
記住我

Hyperparathyroidism is a clinical syndrome caused by excessive secretion of parathyroid hormone from the parathyroid gland. Hyperparathyroidism is divided into primary hyperparathyroidism (PHPT) and secondary hyperparathyroidism (SHPT). The main causes of PHPT are parathyroid adenoma (PTA), parathyroid hyperplasia, and parathyroid carcinoma.1 PTA is the most common, accounting for about 85%,2 among which solitary adenoma accounts for about 80% of all PHTP cases.3 On the other hand, parathyroid carcinoma is relatively rare, accounting for less than 1%.4 Moreover, the incidence of PHPT in women is three times higher than that in men, and the incidence increases with age.5, 6
The oversecreted PTH in PHPT patients has a short half-life and a multitarget binding ability, which can cause metabolic disorders in multiple systems and target organs. It can also lead to small local lesions and a large systemic effect.7 Patients with PHPT usually develop hypercalcemia.5 Its main clinical manifestations are complex, with kidney stones being the most common. It can cause osteoporosis and fracture, and can also cause calcification of blood vessels and soft tissues, increasing the risk of other diseases, and sometimes even endangers life.8, 9 PHPT may increase a patient's morbidity and even mortality if left untreated. While parathyroidectomy (PTX) is considered the standard treatment for PHPT, surgical treatment is traumatic and not well tolerated by all patients, especially elderly patients who cannot tolerate general anesthesia.10
Over recent years, several new techniques have been developed for treating PHTP, including microwave ablation (MWA), radiofrequency ablation (RFA), laser ablation (LA), and so on.11-14 MWA has been gradually applied in clinical practice, it is effective and safe approach that causes less trauma (no scar formation) to the patient and allows for quick recovery, and can remove lesion under local anesthesia. It provides a new tumor treatment for the elderly patients and young women who care for beauty. In this study, we evaluated the clinical efficacy and safety of MWA in the treatment of PHPT.
2 MATERIALS AND METHODS 2.1 PatientsThis retrospective study was approved by the Ethics Committee of our hospital (QYFYWZLL-26523). All patients signed written informed consent and agreed to follow-up. The medical records of all PHPT patients who received US-guided percutaneous parathyroid MWA treatment in our hospital between August, 2019 and January, 2021 were retrospectively analyzed. Demographic data, clinical symptoms, and lesion data (location, size, number, echo, pathological pattern), the ablation time, serum PTH, calcium, phosphorus levels were collected.
Inclusion criteria were: (1) PTH level >65 pg/ml, serum calcium levels >2.52 mmol/L; (2) 99mTc-MIBI and sonographic findings are positive; (3) patients who refused surgery or were not suitable for surgery (elderly, weak, those with severe heart or lung dysfunction, not subject to general anesthesia); (4) those with parathyroid glands located in difficult areas to resect (e.g., mediastinum, tracheoesophageal sulcus, posterior area of the esophagus); (5) those who underwent parathyroid surgery in the past.
Exclusion criteria were the following: (1) US and 99mTc-MIBI imaging showed an ectopic parathyroid tissue, which could not be accurately explored by ultrasound examination; (2) patients with difficult parathyroid puncture approach, for whom it was not possible to perform complete ablation; (3) pathological puncture results suggesting malignancy; (4) severe abnormal coagulation indicators (such as prothrombin time > 18 s, prothrombin activity <60% or platelet count <60 × 10 9 / L); (5) laryngoscopy reveals the presence of recurrent laryngeal nerve (RLN) injury, especially in patients with RLN injury opposite to the parathyroid nodules; (6) a history of neck irradiation; (7) other diseases affecting calcium, phosphorus and bone metabolism.
Preoperative preparation: (1) history collection: basic patient information and their clinical manifestations; (2) routine preoperative examination: routine blood, coagulation routine, electrocardiogram, serum PTH, calcium, and phosphorus level; (3) accurate localization of parathyroid nodules performed by US, and 99mTc-MIBI imaging; (4) laryngoscopy performed to rule out preoperative RLN injury; (5) anticoagulant drugs, such as aspirin, fawarin, and clopidogrel, which were to be preoperatively discontinued for more than 5 days; (6) the condition, as well as the intraoperative risks and possible postoperative complications, were explained to the patients and their family members.
