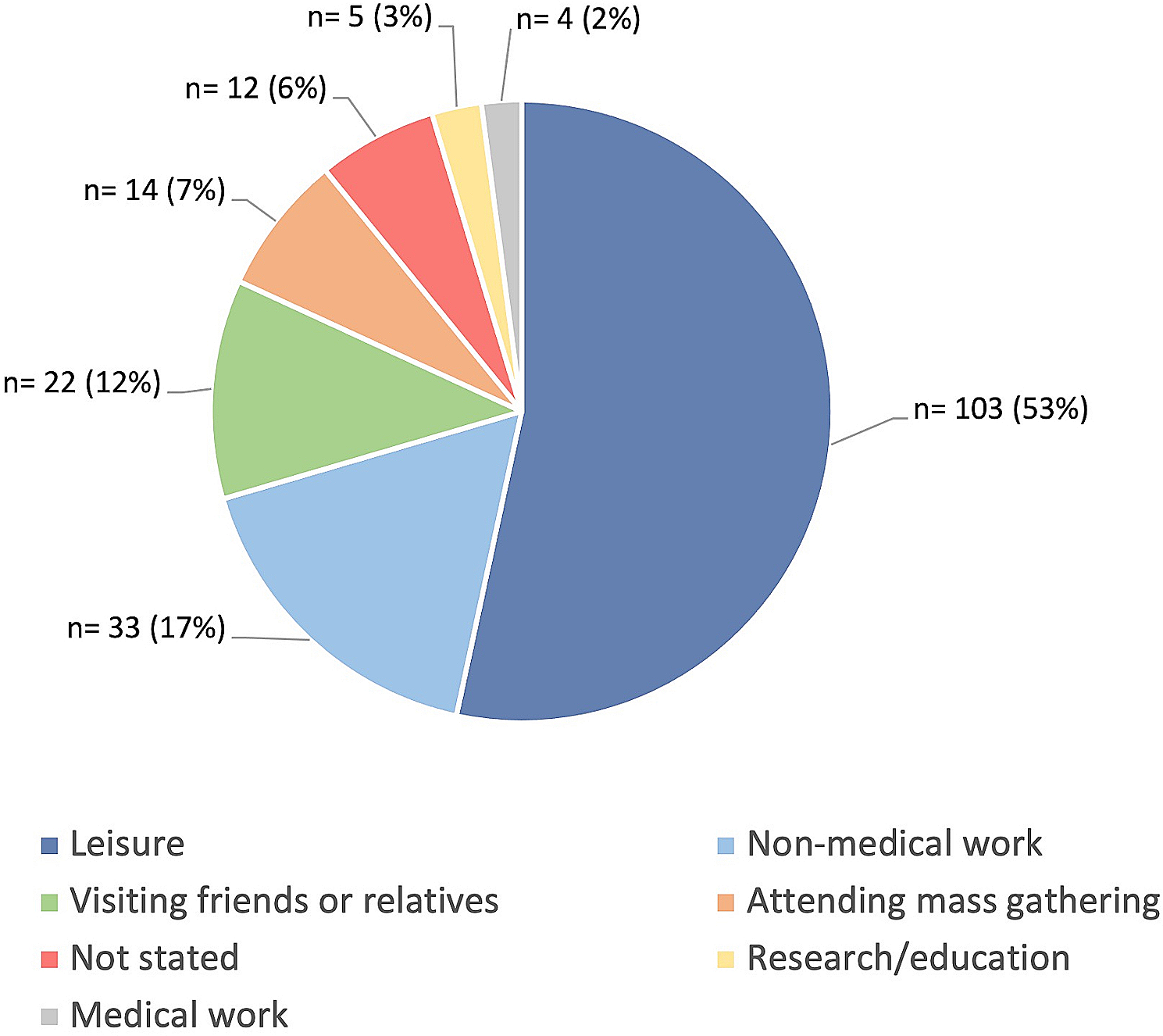
General characteristics of participants and their travelsOf the 399 participants, 224 (56.1%) participants were enrolled during the first period of the study (May–June) and 149 (37.3%) participants were enrolled at the Thai Travel Clinic. The demographic data of the participants are displayed in Table 1. The most common purpose of travel was business/work. Of note, 40% of travelers had experienced the test for COVID-19 and two of them had positive results. In addition, 90% of participants sought pretravel advice, and 54.4% sought a pretravel consultation at hospitals/clinics.
Table 1 Demographic data of participants (N = 399)Major sources of information about COVID-19 were social media (86.5%) and TV/radio (65.7%). Approximately three-quarter of participants reported that the COVID-19 pandemic had greatly affected their travel plans and resulted in trip cancellations or postponements (Table 2). The most common reason accounting for half of the cancellation and/or postponement was the travel restrictions from departure airports or the destination countries.
