Statement of principal findings
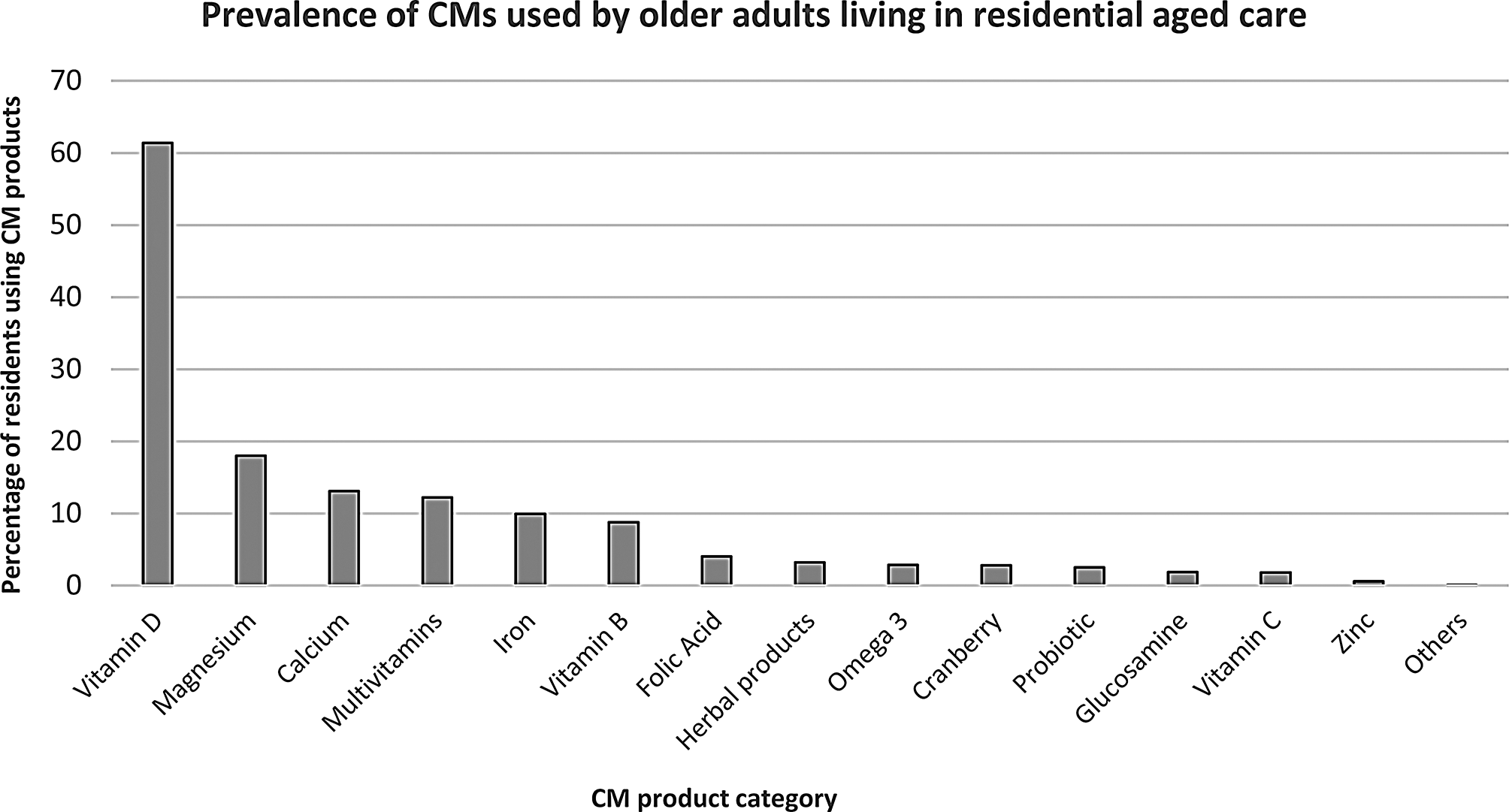
To our knowledge, this is the first study to describe the prevalence of CM use and factors associated with their use among older adults in Australian RACFs, and one of the few internationally that has investigated CM use in a residential aged care population. We observed high use of CMs with 78.4% of residents using at least one CM product, and 41.2% using two or more. However, the most frequent CM used in this population was vitamin D, with 61.4% of residents using vitamin D. Other frequently used CM products included magnesium, calcium, and multivitamins.
Interpretation within the context of the wider literature
The prevalence of CM use in our study is higher than that reported in previous studies conducted in RACFs internationally. A six-month study of 230 older adults in two RACFs in Turkey reported that 59.1% used at least one CM (e.g. garlic, vitamin B, vitamin C, fish oil, vitamin D) [24]. Another study of 189 older adults in a long term care home in Canada found 48.7% were using at least one CM in a year [25]. Our prevalence is also higher than findings from Australian studies conducted in settings other than RACFs which have used a similar definition of CMs as applied in this study. A cross sectional study among 341 adults found 44.3% had used a CM such as, multivitamin, magnesium, fish oil, vitamin D and calcium in the last fortnight [16]. Another study of 14,757 community-dwelling older adults observed 74.3% of CMs usage either daily or occasionally over four years [26].