2.2 MWA equipmentThe MWA equipment is consisted of a microwave generator, a flexible coaxial cable, and a cooled-shaft antenna. The antenna is an internally cooled ablation needle with normal saline (Nanjing ECO Microwave System, frequency 2450 MHz). Distilled water circulates through two channels inside the antenna to prevent overheating of the rod.
2.3 MWA principleThe essence of microwave is electromagnetic wave. The principle of MWA uses magnetron in its microwave generator to generate a large number of microwaves, which are transmitted to the ablation area through coaxial cable and ablation antenna. The polar molecules (mainly water molecules) in the tissue generate heat by high-frequency vibration, after which the local temperature rapidly rises to 60–100°C to cell dehydration necrosis, so as to achieve the purpose of treating diseases.15
The combination of US technology with MWA can help surgeons accurately and comprehensively locate the tumor tissue in real-time. The dynamic observation of the whole MWA process showed strong targeting, and the fluid in the isolation zone can be supplemented in time to avoid damage to the surrounding normal tissues.16 In a word, combined with ultrasound, MWA can effectively remove the lesions and these lay a foundation for subsequent treatment and can effectively improve the effectiveness and safety of treatment.
2.4 MWA procedureIn this study, a GE LOGIQ E9 ultrasound diagnostic instrument was used. Continuous electrocardiogram (ECG), blood pressure, and finger oxygen saturation were monitored throughout the process, and the changes of patients' vital signs were closely monitored. Before ablation, an ultrasound contrast agent (Sonovue, Bracco, Milan, Italy) diluted with sterile normal saline was injected through the cubital vein. The filling of parathyroid nodules was observed in real-time under low mechanical index (MI = 0.13) and dual contrast mode. The patient was then placed in a supine position with a soft pillow of 5–7 cm behind the neck to fully expose the neck. The surgical area was routinely disinfected, and 1% lidocaine (Chaohui Pharmaceutical, Ltd.) was used for local anesthesia of the skin surface and around the nodule. Under the guidance of Doppler ultrasound, the color blood flow were avoided. Normal saline was injected into the posterior parathyroid gland with a 23G PTC needle, and then a >5 mm isolation zone was formed between the parathyroid gland and the important surrounding structures.17 Then, the tip of a 16G MWA needle was placed in the deepest part of the parathyroid nodules. The ablation switch was turned on, and the corresponding power (20–30 W)18 was given. The nodules were then ablated by using the “moving targets” technique.18, 19 The ablation power, time, and tip position were adjusted according to the changes of the strong echo microbubbles.20 During the operation, the patient's vital signs and vocalization were closely monitored. Once dysphonia or pain intolerance occurred, the ablation was immediately stopped.11
Contrast-enhanced ultrasound (CEUS) is a technique to dynamically observe the enhancement patterns of lesion sites by intravenous injection of contrast agent under ultrasonic instruments. Different tissues have different patterns of enhancement, thus, it can be used to diagnose the disease. The resolution and sensitivity of ultrasonic diagnosis are improved.21-23 When strong echo microbubbles completely covered the lesion, CEUS was used to evaluate whether the ablation was completed24 (no contrast agent in the nodules suggested that the ablation was successfully completed; if the contrast agent was detected, the filling area was ablated again; the procedure was repeated until no contrast agent was present after which and the needle could be withdrawn11, 18). Therefore, CEUS was an important means to determine whether the ablation was completed, and can effectively avoid incomplete ablation and postoperative recurrence.7 The whole MWA process was completed by the same experienced ultrasound physician under the real-time monitoring of ultrasound equipment. In the ablation interventional surgery room, a specialist was responsible for recording the patients' angiography and ablation process and image and video storage. After surgery, the patient was ordered to receive medical observation for 1 hour in the observation room, and a bag of normal saline was placed on the neck and slightly pressurized to prevent bleeding or hematoma formation. The patient was monitored for any symptoms. If there was no discomfort, the patient was discharged.25 If the patient experienced hoarseness for more than 24 hours, a laryngoscopy was performed to explore for RLN damage.11
2.5 Case historyWe present a case of a 64-year-old woman with multiple endocrine adenomas (MEN2A type), grade 3 hypertension (very high risk), type II diabetes mellitus, and osteoporosis. 99mTc-MIBI imaging of the parathyroid gland was performed (Figure 1), showing an elliptical, slightly low-density nodular shadow on the upper pole of the left thyroid lobe, with a clear boundary with the thyroid gland. The size was 2.8 × 1.8 × 1.6 cm. The ablation procedures were shown in Figure 2a-2(A-F).

