
記住我
The interaction between public health issues and economic development has garnered increasing attention in the context of accelerating globalization and urbanization. In recent years, recurrent public health crises have posed profound challenges to global health systems while disrupting the stability and sustainability of regional and global economies. Public health expenditure, as a cornerstone of improving population health and promoting social welfare, plays a vital role in addressing these challenges. Encompassing a wide range of activities—including the development of medical infrastructure, vaccine research and distribution, and disease prevention—public health expenditure directly strengthens the foundational health conditions necessary for economic stability. By optimizing resource allocation and promoting health equity, it bolsters both societal resilience and economic growth (1).
Cities, as the primary hubs of economic activity, face mounting vulnerabilities to external shocks such as natural disasters, economic fluctuations, and public health emergencies. Urban economic resilience—the capacity of cities to withstand, adapt to, and recover from such disruptions—has become a key indicator of their risk management capabilities and long-term viability. Existing research highlights how economic resilience enables cities to adjust their economic structures, optimize resource allocation, and sustain growth amid crises (2). Enhancing urban economic resilience, therefore, is not only critical for a city’s ability to survive and recover during crises but also for achieving high-quality, sustainable development and social stability.
There exists a profound and intrinsic relationship between public health expenditure and urban economic resilience. Public health spending plays a pivotal role in safeguarding the health of urban populations, enhancing resilience to risks, promoting economic structural optimization, and advancing social stability and health equity. As such, it is not only a critical component in cities’ responses to public health crises, but also a key lever in strengthening urban economic resilience. This study addresses three core questions: (1) how public health expenditure affects urban economic resilience; (2) the mechanisms through which this influence operates; and (3) the regional and spatial characteristics of these effects. By providing both theoretical insights and empirical evidence, this work aims to contribute to the growing body of literature on urban economic resilience and to inform policymakers in optimizing public health and economic strategies.
2 Literature reviewPublic health expenditure is a fundamental component of socio-economic development in modern nations. With the increasing frequency of global public health crises, the economic benefits and social impacts of such expenditures have garnered significant attention (3, 4). Economically, public health investment enhances labor productivity by improving population health (5, 6). A healthier workforce demonstrates higher participation rates and greater efficiency, thereby contributing robustly to economic growth (7). Moreover, health investment reduces the burden of medical expenses, freeing up disposable income for businesses and households, which in turn stimulates consumption and investment, driving further economic development (8). Public health expenditure also indirectly fosters per capita GDP growth by improving overall health conditions (9, 10). Empirical evidence highlights a strong positive correlation between per capita GDP growth and public health spending (11). Additionally, the growing demand for health services promotes the expansion of the service sector, optimizes urban industrial structures, and enhances economic diversity and resilience to external shocks (12, 13). From a social perspective, the allocation of public health expenditure is closely tied to achieving social equity (14, 15). Equitable distribution of healthcare resources can narrow health disparities, improve access to medical services for vulnerable populations, and enhance overall societal well-being (16). For developing countries, increasing public health investments in low-income regions is particularly important, as it optimizes resource allocation and fosters balanced regional development (17). To address public health challenges more effectively, many countries are increasing the proportion of their budgets dedicated to public health, with particular emphasis on vaccine development, healthcare infrastructure, and disease prevention (18). Simultaneously, ensuring the equitable distribution of resources—particularly by prioritizing underserved groups and underdeveloped areas—is essential to achieving universal healthcare access and equity (19).