Table 2 Effects of COVID-19 on travel planKnowledge on COVID-19Twelve knowledge questions and the corresponding number of participants with correct answers are shown in Table 3. The knowledge score ranged from 4 to 12, and the mean was 8.64 ± 1.58. The mean knowledge score was significantly higher among travelers whose data were collected outside the hospital (8.79 ± 1.55 vs 8.39 ± 1.60, p-value < 0.001), among those who were Thai (8.73 ± 1.55 vs 8.34 ± 1.65, p-value 0.041), had a Bachelor’s or higher education level (8.89 ± 1.47 vs 8.02 ± 1.67, p-value < 0.001), had been tested for COVID-19 earlier (8.84 ± 1.41 vs 8.51 ± 1.67, p-value 0.035), or had a history of influenza vaccination in the past year (8.95 ± 1.45 vs 8.41 ± 1.64, p-value < 0.001). The mean knowledge score was also significantly higher in the group whose data were collected in the first period of the study (8.79 ± 1.57 vs 8.46 ± 1.58, p-value 0.042) (See Additional file 2).
Table 3 Percentages of participants with correct answerSufficient knowledge regarding COVID-19 (scored ≥60%) was reported in 77.9% of participants. The factors that were associated with sufficient knowledge were further determined using the logistic regression analysis. (Table 4) The covariates with p-value < 0.1 in univariate models were included in the multivariable analysis. The factors independently associated with a sufficient knowledge score were type of travelers (Thai) and education level (Bachelor’s degree or above).
Table 4 Factors associated with sufficient knowledgeAttitude toward COVID-19The attitude toward COVID-19 is displayed in Fig. 2. Nearly 80% of participants had agreed that COVID-19 was easier to spread than influenza and international travel should be discouraged throughout the outbreak. Approximately 60% of participants agreed that international travel posed greater risk than domestic travel. Over 80% of participants consider it is necessary for travelers from COVID-19 active countries to quarantine and mask-wearing to be mandatory in public. Seventy percent of participants agreed that their respective home country’s healthcare facilities were easily accessible in an event they developed abnormal symptoms. However, only 41% agreed that easily accessible healthcare facilities were available if abnormal symptoms arose at their destination countries.
Fig. 2
Attitude of the participants toward COVID-19. The attitude of international travelers toward COVID-19 was assessed with “5-level Likert scale” questions. The percentages of the attitude of participants regarding COVID-19 are displayed in the diverging stacked bar chart
The mean concern score over the COVID-19 situation was 6.09 ± 2.32 (maximum concern = 10). There were no significant differences in the mean score between the two data collection periods (p-value 0.703).
PracticesAlthough the overall mean practice score was high, a wide variation in the practice rate of each preventive measure was reported. The practices for reducing COVID-19 transmission were assessed by their frequency within several preventive parameters, ranging from 4 (always) to 1 (never). The mean practice score was 3.54 ± 0.38. The rate of ‘always practices’ by item ranged from 33.8–96.5% (Fig. 3). Almost all participants reported regular practices of basic preventive procedures against COVID-19. The rate of ‘always practices’ was high in the categories of wearing a mask when going to public places (96.5%), hand washing (88.5%) and avoiding contact with sick people (86%). However, only half of the participants reported good practices in the categories of avoiding going to public areas/using public transportation during rush hour, cleaning high touch surfaces every day, and checking body temperature when they feel unwell.
Fig. 3
Practices of the participants toward COVID-19. The percentages of participants’ practices of ten preventive measures toward COVID-19 are plotted in the stacked bar graph
To determine factors influencing practices regarding COVID-19 prevention, the stepwise multiple regression analysis (MRA) was employed. With respect to sociodemographic characteristics, the independent influencing factors for practices in COVID-19 prevention were site of data collection, pretravel advice at hospital, gender, period of data collection, age, and purpose of travel. (Table 5) The results revealed that mean practice score tended to be higher in participants who completed the questionnaire from outside the hospital (Beta = 0.195), participants who sought pretravel advice (compared with those who did not) (Beta = 0.168) and females (Beta = 0.154). In contrast, participants in the second period of data collection tended to have lower mean practice score (Beta = − 0.153). Participants aged 40–49 years had higher mean practice score compared to those who were younger or older (Beta = 0.143). Lastly, participants who visited friends and relatives were more likely to have higher mean practice score than other travel purposes (Beta = 0.107).
Table 5 Factors influencing practice on COVID-19 (Stepwise MRA)The differences in the practices of participant groups were then evaluated by item using the Chi-square test, and the percentage of participants who regularly (always) practice preventive measures were compared with those who do not regularly (sometime/rarely/never) practice (Table 6). Overall, the results showed a higher trend of ‘always practices’ in the first period than the second period of data collection. Most participants always wore a mask when going to public places, and there were no differences between different groups except Thai and non-Thai travelers (98.1% vs 90.9%, p-value 0.001). The hand hygiene practice was significantly higher in females and in the first period of data collection. Furthermore, the practice of cleaning high touch surfaces everyday was significantly more common among females, lower education group, Thai travelers, and among participants in the first period of data collection.
Table 6 The difference between participant groups and practices of COVID-19 measured by each item (Chi-square test)
留言 (0)