99mTc-MIBI imaging of the patient

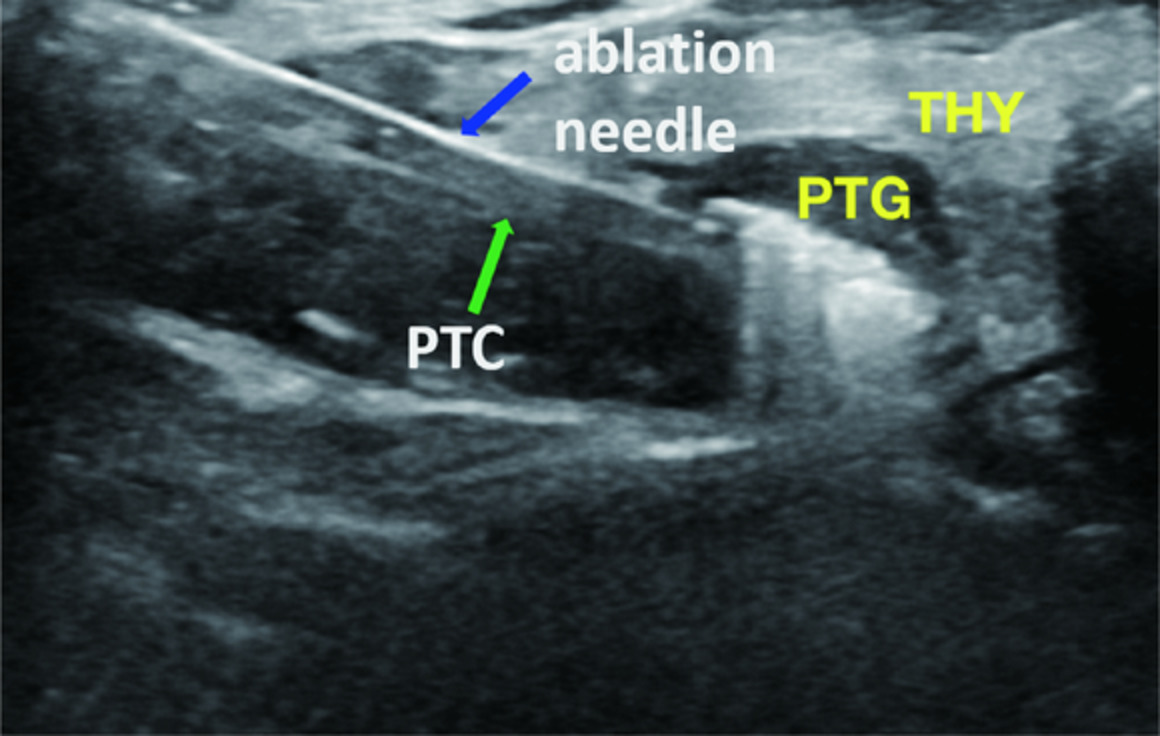
The ablation procedures of the patient
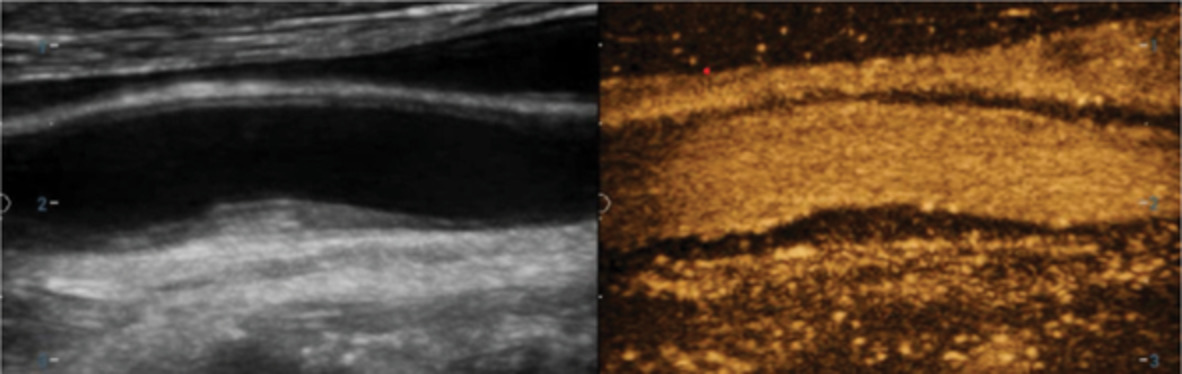
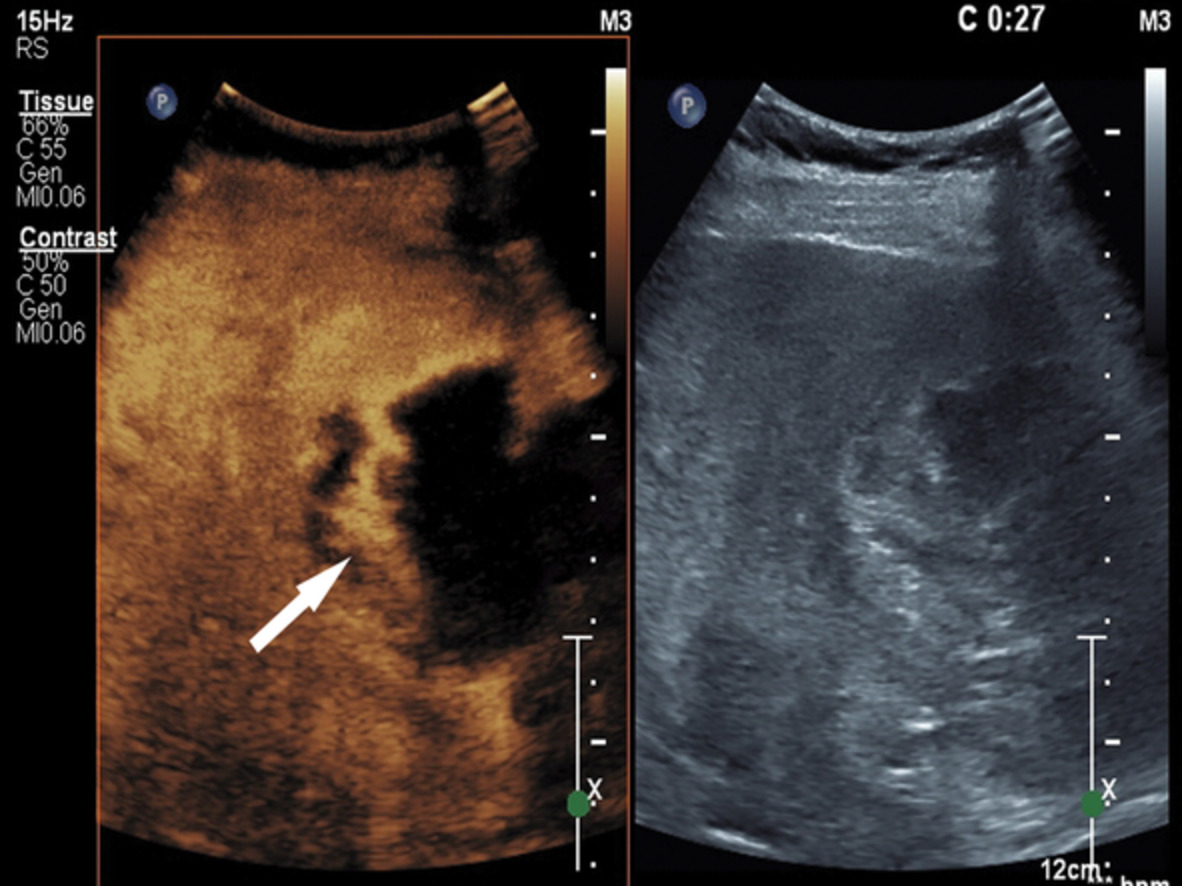
(A) Routine preoperative ultrasound examination: 2.9 × 1.9 × 1.4 cm hypoechoic nodules were seen in the upper pole of the left thyroid lobe, with regular morphology and clear boundaries. (B) Spot blood flow signals were seen in CDFI, and biopsy pathology suggested parathyroid adenoma. (C) Preoperative CEUS: 12 s contrast agent enters the periphery of the nodule (arrow) from the outside to the inside, showing equienhancement, and fades away in 25 s. (D) Full water isolation (red arrow) is performed for the parathyroid nodule to avoid damage to the surrounding tissues. (E) Intraoperatively, the strong echo microbubbles generated by the ablation needles (blue arrows) gradually expand until the strong echo completely covers the lesion, and the ablation is stopped. (F) Postoperative contrast imaging shows that the ablation area (arrows) does not see the obvious filling of contrast agent, and the ablation is completed.
CCA:common carotid artery, PTC:PTC needle, PTG:parathyroid gland, THY:thyroid gland, TRA:trachea.
