
記住我
This was a retrospective single center cohort study of infants with CDH born 2008–2023. We have structured our CDH DR program using the framework of a Learning Health System [15] to inform and improve care. In this model, observations of clinical performance and outcomes prompted changes to clinical management, which were then assessed through ongoing review of patient data. Temporal changes in golden hour management included initiating a lower fraction of inspired oxygen, reducing use of empiric inhaled nitric oxide (iNO), developing separate DR algorithms based on anticipated severity, and utilizing high frequency oscillatory ventilation as the initial mode of ventilation immediately after birth. With these temporal changes in management and introduction of an electronic medical record, infants were grouped into 3 epochs: 2008–2013, 2014–2018, and 2019–2023. Epochs were divided into roughly equal increments and marked by changes in clinical management as outlined below. Using the Clinical Outcomes Data Archive (CODA) Registry [16], we included all infants who received active treatment and excluded any infants with a planned palliative delivery. Outcome measures included extracorporeal membrane oxygenation (ECMO) therapy and survival. The CHOP Institutional Review Board approved this study (IRB 21-018553) with a waiver of informed parental consent.
Hospital delivery room resuscitation protocolsUniform interventions throughout all epochs: 2008–2023Throughout the entire study period, all infants with CDH were intubated immediately after birth, and received intermittent positive pressure ventilation (PPV) with a T-piece ventilator; settings included peak inspiratory pressures (PIPs) of 20–25 cm H2O, positive end expiratory pressure (PEEP) of 5 cm H2O, and a ventilation rate of 40–50 breaths/minute. A gastric decompression tube was placed immediately following intubation to promote adequate ventilation and stability by minimizing dilation of the intrathoracic bowel. Infants transitioned to a ventilator as soon as the endotracheal tube was secured. Vascular access was established and a blood gas, arterial if available, was used to guide ventilator adjustments (Fig. 1). Imaging and vascular access were obtained in the DR. It was our clinical practice to administer fentanyl with or without vecuronium to infants with significant hypoxia presumed to be secondary to pulmonary hypertension to improve pulmonary blood flow and reduce asynchrony with the ventilator. Throughout the study period, all new providers joining the SDU team participated in multidisciplinary delivery simulations focused on unique aspects of DR resuscitations of infants with surgical anomalies. The SDU DR team included a neonatologist, a neonatal fellow physician, an advanced practice provider, two to three neonatal intensive care unit (NICU) nurses, and a respiratory therapist. A pediatric surgeon frequently attended DR resuscitations.
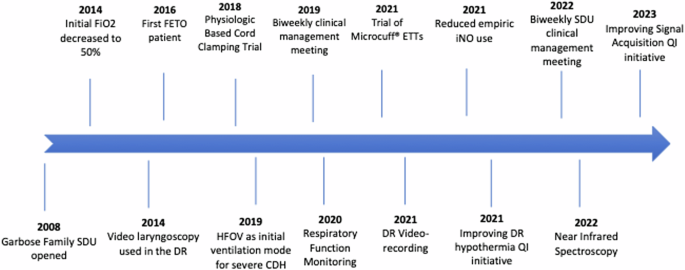
Fig. 1: Timeline of changes in delivery room practice.
DR delivery room, ETTs endotracheal tubes, FETO fetoscopic endoluminal tracheal occlusion, HFOV high frequency oscillatory ventilation, iNO inhaled nitric oxide, SDU Special Delivery Unit, QI quality improvement.
Changes introduced to the resuscitation protocol throughout the 15-year study period are outlined with significant events highlighted in Fig. 1.
Epoch 1: 2008–2013InterventionsFollowing the opening of the SDU in 2008, infants with CDH were born within the freestanding children’s hospital, thereby eliminating the need for postnatal transfer after delivery. Initial resuscitation protocols were grounded in historical perspectives and expert consensus. In addition to the interventions above, protocols included intubation with a conventional laryngoscope and conventional mechanical ventilation with an initial FiO2 of 100%. Empiric iNO was used frequently prior to echocardiogram in the setting of profound hypoxia on 100% FiO2 and based on provider discretion.
MonitoringMonitoring was limited to pulse oximetry and electrocardiography.
Epoch 2: 2014–2018InterventionsBeginning in 2014, initial DR FiO2 was decreased from 100% to 50%. FiO2 was then subsequently titrated to achieve pre-ductal oxygen saturation goals of ≥85% by 10 minutes of life and beyond. Riley et al. studied this practice change and demonstrated that an initial FiO2 of 50% was safe and effective [17]. Intubation in infants with CDH can be challenging due to significant airway deviation. Following review, our institutional experience demonstrated improved intubation outcomes with video laryngoscopy and in 2014 [18], video laryngoscopy was made standard of care.
In 2016, fetoscopic endoluminal tracheal occlusion (FETO) was introduced to our center for infants with severe left CDH. The Tracheal Occlusion to Accelerate Lung Growth trials found that FETO resulted in increased fetal lung volume and survival in infants with severe, isolated, left CDH with less clear benefit for infants with moderate CDH [19, 20]. In 2018, a pilot feasibility trial assessed physiologic based cord clamping, whereby the umbilical cord was clamped after intubation and lung aeration were established. Although physiologic based cord clamping was safe and feasible for infants with CDH, there was no clear benefit in clinical outcomes compared with historical controls [21]; therefore, this approach was not adopted for standard practice in our center.
