Objectives
While the mechanism behind how liver flukes work to cause cholangiocarcinoma (CCA) and hepatocellular carcinoma (HCC) has been well studied, there is a dearth of peer-reviewed literature on how comorbidities such as viral hepatitis (B and C) affect the progression of CCA and HCC. The most vulnerable populations with comorbidities can benefit through more research on this topic. Once the disease progresses to CCA or HCC, it will almost always be fatal in these populations so prevention and treatment of liver flukes should be prioritized and identification of external factors that could be contributors.
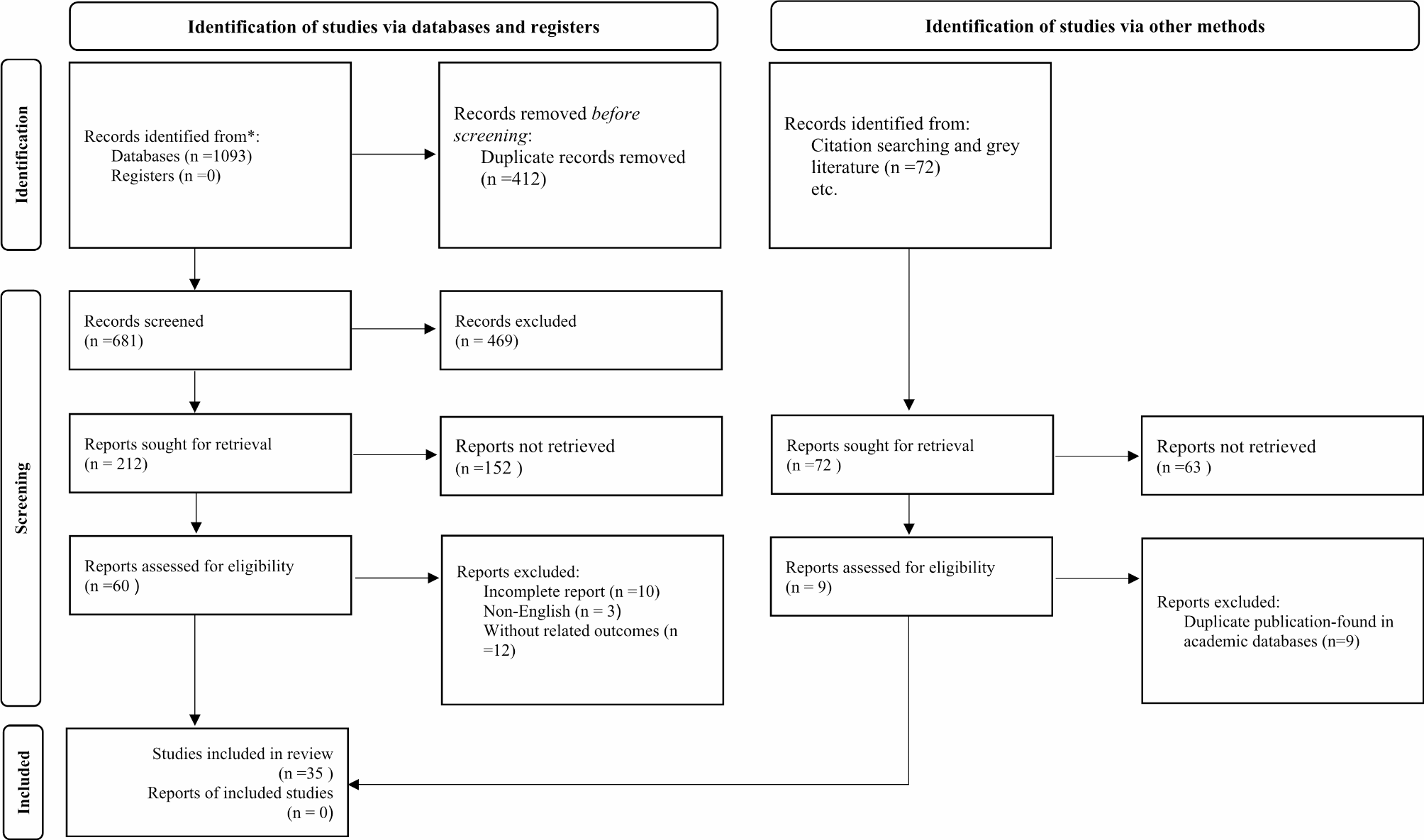
In this paper, we examine the effect of Hepatitis B and C viruses on the progression of O. viverrini and C. sinensis to CCA or HCC. We conducted a systematic review to analyze the available literature and identified the gaps and limitations in the manuscripts which impede showing causality.