2.6 Data collection and follow-upThe clinical data included the changes of biochemical blood indexes (serum PTH, calcium, and phosphorus levels), ultrasonic characteristics, and clinical manifestations. These data were collected before ablation and at each follow-up visit (2 hours, 1 day, 2 days, 1 month, 3 months and 6 months post operation) and statistically analyzed.
2.7 Statistical analysisData analysis was performed with statistical software SPSS (IBM Corp., Armonk, NY, USA, version 26.0). Continuous variables were expressed as mean ± standard deviation, or median and interquartile ranges. The paired-sample t-tests were used for those conforming to the normal distribution, and the paired-sample Wilcoxon signed-rank tests were used for those incompatible to compare the changes in serum PTH, calcium, and phosphorus levels before ablation and each follow-up visit. p-value <0.05 was considered statistically significant.
3 RESULTSA total of 35 patients with PHPT who received MWA treatment were included in this study and three of the them were ablated with double parathyroid adenomas. Basic information and post-ablation information of all patients are shown in Table 1.
TABLE 1. Basic information and surgical information of all patients Characteristics Data Number of cases (n) 35 Nodules in ablated lesions (n) 38 Sex Male (n) 9 (26%) Female (n) 26 (74%) Age (years) 55.63 ± 15.74 (34–85) <55 19 (54%) >55 16 (46%) BMI (kg/m2) 23.23 ± 3.42 (18.01–31.81) Location