Time-and-Motion Methods as a Novel Approach to Evaluating Pump Therapy
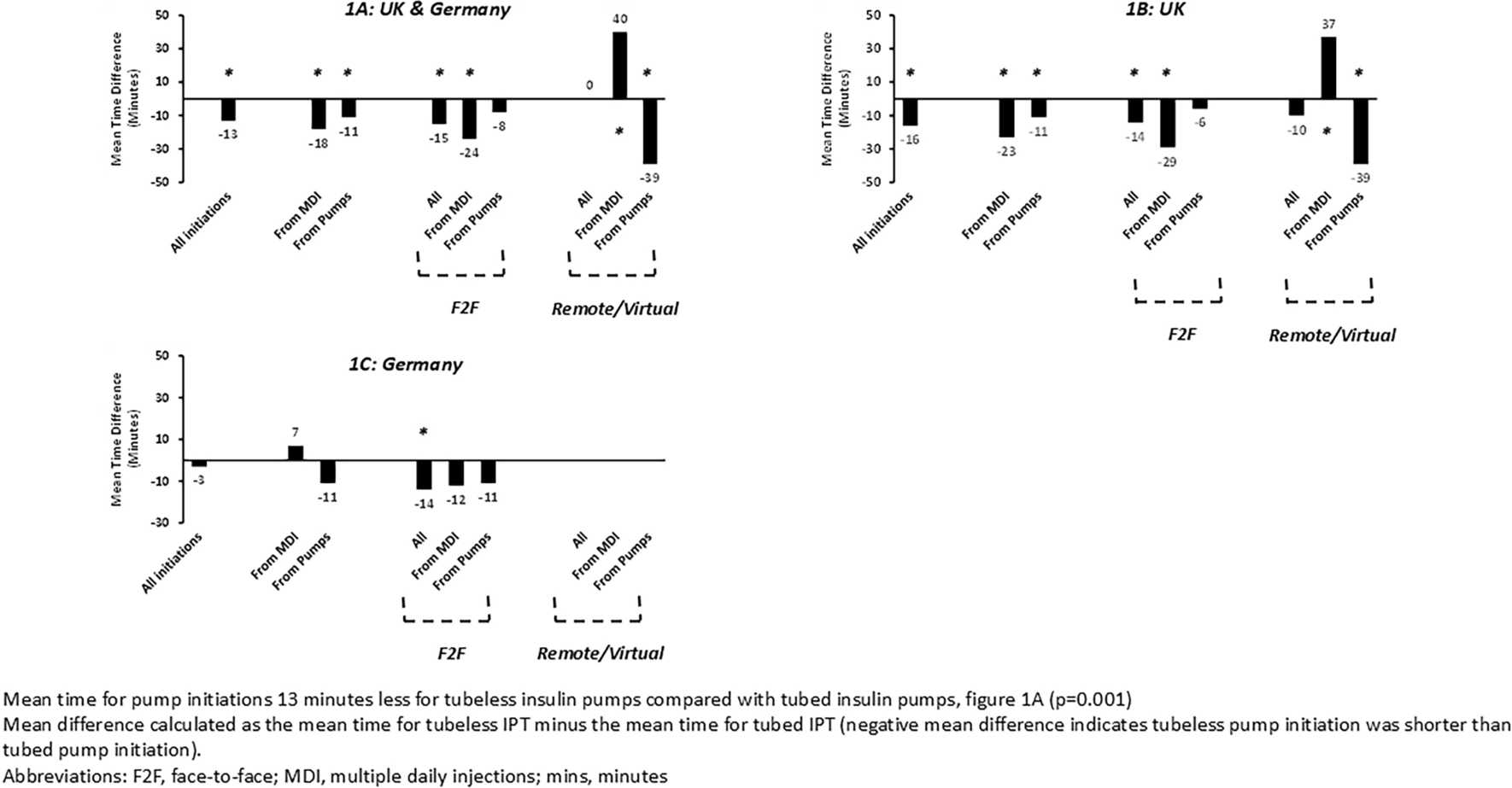
Time and motion is a technique that has wide acceptance in healthcare for investigating resource use and providing insight into workflow efficiencies, patient safety and quality, and is a term that can be used to describe a broad spectrum of study designs [19, 22]. This time-and-motion study took a novel approach to investigating practices in the delivery of diabetes care focusing on the process of initiating people on IPT where there has been little previous research, identifying significant time reductions for initiating tubeless IPT compared with tubed ones, 13 min of nurse time per person. By using a remote technology-based methodology, the study was able to reach a large number of diabetes nurse educators working across a wide range of real-world settings in two countries, lending the results external validity and real-world relevance.
Initiation Settings and Previous Therapy
For initiations in remote versus face-to-face settings, differences in approach and user engagement could be a confounding factor. There was a particular time-savings benefit for tubeless IPT initiations observed in people transferring from MDI and for all initiations in a face-to-face setting. People transferring from MDI in a face-to-face setting had a substantial time saving with tubeless pumps (24 min per nurse per initiation), and this was also large for people transferring from prior IPT in the remote/virtual setting (39 min per nurse per initiation). The findings for prior MDI users are particularly relevant to practice for initiating people onto IPT as the majority of people in the UK and Germany with T1D use MDI. Only one analysis showed a shorter time with a tubed IPT, for people transferring from MDI in a remote/virtual setting. It is notable that the mean time for the tubed IPT initiations in this subgroup was 70 min, substantially shorter than the mean for all the tubed initiations, 131 min, and could indicate some unseen confounding in the initiations from people transferring to a tubed IPT from MDI in the remote/virtual setting. The difference between tubed and tubeless IPT was less in Germany than the UK, which may be due to the smaller sample size in Germany, but was directionally the same. A comparison of the remote/virtual initiations was not possible in Germany due to insufficient numbers.