Prevalence and geographic distribution
Liver fluke infections caused by Opisthorchis viverrini, O. felineus, and Clonorchis sinensis pose a major health risk to over 600 million people globally [7].
It is estimated that worldwide there are over 10 million people infected with O. viverrini and that 6–8 million of those individuals live in Thailand [24, 25]. O. viverrini is endemic to Southeast Asian countries, including Thailand, Lao People’s Democratic Republic, Vietnam, and Cambodia [8]. Even within Thailand the distribution of liver flukes is uneven with the north (19.3%) and northeast (15.7%) causing a high prevalence compared to the central (3.8%) and southern (0%) regions [6]. Khon Kaen province in northeast Thailand has the highest incidence liver fluke induced cholangiocarcinoma in the world [5, 16, 29].
It is estimated that globally over 35 million people are infected, and that 1.5–2 million people show symptoms or complications of C. sinensis [27]. C. sinensis infection is common in rural areas of Korea and China [8]. China has the largest population of infected people, which is estimated at 15 million [27].
Infection with food-borne parasites is common in these regions because uncooked cyprinoid fish are a staple of the diet. Liver fluke infection occurs when a human ingests raw freshwater fish that are fluke-infested [10]. Poor sanitation and sewage infrastructure in these countries also contribute to this problem. People infected with these liver flukes pass the eggs into the fresh water supply through the improper disposal of feces, which then leads to a continued cycle of infections [15].
In this article we are going to focus on O. viverrini and C. sinensis because they are predominantly found in Asia while O. felineus is mainly found in Italy, Germany, Belarus, Russia, Kazakhstan, and Ukraine [15]. These populations have different comorbidity burdens and access to healthcare which makes comparison insignificant.
Mechanism for causing cancer
Most people who have O. viverrini and C. sinensis do not display any symptoms of infection. About 5%-10% of individuals, usually heavily infected, have symptoms of right upper quadrant abdominal pain, flatulence, and fatigue [12, 19, 28]. Long-term and heavy parasite count infection of liver flukes is associated with several different hepatobiliary diseases including cholangitis, obstructive jaundice, hepatomegaly, fibrosis of the periportal system, cholecystitis, and cholelithiasis [4, 23] .
Liver flukes are classified as a group 1 carcinogen as the mechanical, immunopathic, and secretory pathways of the parasite have been directly linked to causing cholangiocarcinoma (CCA) and Hepatocellular carcinoma (HCC) [11, 16, 25]. It is estimated that around one in six people who are infected with liver flukes will develop CCA or HCC and the prognosis is very poor with an almost 100 percent fatality rate [17].
Mechanically, the liver flukes use their suckers to bind to the walls of the biliary ducts which causes ulcers [18]. The liver fluke eggs can then become ensnared in those ulcers and can cause granulomatous inflammation of the periductal tissue. C. sinensis, which is larger in size than O. viverrini, can cause a partial bile duct obstruction resulting in bile stasis and an increase in biliary pressure. Additionally, the immune response to the parasite causes damage to the cells which contributes to the mutation of the DNA. Many different immune cells respond to the presence of the parasite and attack the region which it occupies. Finally, the parasite’s excretory/ secretory products promote immune mediated inflammation which also encourages DNA mutation. All this damage can cause inflammation and then eventually healing which repeats for the whole length of the infection. This cyclic process can eventually cause DNA mutations that lead to the development of CCA.