Epoch 3: 2019–2023InterventionsBeginning in 2019, our DR protocol was updated to reflect two cohorts of infants with CDH based on anticipated severity, with severe CDH defined as an intrathoracic liver or right CDH. For infants with mild to moderate left CDH, initial conventional mechanical ventilation in the DR remained standard. Initial FiO2 was decreased further from 50% to 30% following close monitoring of infants started on 50% FiO2 with no adverse events noted and an overall reduction in exposure to supplemental oxygen. Patient level outcomes including delivery room outcomes (bradycardia, hypotension, Apgar scores) and NICU outcomes (survival, duration of invasive ventilation, incidence and duration of ECMO, days to surgery) were compared pre and post policy change to assess patient safety, as described in Riley et al. [17]. In contrast, as a response to high rates of hypercarbia in infants with severe CDH, high frequency oscillatory ventilation (HFOV) was established as the initial mode of ventilation for infants with severe CDH immediately after the endotracheal tube was secured; initial FiO2 remained at 50% for this population. Recommended HFOV settings include Mean Airway Pressure (MAP) of 11–13 mm H2O, amplitude of 30–35 adjusted to achieve appropriate chest wall vibration, and frequency or Hertz (Hz) of 6 for term infants that was increased with decreasing gestational age. Within these ranges, clinicians were encouraged to use the lowest possible settings to minimize barotrauma. The clinical impact of initial HFOV was assessed four years after this practice change; this analysis demonstrated significantly improved early gas exchange with no adverse differences in hospital outcomes among infants with severe CDH [22].
iNO was considered as an adjunctive DR therapy in infants predicted to have severe CDH with severe hypoxia on 100% FiO2. However, with a growing appreciation for left ventricle (LV) hypoplasia and dysfunction as a contraindication to iNO due to increased risk for pulmonary edema [23,24,25], we evaluated our experience and found increased ECMO need and higher mortality in infants with LV dysfunction that were treated with iNO [26]. Thus, in 2021 we changed our guidelines to recommend against use of iNO in infants with evidence of LV dysfunction.
We socialized these new guidelines and recommended obtaining an echocardiogram to evaluate LV function prior to starting iNO. Instead of empiric iNO use, we now use iNO on a case-by-case basis in a subset of infants with RV dysfunction without LV dysfunction and do not use iNO in the delivery room.
In 2021, we briefly introduced Microcuff® endotracheal tubes in the DR to allow inflation of the cuff peri-operatively to improve ventilation during the dynamic respiratory challenges during CDH repair. However, the practice was discontinued after an interim review of 22 patients revealed that more intubation attempts were needed to successfully intubate infants with CDH in the DR when Microcuff® tubes were used. Finally, in 2022, we undertook a quality improvement project to reduce rates of admission hypothermia for infants with congenital anomalies, given the evidence demonstrating both the association between admission hypothermia and increased morbidity and mortality in preterm infants and the increased risk of hypothermia in infants with congenital anomalies [27]. At baseline, 27% of infants were hypothermic (<36.5 degrees Celsius) on NICU admission. Plan, Do, Study Act cycles included standardizing the temperature of the DR and resuscitation bed, recommendations for increased frequency of temperature monitoring, trialing polyethylene lined hats, and implementing a DR thermoregulation checklist; in conjunction, these interventions led to an improvement with hypothermia seen in only 9% of infants in a recent cohort [28].
MonitoringIn 2020, we introduced enhanced monitoring in the DR beginning with respiratory function monitoring (RFM) to characterize the transitional pulmonary physiology of infants with CDH in real time during DR resuscitation [29]. RFM allows for evaluation of exhaled tidal volumes and end-tidal carbon dioxide monitoring during invasive positive pressure ventilation immediately after birth to guide ongoing ventilatory support. DR resuscitation video recording was also introduced in 2021 as routine practice for quality assurance [1]. In 2022, we introduced near infrared spectroscopy (NIRS) to evaluate cerebral hypoxia during the perinatal transition with ongoing evaluation of these data. In 2023, we started a quality improvement study to improve time to lead placement and vital sign acquisition in the DR given the unique challenges and competing interests of immediate intubation and invasive ventilation for infants with CDH. Plan, Do, Study, Act cycles have included transitioning to different electrocardiography leads with faster time to signal acquisition as well as rotating infants on the warmer bed to give bedside nurses improved access to placing leads on the infant.
Planning/team communicationIn 2019, we implemented biweekly multidisciplinary CDH clinical management meetings to review DR and neonatal care. In 2022, we added alternating biweekly SDU management meetings to review upcoming deliveries and management plans, recent deliveries, and areas for education or improvement. In 2022, we implemented monthly video review conferences to identify facilitators and challenges to optimal stabilization that inform education initiatives, quality improvement projects, and guideline changes.
Main outcome measuresMain hospital-based outcome measures included extracorporeal membrane oxygenation (ECMO) therapy and survival.
Data analysisWe evaluated the proportion of infants who experienced these outcomes across epochs. The Chi-squared test of trend was used to evaluate systematic increase or decrease in categorical variables across the time epochs. A linear regression model with the epochs coded as a continuous variable was used to evaluate trends in continuous variables. Additionally, a multivariable logistic regression was used to assess the confounder adjusted association between survival at NICU discharge and time. All analyses were conducted in R V.4.1.2.
留言 (0)