
記住我

The skin is composed by the epidermis and the dermis, the latter consisting for 70% of connective tissue.1-3 Dermis thickness varies in the different body areas, decreasing with aging.1-4 The dermis has an intense vascularization, particularly in its deeper aspect.1-3 This vascular network serves a number of vital functions such as nutritional support for tissues and homeostasis.5 However, dermis vessels are usually not detectable in healthy subjects using color-Doppler and power-Doppler (PD) imaging.3, 5-8 This limitation is due to the small size of the vessels and to their slow velocity, commonly equal to or less than 2 cm/s. In the last years, several companies have developed advanced technologies for the ultrasound (US) study of the microvasculature. We hypothesized that these new techniques may allow detecting some more flow signals in the dermis compared to conventional PD imaging. Consequently, we prospectively compared PD and superb microvascular imaging (SMI, Canon Medical Systems, Tokyo, Japan) in the assessment of dermal vessels in healthy subjects (Figure 1).

Subjective scoring of the flow signals amount in the dermis. No flows at SMI and PD (a), comparable flows at SMI and at PD (b), more flows at SMI than at PD (c), more flows at PD than at SMI (d). Flow signals in the subcutaneous layer were not considered in this study
2 MATERIALS AND METHODS 2.1 Study design and subjectsThe study was developed as a single-center, prospective experience on healthy adult volunteers. The study protocol was reviewed and approved by our institutional review board and was conducted according to Good Clinical Practice and the Declaration of Helsinki. All participants provided written informed consent. The skin of the selected anatomical areas was inspected and subjects with cutaneous abnormalities were excluded. Hence, inclusion criteria were age above 18 years old and absence of any skin abnormality at both physical inspection and ultrasound exploration.
Thirty Caucasian subjects were enrolled between September 2020 and December 2020. There were 18 males and 12 females, aged 20–77 years (mean, 45 years old).
2.2 Ultrasound techniqueTwo radiologists with respectively 23 and 12 years of experience with US acquired each one the images of 15 random subjects. Care was taken to avoid an excessively low temperature in the room. We choose to study the following five body areas: forehead, dorsal aspect of the forearm, hand palm, buttock, and anterior aspect of the thigh. These anatomical sites were chosen considering some published articles on US assessment of skin thickness skin and echogenicity in sun-exposed and non-sun exposed areas as well as to study both glabrous and non-glabrous skin.2, 9-11
Gray-scale US, SMI, and PD images were obtained on an Aplio i800 system (Canon Medical Systems Corporation) equipped with a 22-MHz hockey stick-shaped linear array transducer. First a good quality skin image was taken on the gray-scale, using a large amount of ultrasound gel. SMI was then performed, in the color mode, with the following parameters: velocity scale, 1.5 cm/s; frame rate, 57 frames per second; filter 4 (range, 0–7); and dynamic range, 75 dB. The systolic cardiac phase in which the vascular codes were brightest and largest was caught in all cine images to exclude differences caused by pulsatility.12 In each body area, the flow signals were first searched by using SMI. Then, once that a clear SMI scan showing dermis vessels was taken, this image was freeze on the split-screen and then a corresponding PD scan was quickly obtained. The operator froze the PD acquisition and went back to the frame showing the largest amount of flow signal, storing it in the scanner archive. PD parameters were as follows: monochromatic code, velocity scale, 2.8 cm/s; frame rate, 19 frames per second; filter 2 (range, 0–7), and dynamic range, 75 dB. For both SMI and PD imaging care was taken to avoid motion of the operator's hand or the transducer, which was placed gently above the gel layer. The beam focus was placed at the dermis-hypodermis edge both for SMI and PD imaging. The color gain was not changed between the two techniques.