People upgrading from a previous iteration of IPT from the same manufacturer, for example the Omnipod System to Omnipod DASH or from Medtronic 640G to 740G, would already have substantial familiarity with that type of technology. For prior IPT initiations, the tubed IPT group had a higher proportion of initiations upgrading IPT from the same producer than the tubeless IPT group, 40% (26 users) vs. 23% (9 users) mitigating this as an explanatory reason for the shorter initiation time for tubeless IPT in the prior IPT group.
Interpretation of Time Savings with Tubeless IPT
In our clinical experience, several key practical factors may plausibly contribute to time savings with tubeless insulin pump therapy (IPT) during the initiation process and result in fewer unresolved questions at the end. With tubeless IPT, there is no need to spend time inserting the battery, as the controller is charged by means of a rechargeable battery that can be done before the pump initiation appointment. During initiation, the first pod is filled concomitantly with the instruction and the cannula is inserted automatically. Therefore, there is no need for an explanation of how to fill the reservoir and use the infusion set correctly as is necessary with tubed IPT. Tubeless IPT can easily be worn on the body in several locations where insulin would ordinarily be administered. Tubed IPT have different wearing systems (clip, strap) to choose from due to the indirect connection to the body, and this can vary for different activities such as sleep or sports, requiring additional explanation, especially for people switching from MDI to IPT. The tubeless IPT handheld controller comes with a logically structured setup menu that takes a new user through the most important points after switching on for the first time step by step, which allows for an efficient setup process. Lastly, the low component count with the pod and controller saves time, as explanations on system assembly are not required [23].
Importantly, according to the survey responses, nurses reported initiations on tubeless IPT to be as effective as on tubed ones despite taking less time. Nurses reported similar perceived confidence levels relating to the user’s capability to use their pump following the initiation with both tubeless and tubed IPT.
Implications for Delivery of IPT in UK and Germany
The structure of care for people with type 1 diabetes in Germany is extensive and organized into three areas: outpatient care, hospitals, and rehabilitation facilities. Outpatient care in the community can be delivered via specialist practices or general practice care with substantial regional variation of this mix. Delivery of technical instruction on the use of IPT can take place on an outpatient or inpatient basis, as individual or group training, and is the responsibility of manufacturers and done for the company by personnel certified in instruction on the model with oversight by diabetes specialists within the practice, who may also do the initiations themselves. An upward trend in the use of modern technologies and a positive attitude by people with diabetes is leading to increasing demand for IPT [24]. Meeting the demand for initiations presents a challenge, limiting access to the technology and potentially contributing to unequal adoption among underserved populations in Germany [9].
Across the UK, access to IPT has been variable. In England and Wales, NICE Technology appraisal guidance currently recommends IPT in people aged 12 years and over who cannot achieve their target HbA1c on MDI without disabling hypoglycemia or in those whose HbA1c levels remain high despite a high level of care [25]. Those starting IPT should be initiated by a specialist team, which should include the physician leading the care, a diabetes specialist nurse, and a dietitian. Commonly, initiations are done one-to-one in a hospital setting and in practice frequently involve a representative from the manufacturer. Due to increasing demand for IPT and limited diabetes workforce capacity recommendations from the British Clinical Diabetologist's Diabetes Technology Network are that, “ongoing support from industry will be required in upskilling HCPs and in onboarding people with T1D in an efficient manner” [26].
The time savings for initiations of tubeless IPT of 15–20 min in this study have a substantial scale and potentially important implications for pump services in Germany and the UK in addressing these needs as they could be used to increase throughput for IPT initiations. Applying this time saving across a pump service could substantially reduce the workload needed to initiate IPT and potentially increase service efficiency. This could release an hour of time for every 3–5 initiations that could be used for an additional pump start or other productive work.
In Germany, where doubts about incorrect therapy decisions, information overload, and a negative impact on the doctor–patient relations have been reported, the low number of virtual initiations suggests initiations done virtually/remotely are less common practice. The high level of nurse-perceived confidence in users’ ability to use the pump after the remote/virtual initiations in this study, including in Germany, suggests that despite these reservations, virtual settings are a potential time- and cost-effective model that can be used for initiations in suitable users (those with internet access, with a preference for remote/virtual initiation, previous knowledge of MDI/pump therapy) but particularly for those who are experienced IPT users/pre-existing IPT users. In the UK, the COVID-19 pandemic saw an exponential rise in virtual service delivery, meaning locality and waiting times may no longer be a barrier to pump services [17]. With staff trained specifically in the remote/virtual initiation of tubeless IPT, a large number of patients could be reached in a shorter time, with more flexible appointments, and less need to travel. This could have the potential to enhance ongoing concordance and engagement with IPT. Though the subgroup analyses in this study does not allow for robust conclusions, Tubeless IPT, having a short initiation time overall, fewer components and arguable simplicity in comparison to tubed IPT, could be an enabler for remote/virtual initiations. Remote/virtual initiation of IPT will not be suitable for all users, requires appropriate follow-up, including face-to-face options, and there are issues around digital equality and preference to consider. Ongoing evaluation of service responsiveness to need should be done to enhance satisfaction and concordance with IPT.








留言 (0)