Our results also show a higher prevalence of CM use than studies conducted in community- dwelling populations globally. In a survey of 560 participants in Jordan, three month use of CM was 64.1% [27]. Similarly, a survey of CM use in 1,008 adults in Norway reported 67% had used a CM in the three month period [28]. Older adults in RACFs often have multi-morbidity which may contribute to their higher rate of CM use compared to older people in the community [29].
In our study, vitamin D emerged as the most frequently used CM. The higher utilisation of vitamin D in RACFs could be attributed to the common deficiency of this essential vitamin observed among this population worldwide. Numerous studies have consistently reported vitamin D insufficiency among older adults in RACFs [30, 31]. Furthermore, vitamin D supplements are commonly used for fracture prevention in RACFs. According to recommendations from the Consensus Conference on the treatment of osteoporosis, falls, and fractures in RACFs in Australia, the use of vitamin D and calcium supplements is recommended for all residents in RACFs, to support bone health, given the prevalence of osteoporosis and associated fracture risks in this population [32,33,34]. Thus, despite the high levels of vitamin D use (61.4%) in our study this is lower than the recommendation that all residents receive vitamin D.
Evidence of the potential benefits from many of the CMs identified in this study is equivocal or largely absent in the literature such as, herbal products, glucosamine, magnesium, cranberry, omega 3, folic acid, zinc, and others. Omega 3 products and herbal products such as ginkgo biloba are potentially inappropriate medicine if used by residents with dementia, as evidence of their efficacy is absent [35]. Similarly, cranberry has uncertain evidence of its effectiveness for UTI prevention among the RACF residents [36, 37]. The use of CMs with limited evidence to support their efficacy could be a concern in the context of the high levels of polypharmacy experienced by RACF residents, which may increase risk of harm. There is evidence that some CMs may interact with prescription medicines, impacting drug metabolism and interactions with transport proteins [38]. For example, interactions can occur between warfarin and ginkgo biloba, garlic, cranberry, glucosamine, and fish oil, increasing bleeding risk [39]. There are also documented interactions between the antivirals used for the treatment of COVID-19 and CMs [10].
We found the proportion of residents on CM products varied widely between facilities, from 54 to 88% of residents using at least one CM product, and 23–52% using more than one CM product. However, only one out of 23 facilities had a CM utilisation percentage outside the control limits indicating that the use was lower than would be expected due to statistical variation. Given that vitamin D was the predominant CMs used in our population, the low use of any CM products in this facility could be a trigger to review whether vitamin D is being used in accordance with guidelines for the RACF population.
Implications for practice and research
The study highlights the importance of medication reviews for CMs, to ensure their desired effects (safety and efficacy) and monitor potential interactions with other medications carefully. The high prevalence of CM use in RACFs could lead to dug drug interaction. For example, drug interactions were seen with self-medication like glucosamine and warfarin elevates risk of bleeding. Thus, the high frequency of CM use among residents of RACFs needs to be incorporated as a part of comprehensive medication review. In addition to this further research needs to investigate the appropriateness of CM usage to ensure its safer and more effective utilisation in RACFs. Despite the high usage of CMs and important part of health care, Australian government has undertaken little research regarding policy point of view. Our study has revealed the high use of CMs in residents with osteoporosis and fracture. So, it would be good to regulate the information regarding CMs by the government, as consumers mostly get the information on CM from family, friends, and internet.
Strengths and limitations
The strength of the study is that it is the first to investigate the prevalence of CMs among older people in Australian RACFs using routinely collected aged care data. The use of electronic health data offers a valuable advantage in identifying CM usage without the need for time-consuming chart reviews or primary data collection. This streamlined approach enables researchers to access comprehensive information efficiently, enhancing the study’s efficiency and reducing potential biases associated with data collection methods. Furthermore, the study’s strength lies in its multi-centre design, involving a substantial cohort of 1873 residents from 23 different RACFs. This large sample size increases the study’s statistical power and generalizability of findings, allowing for a more robust and representative examination of CM usage patterns.
The limitation of the study is that it included RACFs from one aged care provider in a metropolitan area, thus the results of study may not be representative of all RACFs in Australia. Furthermore, our study did not consider other demographic variables such as ethnicity, education status, country of birth and language that may influence residents’ use of CMs, due to lack of data on these variables. We were also not able to examine the indications for CMs or ascertain the reasons for their use from the residents’ perspectives [40]. Moreover, it should be noted that CMs which were taken by residents in private space that did not cause severe consequences, might be missing in the medication administration data set because it might not be self-reported by residents to aged care staff. In addition to this, we have used data from December 2021 to determine the prevalence of CM use among residents in RACFs. Self-medication and misuse of drugs was common during COVID-19. Vitamins (C, D, Zinc), minerals, herbs, natural and dietary supplements were also popular during COVID-19. Seasonal allergies are commonly treated by CMs. It could impact the findings with increasing use of CMs by residents at that time.









留言 (0)