2.3 Images analysisTo obtain an objective, quantitative assessment of flow signals in PD imaging and in SMI we employed the vascularity index (VI), which determines the number and percentage of color pixels in the total gray-scale pixels in a defined region of interest (ROI).12-14 Starting from the saved double-screen image containing the SMI scan on the left and the PD scan on the right, we placed an identical rectangular ROI on both images to assess the VI. Care was taken to exclude the subcutaneous vessels and to include in the ROI only signals from the dermis. The color artifacts, defined as random and transient colored pixels not representing true flows, were always excluded from the ROI. These noise artifacts were sometimes present in the images, particularly on the SMI scans and, especially at the uppermost portion of the field of view, but care was used to review the frames and choose clear scans without any motion color artifact. The number of pixels with flow signals was recorded for both SMI and PD imaging for each anatomical site.
2.4 Statistical analysisAll of the statistical analyses were performed with MedCalc for Microsoft Windows (version 13.1.2.0, MedCalc). For comparison of the sensitivity between the SMI and PD in detection of flow signals for each anatomical site, the McNemar test was applied. A two-tailed P value of less than 0.05 was considered to indicate a statistically significant difference.
3 RESULTSThe mean number of colored pixels was 2047 for SMI and 769 for PD at level of the forehead, 3215 for SMI and 1256 for PD at level of the forearm, 3118 for SMI and 1029 for PD at level of the palm, 3667 for SMI and 600 for PD at level of the buttock, and 3192 for SMI and 436 for PD at level of the thigh (Table 1). Overall, mean VI was higher for SMI than for PD for all 30 subjects (100%). Regarding each anatomic area, forehead VI was higher for SMI than for PD in 28 out of 30 cases (93%), forearm VI was higher for SMI than for PD in 29 out of 30 cases (97%), palm VI was higher for SMI than for PD in 26 out of 30 cases (87%), buttock VI was higher for SMI than for PD in 30 out of 30 cases (100%), thigh VI was higher for SMI than for PD in 30 out of 30 cases (100%; Figure 2).
TABLE 1. Number of color pixels at SMI and at PD in 30 subjects at level of five different anatomic areas Body areas Forehead Forearm Palm Buttock Thigh Subjects Sex/age SMI pixels PD pixels SMI pixels PD pixels SMI pixels PD pixels SMI pixels PD pixels SMI pixels PD pixels 1 M/33 745 819 433 0 4548 3227 4543 78 344 0 2 M/41 1829 78 493 19 3289 2349 79 0 2309 0 3 F/67 602 0 6523 5898 813 28 327 0 934 412 4 M/20 6539 2301 2319 0 2232 3989 1227 0 369 0 5 F/40 872 129 1126 0 7645 7005 9132 2302 517 0 6 M/55 4502 3611 5237 4234 38 0 4209 0 5643 673 7 M/77 1002 321 7614 5493 812 802 3427 0 5638 788 8 F/55 529 0 5334 0 2347 57 348 47 588 0 9 M/60 921 622 3209 934 1021 0 6543 332 8208 990 10 F/42 848 340 1321 768 1876 0 5732 0 805 0 11 M/21 831 527 610 99 1860 1060 4390 90 452 27 12 M/21 3006 2143 562 0 1211 2356 4219 0 708 345 13 M/29 4775 807 1079 0 3443 271 3343 3245 4427 0 14 F/33 328 0 5742 4392 299 0 5837 3228 4376 564 15 M/65 788 622 4215 2311 4468 2511 459 0 6732 0 16 F/57 333 321 5659 0 2418 0 1446 0 663 0 17 M/43 476 428 4311 3218 7412 427 7432 329 389 276 18 F/57 481 519 1933 0 3437 276 3225 553 6866 222 19 M/38 336 291 6765 3423 374 0 4337 0 6534 0 20 F/28 1221 0 933 1206 3254 3345 332 111 1723 0 21 M/66 5904 3320 3321 234 1822 1731 568 0 6578 430 22 M/43 868 29 234 211 2476 0 6745 0 7262 1656 23 F/34 457 16 2320 0 2365 177 5698 0 2376 0 24 M/32 589 0 3278 1202 288 32 511 342 3423 0 25 F/47 9929 1302 5632 467 2654 211 2222 69 3766 324 26 M/76 4343 399 3328 0 6452 29 6598 0 3654 267 27 F/51 731 0 8345 3211 92 0 7056 4222 769 86 28 M/45 3320 2786 3377 342 9222 0 5678 2367 858 0 29 M/47 4211 0 326 0 478 976 3889 455 7623 6321 30 F/40 2478 1325 877 23 374 0 459 215 1234 0 Mean, 2047 Mean, 769 Mean, 3215 Mean, 1256 Mean, 3118 Mean, 1029 Mean, 3667 Mean, 600 Mean, 3192 Mean, 436 Abbreviations: F, female; M, male; PD, power-Doppler; SMI, superb microvascular imaging.