of nodules (n) Upper pole of left lobe 13 (34%) Lower pole of left lobe 10 (26%) Upper pole of right lobe 3 (8%) Lower pole of right lobe 12 (32%) Nodules in ablated lesions (n) 1 32 (84%) 2 3 (16%) Time of contrast agent(s) Time to focus 10.61 ± 1.0 (8–12) Time to fade away 21.11 ± 2.02 (19–25) Maximum diameter of lesion (cm) 1.62 ± 0.64 (0.9–3.2) Lesion volume (cm3) 1.29 ± 1.57 (0.14–7.4) Power of MWA (W) 29.08 ± 1.96 (25–30) Time of MWA (s) 182.63 ± 101.06 (56–407) Angiographic dose was injected before MWA (ml) 1.78 ± 0.22 (1.5–2.4) Angiographic dose was injected after MWA (ml) 1.76 ± 0.18 (1.5–2.2) Complications (n) Pain 4 (11%) Swallowing foreign body sensation 5 (14%) Hoarseness 3 (9%) Transient hypocalcemia 2 (6%) Associated symptoms of PHPT (n) Hypertension 19 (54%) Diabetes 13 (37%) Coronary artery heart disease 10 (29%) None 13 (37%) Abbreviations: MWA, microwave ablation; PHPT, primary hyperparathyroidism. 3.1 Laboratory analysisA follow-up visit was performed after MWA. Compared to that before treatment, serum PTH and calcium levels of the patients decreased at 2 hours, 1 day, 2 days, 1 months, 3 months, and 6 months, and phosphorus level increased (except 2 hours) after operation. Details were in Table 2, and changes in serum PTH, serum calcium and serum phosphorus levels after surgery were shown in Figures 3-5.