Viral hepatitis and its role on the liver
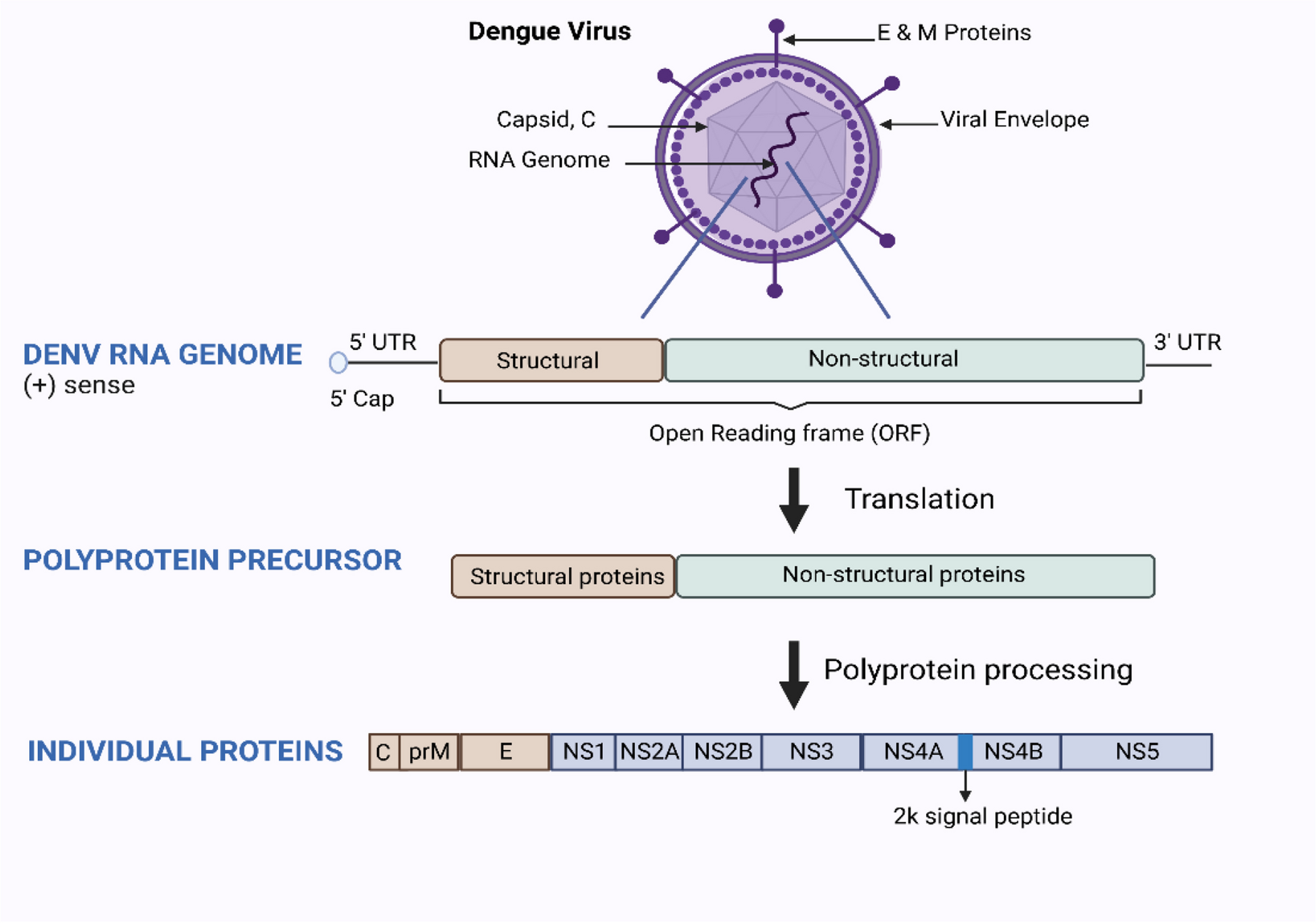
Viral Hepatitis plays an important role in the global cancer scale as it is the second leading cause of cancer behind tobacco use [1, 2]. Hepatitis B virus (HBV) belongs in the Hepadnaviridae family and Hepatitis C virus (HCV)is a member of the Flaviviridae family. The viruses are estimated to chronically infect over 300 million people globally and about 2 billion people (1 in 3) have been infected at one point in their life (CDC, 2019). Most people who are infected with HBV/HCV can clear the virus but an estimated 5%-10% of adults and 90% of babies will develop chronic hepatitis [9]. Chronic hepatitis infection can cause liver damage that can lead to liver disease or liver cancer [9]. It is estimated that 60%-75% of global chronic hepatitis infections are found in Asia and are endemic in many parts of the country [13]. HBV/HCV has been circulating around Asian countries for many centuries and they historically have low rates of vaccination [20]. A large proportion of individuals with chronic HBV/HCV infection in these countries were infected at childbirth and it is common to see many individuals in one household with the virus [20].
Liver flukes are a neglected tropical disease and resources for treating it are limited in these Asian countries. Understanding the comorbidities that increase the rate of progression from liver fluke infection to CCA or HCC would allow for more targeted treatment of the highest risk populations.






留言 (0)