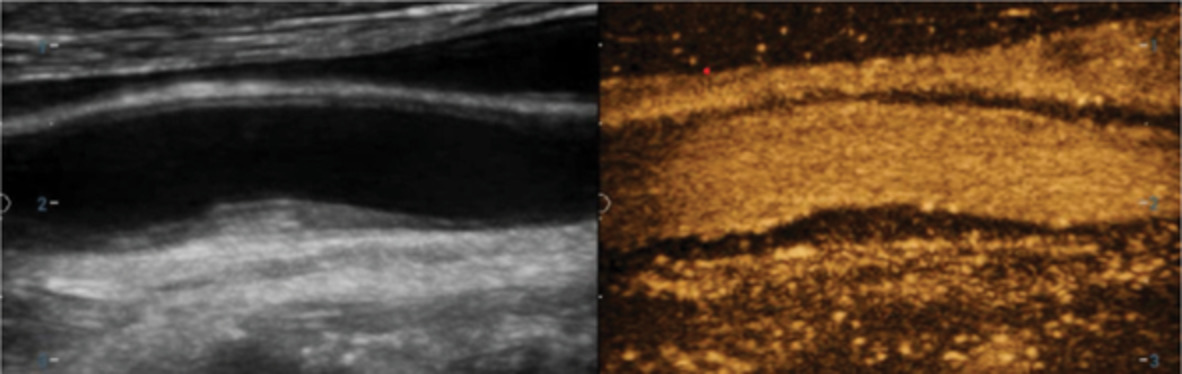
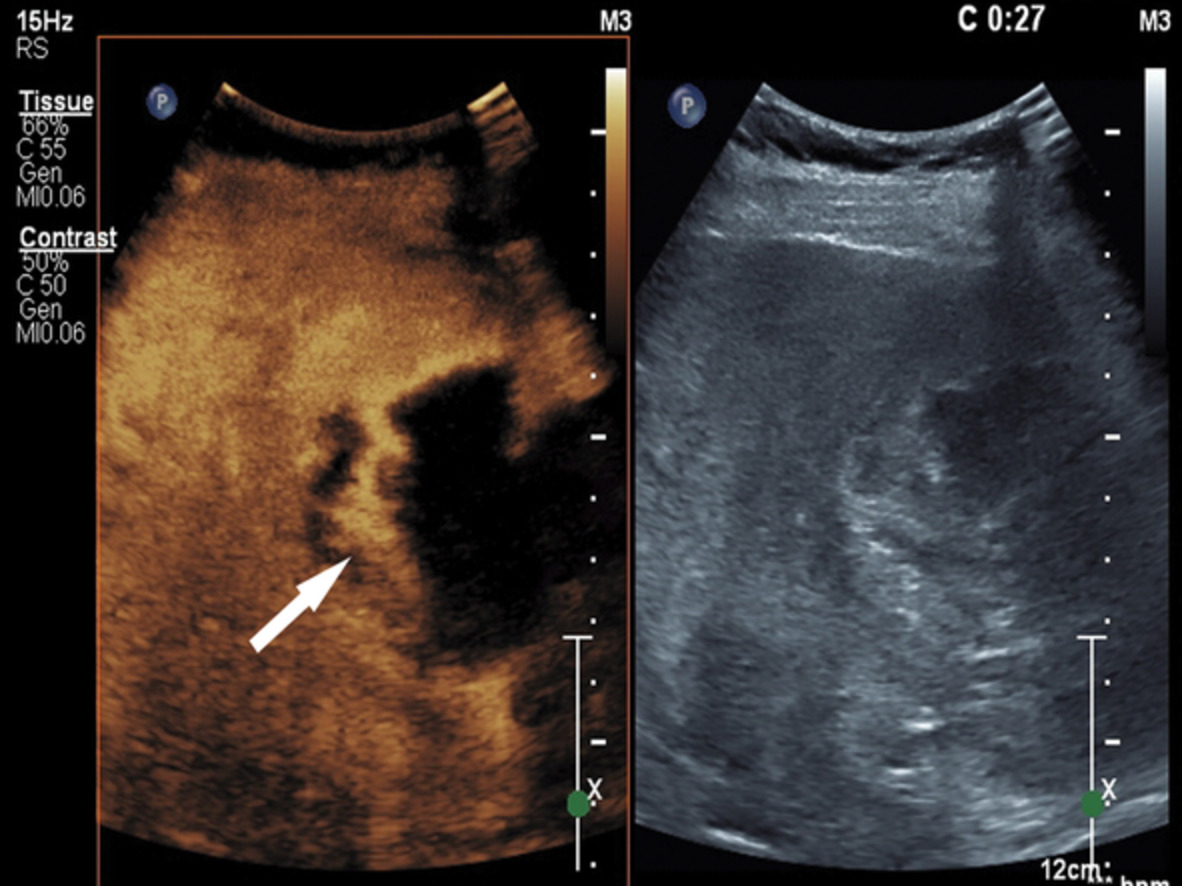
Sixty-year-old asymptomatic male. Dermis vascularization in the thigh at SMI (left part of the image), with 8208 colored pixels, and at PD (right part of the image), with 990 colored pixels
SMI, by detecting vascular signals in all 180 body areas, showed a sensitivity value much higher than PD (100% vs. 86%). PD even failed to show any flow signals in 7 out of 30 cases in the forehead (23%), 11 of 30 cases in the forearm (37%), 10 of 30 cases in the palm (33%), 14 of 30 cases in the buttock (47%), and 15 of 30 cases in the thigh (50%; Figure 3). The difference in terms of sensitivity was statistically significant for all the body areas investigated. The P value was less than 0.0001 for the forehead, forearm, and palm. It equaled 0.0002 for the buttock and 0.0003 for the thigh.

Fifty-seven-year-old asymptomatic female. Dermis vascularization in the forearm at SMI (left part of the image), with 1933 colored pixels, and at PD (right part of the image), with 0 colored pixels
4 DISCUSSIONThe dermis has a mesodermal origin and is dominated by packages of organized collagen, providing the supporting structure to the skin.15 On US it appears as a moderately echoic layer just below the thin, more hyperechoic epidermis.3, 6 From the histological point of view, the dermis includes the thinner, superficial layer of the papillary dermis, and the thicker and more profound layer of the reticular dermis. These two layers differ in the way collagen fibers are arranged, being denser in the reticular dermis.1, 8 US cannot readily differentiate these two portions, although the papillary dermis may be less echoic than the reticular one. The dermis includes blood vessels, lymphatics, nerves, hair follicles, and sweat glands.1, 16 Dermis vascularization decreases with aging, with a lower vascular density and a smaller vessels diameter in the elder than in the young.7, 18, 17 The structure of vessels is arranged into superficial and deep horizontal plexuses (Figure 4).5 A deep plexus, made by relatively larger vessels, mostly veins, is located at the interface of the