TABLE 2. The difference of the serum PTH, calcium and phosphorus levels of the patients before and after operation Time PTH (pg/ml) Ca (mmol/L) P (mmol/L) Before MWA 171.31 ± 85.91 2.69 ± 0.11 0.95 ± 0.17 Post-MWA 2 h 30.69 ± 16.78 2.65 ± 0.10 0.83 ± 0.18 Post-MWA 1 day 31.71 ± 8.65 2.35 ± 0.13 0.97 ± 0.17 Post-MWA 2 days 34.05 ± 7.56 2.27 ± 0.12 1.03 ± 0.11 Post-MWA 1 month 47.42 ± 11.96 2.29 ± 0.10 1.01 ± 0.10 Post-MWA 3 months 39.89 ± 10.78 2.25 ± 0.10 1.08 ± 0.09 Post-MWA 6 months 35.88 ± 7.75 2.24 ± 0.12 1.12 ± 0.11 Abbreviations: MWA, microwave ablation; PTH, parathyroid hormone.
Changes in serum parathyroid hormone level after surgery

Changes in serum calcium level after surgery

Changes in serum phosphorus level after surgery
Data are presented as the mean ± standard error. *p < 0.05, **p < 0.01, and ***p < 0.001 compared with the baseline values before MWA treatment.
As shown in Figures 3-5, 2 hours after MWA, the serum PTH levels of all patients significantly decreased (p < 0.001) and the serum PTH level basically returned to a normal level, which indicated that MWA could effectively destroy parathyroid lesions that are the main source of PTH. By contrast, the serum calcium level decreased slowly (p > 0.05) and was still higher than the upper limit of normal value.
One day after MWA, the serum PTH (p < 0.001) and calcium levels (p < 0.001) decreased, while the serum phosphorus level (p > 0.05) increased compared with their level before ablation. At 1 month, the levels of PTH and calcium increased, and a rebound phenomenon was observed. We observed whether the ablated lesions recurred or other new lesions appeared. At 3 and 6 months, the levels of PTH and calcium significantly decreased (p < 0.001), and the phosphorus level increased. From 1 day after the MWA operation to the end of the follow-up visit, the PTH, calcium, and phosphorus levels of the other patients were basically within the normal range, and the clinical symptoms were significantly improved, except for two patients whose PTH was higher than the normal range in the first and the third month.
The above results indicated that MWA was relatively safe and effective in treating PHPT patients. MWA could significantly reduce the level of serum PTH, calcium, and phosphorus, and it had a lasting effect. At the same time, it could improve the clinical symptoms of patients, improve the quality of life of patients, and reduce the suffering of patients.
3.2 Clinical symptomsMWA improved clinical symptoms such as fatigue and bone pain, which were relieved after treatment. Four patients had obvious pain after surgery and were given an ice pack cold compress. The pain was significantly relieved on the second day and was considered to be caused by postoperative thermal injury. Five patients developed mild swallowing foreign body sensation after surgery, which was considered to be related to postoperative edema in the ablation area. Three patients developed hoarseness after surgery, and their voices respectively returned to normal at 2 weeks, 2 months and 4 months after surgery. None of the patients developed tracheal or esophageal injuries, peripheral hematoma, infection, or other serious complications.
4 DISCUSSIONThe anatomical structure of the neck is fine and complex. The parathyroid gland is routinely adjacent to the neck vessels, RLN, trachea, esophagus, and other structures.26 In the past, surgical treatment of PHPT patients may be the traditional treatment method, and surgical treatment is associated with a high risk of trauma and complications.27 Previous studies have suggested that the recurrence rate of 1 year after surgery is as high as 30%.28 Moreover, there is a risk of general anesthesia for elderly patients, and as the surgical incision is usually 5–8 cm, young women are commonly concerned about postoperative scar formation.29 MWA can effectively solve these problems. Moreover, related studies18, 30 have shown no significant difference in the cure rate and clinical efficacy between MWA and PTX when treating PHPT patients.
Over the recent years, minimally invasive surgical treatment has developed rapidly and has gradually been widely used in clinical practice. Although parathyroidectomy represented by endoscopic surgery has little trauma, the visible scope under the microscope is small and there is a risk of damage to RLN. Moreover, it is difficult to accurately locate small lesions, which represents a big challenge during surgery.3 Thermal ablation techniques have been extensively applied, mainly RFA. RFA has been often applied for nodules <15 mm in diameter but has shown little effective for nodules with >15 mm in diameter and rich blood flow.31 LA can only temporarily decrease the levels of PTH and calcium, and its long-term effect was not significant.32 MWA is less used at present. In this study, MWA was used for the ablation of parathyroid nodules. The thermal efficiency of MWA was higher than other ablation methods,33 and it had the advantages of rapid temperature rise, high heat, short treatment time, relatively large ablation range, and complete inactivation of tumor tissue.16 At the same time, MWA applies thicker ablation needles and its accurate control of the thermal field is difficult. It also has high technical requirements for operators.
Several key points were summarized in the process of MWA: (1) Before MWA, US and 99mTc-MIBI imaging were used to comprehensively and accurately locate and evaluate the number and location of lesions34; when patients complicated with Hashimoto's thyroiditis, parathyroid nodules were not easily distinguishable from cervical region VI lymph nodes and could be further determined by fine-needle aspiration biopsy (FNA) and serum PTH eluents. (2) During the process of MWA, attention should be paid to establishing the isolation band, and the surrounding tissues of the lesion should be fully isolated with water to avoid damage and postoperative complications as far as possible. (3) If postoperative hoarseness did not recover after 24 hours, laryngoscopy should be performed to check whether RLN injury occurred. (4) The changes in biochemical blood indexes of the patients were closely monitored after surgery, and a timely correction was made in case of hypoparathyroidism and hypocalcemia.
In this study, three patients developed hoarseness after surgery and received an intramuscular injection of 1 dose of 5 mg dexamethasone to reduce the edema of surrounding tissues. Yet, symptoms did not improve 24 hours after surgery, and laryngoscopy examination indicated reduced activity of one side of the vocal cord. During a postoperative follow-up visit, the hoarseness of the patients gradually decreased and returned to normal at about 2 weeks, 2 months and 4 months after surgery, respectively. The main causes leading to hoarseness were: (1) patients with a large volume of ablated nodules, large ablation range, long ablation time, and difficult thermal field control, there was a risk of thermal damage; (2) although adequate water isolation has been done, the lesion was squeezed during the process of “moving the target,” so the isolation fluid was reduced or even disappeared, and adequate water isolation between the nodules and the RLN could not be achieved; (3) the continuous injection of isolation fluid and the edema of surrounding tissues during the operation compress the RLN, and the above factors may cause hoarseness; this was consistent with previous references.