dermis and subcutis. It is fed by branches of the large subcutaneous arteries. Vessels caliber in the reticular dermis, ranges from 50 to 150 μm.19 The border between papillary and reticular dermis hosts a superficial plexus that supplies the dermal papillae through a candelabra-like capillary system.8, 20 This superficial plexus is located 1–1.5 mm below the skin surface and consists of vessels less than 50 μm in caliber. The two horizontal plexuses are connected by direct, vertical, arborizing channels.19

Drawing showing schematically the normal skin vascularization. Large, subcutaneous vessels reach the dermis and form a superficial and a deep horizontal plexus
In the US assessment of vascularization of breast and thyroid nodules, for example, the difficulty resides in the small caliber of the vessels and in the slow flow of the blood inside them. For the skin assessment, there are two additional obstacles. The first one is the pressure applied by the transducer, even if the operator hold the probe gently. The second difficulty is the closeness of the skin vessels to the transducer footprint. It is known that the field-of-view area close to the transducer, called the Fresnel zone or near field, is the one better seen at ultrasound since the beam is collimated and the resolution is high. Instead, at some point distal to the transducer, in the far-field or Fraunhofer zone, the beam begins to diverge with decreased resolution. However, the region nearest to the probe is compressed in ultrasound image, for a length that depends on the transducer quality and on the emission frequency.21-23
Several strategies have been proposed to improve the ultrasound display of superficial, slow flows at color- and PD imaging. These include optimization of scanning setting sensitivity (small color box, high transmission frequency, low pulse repetition frequency, low or null wall filter, high color gain),6, 24 interposition of gel stand-off pads,21 use ultra-high frequencies,25 injection of microbubbles.26 Due to the intrinsic limitations of Doppler techniques, however, none of these options allows an adequate assessment of normal dermis vessels.