One patient had bilateral nodules, 1.3 × 1.0 × 0.6 cm on the left side and 1.2 × 1.0 × 0.7 cm on the right side. No discomfort was observed after ablation of the nodule on the left side, then the right side was performed. In this patient, the serum PTH concentration significantly decreased from 207 to 6.88 pg/ml 2 hours after surgery. One day after the ablation, it increased slightly to 10.7 pg/ml. Two days postoperation review increased to 11.3 pg/ml, both lower than normal. After multidisciplinary discussion and analysis, it was concluded that the ablated parathyroid nodules were in the dominant state of secretion while the secretion of other normal parathyroid tissues was suppressed for a long time. The hormone level rapidly dropped after the elimination of dominant nodules, and the suppressed parathyroid tissues recovered to their secretory state after some time. It was suggested that the patient should be regularly followed up. His serum PTH levels then increased to 14.4 pg/ml at 1 month, 20.8 pg/ml at 3 months, and 26.6 pg/ml at 6 months after surgery and were within the normal range. We concluded that the treatment of bilateral parathyroid nodules by MWA was safe and feasible and was consistent with the relevant studies.35
One patient developed bone pain with no obvious cause, mainly in the metacarpophalangeal joint. Cervical ultrasound and parathyroid 99mTc-MIBI imaging indicated parathyroid adenoma. Abdominal CT and MR showed retroperitoneal space-occupying lesions. The final diagnosis was multiple endocrine adenomas (MEN2A type). Surgical treatment of parathyroid adenoma and abdominal pheochromocytoma was recommended. Due to high blood pressure and large fluctuation, the condition was difficult to control with drugs. Thus, surgical treatment was suspended. Reexamination revealed osteoporosis and multiple non-traumatic fractures of the right ankle, accompanied by gallbladder stones and kidney stones. The bone pain significantly increased. After the treatment of MWA, the levels of serum PTH, calcium, and phosphorus quickly returned to a normal level. Postoperative follow-up visits of the patients showed that the bone pain was significantly alleviated and the blood pressure level decreased, and the biochemical blood indexes remained within the normal range. It can be seen that MWA provides a good treatment for MEN2A patients, which can effectively reduce the pain and improve the quality of life in patients.
Patients after MWA may have a temporary decrease in serum calcium.36 Thus, timely reexamination should be conducted to avoid the occurrence of postoperative hypocalcemia. When hypocalcemia occurs, calcium gluconate may be taken orally for mild symptoms. 10 ml/days of 10%CaCl solution could be slowly and quietly pushed for more severe symptoms.37 In this study, the serum calcium level of one patient was lower than normal on the second day after the operation, and no obvious discomfort was reported. Oral calcium was given, and the serum calcium was rechecked on the third day and within the normal range. During a follow-up visit, the serum calcium of the patient was within the normal range.
In two patients, serum PTH level was slightly higher than normal range respectively in the 1-month and the 3-month review. The reasons were as follows: (1) MWA was not complete, and the residual glandular tissues showed compensatory function after postoperative recovery. (2) The body was stimulated by the outside in order to reach a state of balance, the results of hormone regulation in vivo. (3) The heat generated by microwave caused thermal damage to tumor margin cells, causing them to lose blood supply and gradually die. A small amount of serum PTH was still produced in this process. Serum PTH did not continue to rise after complete death. Their serum PTH concentrations were relatively stable in the follow-up visits, all within the normal range, and the difference was not statistically significant (p > 0.05).
Yet, this study has a few limitations. This study was a retrospective study with small sample size and short follow-up time. Thus, a larger, multi-center prospective and long-term follow-up study should be conducted to strengthen the results.
5 CONCLUSIONUS-guided MWA was an effective and safe approach to treat PHPT patients. MWA can significantly reduce the level of serum PTH, calcium, and phosphorus. In addition, Under the guidance of ultrasound, MWA can accurately locate the lesion tissue in real time and has strong targeting of treatment. In conclusion, MWA was a relatively ideal minimally invasive treatment method and provided a new treatment option for PHPT patients who were not suitable or were unwilling to receive surgical treatment.
ACKNOWLEDGMENTSThe authors thank Cheng Zhao, who performed MWA for PHPT patients. We also thank the members of department of abdominal ultrasound for their contributions and discussions during the preparation of the manuscript.
CONFLICT OF INTERESTThe authors declare no conflict of interest.
ETHICS STATEMENTAll procedures followed were in accordance with ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. Informed consent was obtained from the patients.
留言 (0)