SMI applies clutter suppression algorithm that separates flow signals from overlying tissue motion artifacts. Consequently, SMI allows preserving the low-flow components, which are removed by conventional wall filters in color- and PD imaging, while displaying flow signals with a high spatial resolution and high frame rates.27 SMI uses higher frame rates than PD, more than 50 Hz, and lower pulse repetition frequencies ranging between 220 and 234 Hz.12 It analyzes the characteristics of motion artifacts arising from nearby structures and extracts the relevant information.28 SMI has proven effective in detecting small vessels in cases where color- and power-Doppler failed to identify any flow signal.27, 29 By now, this technique has been tested in a number of superficial and abdominal anatomical sites.13, 14, 27-29 Govind and coworkers found that SMI is more sensitive than color Doppler in demonstrating microvenous reflux in limbs with venous disease and SMI.30 İslamoğlu and Uysal employed SMI to assess plaques of cicatricial alopecia.31 To our knowledge, no study has investigated yet the value of SMI in studying skin vascularization. Dermatology is a growing field of application of ultrasound.4, 7, 24, 32 The availability of a technique capable to demonstrate dermal flows can be useful in evaluating the activity status of a number of skin abnormalities, including morphea, psoriasis, cutaneous vasculitides, suppurative hidradenitis, burns, wounds, and surgical flaps.4, 19, 33, 34 Our study proved that SMI is by far more sensitive than PD in detecting dermal flows. The difference is probably even higher than what found in our study. In SMI, the color signal is visible only in the vessels while in PD color typically bleeds out of the lumen. This blooming partially compensated at VI assessment the poor sensitivity of PD. Despite this, SMI was significantly more sensitive than PD.
There are some limitations to our study. Firstly, it was conducted in a single center, and the number of cases was relatively small. Secondly, the choice of the anatomical sites to be sampled was somehow arbitrary. However, since the difference between SMI and PD imaging performance was so marked, it is our opinion that similar results would have been obtained also if scanning other anatomical locations. Thirdly, although care was taken to obtain adequately matching scans between SMI and PD, these scans could not be perfectly identical each other. Finally, we made no attempt to differentiate dermis vessels into arteries and veins. This aspect was not relevant for the study purpose and, additionally, the vessels we investigated were too small to obtain an adequate spectral sampling.
In conclusion, new microvascular imaging techniques such as SMI allow reliable ultrasound display of normal dermis flows while conventional PD imaging cannot. This opens new perspectives in the assessment of dermal abnormalities.
ACKNOWLEDGMENTSPublication is approved by all authors and by the responsible authorities where the work was carried out. Each author has participated sufficiently in any submission to take public responsibility for its content.
CONFLICT OF INTERESTThe authors have no conflicts of interest.
ETHICS STATEMENTWritten informed consent was obtained from all patients, and the study was approved by the ethics committee of the institution.
留言 (0)