Against the backdrop of globalization and rapid urbanization, enhancing urban economic resilience has emerged as a key concern for scholars and policymakers alike (20–22). Existing studies on economic resilience often focus on dimensions such as technological resilience, resilience measurement, policy orientation, and industrial diversification. Urban economic resilience is typically defined as a city’s ability to withstand, adapt to, and recover from external shocks, encompassing four dimensions: resistance, recovery, regeneration, and adaptability (23). This concept emphasizes not only short-term recovery but also long-term structural adjustments and innovation capacity (24). In terms of technological resilience, research has shown that cities can effectively respond to and adapt to economic shocks by optimizing technological structures and enhancing technological capabilities, underscoring the critical role of technological resilience in urban economic development (25, 26). Economic resilience is commonly measured using either composite indicator systems or single-indicator methods. For instance, some scholars have developed integrated ecological risk assessment frameworks to demonstrate the long-term Granger causality between land-use changes and ecological risks (27). Other studies compare economic resilience across urban and rural regions relative to regional averages, calculating the economic resilience of NUTS-3 regions (28). Additionally, by analyzing actual wage levels against counterfactual predictions, researchers have assessed urban performance during economic shocks (29). Spatial panel data models have also been employed to forecast employment growth rates, providing insights into the resilience of different regions when confronted with economic disruptions (30). The determinants of economic resilience are multi-dimensional and multi-layered. A diversified economic structure effectively mitigates risks by reducing the impact of external shocks on specific industries or economies. Regions with higher levels of education and skilled labor markets adapt more rapidly to economic changes, fostering innovation and growth. Moreover, robust innovation ecosystems create new growth drivers through technological advancements, knowledge diffusion, and business incubation. Historical and cultural traditions also influence economic resilience by shaping institutional quality, social behavior, and economic structures (31, 32). Scholars argue that optimizing industrial structures is a vital strategy for enhancing economic resilience. Strengthening innovation capacity enables regions to quickly adjust and achieve sustainable growth following crises. Additionally, policies such as government subsidies and tax incentives help businesses and households weather economic hardships. Integration into global value chains also provides regions with access to critical resources and opportunities (33, 34).
In summary, most existing studies either focus on public health expenditure or analyze economic resilience, but few comprehensively examine the interplay between these two dimensions (35, 36). Furthermore, the majority of research linking public health expenditure and economic development emphasizes economic growth, with limited attention paid to urban economic resilience. This gap underscores the need for empirical analysis at the regional level. Building on prior research, this study explores the relationship between public health expenditure and urban economic resilience using data from 284 Chinese cities at the prefecture level and above between 2008 and 2021. Through both theoretical and empirical approaches, it examines the impact of public health expenditure on urban economic resilience. The marginal contributions of this paper are as follows: (1) it investigates urban economic resilience from the perspective of public health expenditure, examining the relationship between the two and addressing gaps in existing research; (2) it provides a theoretical analysis of the mechanisms through which public health expenditure influences urban economic resilience via technological innovation and per capita GDP, uncovering the underlying link between public health spending and economic resilience; (3) it validates the reliability and applicability of the findings through various robustness checks, including excluding data from municipalities directly under the central government, altering the dependent variables, and adjusting estimation methods; (4) it analyzes the significant regional disparities in public health expenditure across eastern, central, and western cities and explores the potential causes, offering new theoretical insights for regional policy development; and (5) it employs a two-way fixed-effects spatial Durbin model to examine the spatial impact of public health expenditure on urban economic resilience and conducts a spillover effects analysis, aiming to provide recommendations for fostering high-quality regional economic development.
3 Theoretical foundations and research hypotheses 3.1 Direct impact of public health expenditure on urban economic resiliencePublic health expenditure directly enhances urban economic resilience by improving public health, upgrading labor quality, and strengthening the economy’s ability to withstand risks. By improving healthcare conditions, reducing the spread of diseases, and increasing labor productivity, public health spending mitigates health-related risks and social burdens that impact economic operations. Furthermore, it drives the growth of healthcare-related industries, creating employment opportunities and injecting new vitality into local economies (37). Equitable distribution of public health resources helps narrow regional disparities in access to medical care, promoting balanced allocation of economic resources and improving overall economic resilience. By advancing healthcare infrastructure and emergency management systems, public health spending significantly strengthens urban preparedness for crises. In the event of natural disasters or pandemics, cities can recover economic activity more quickly, shortening the recovery period. More importantly, increased public health spending fosters confidence in the future among residents, encouraging consumption and investment, and ultimately creating a favorable social environment for economic growth (38).
3.2 Indirect impact of public health expenditure on urban economic resiliencePublic health expenditure indirectly enhances urban economic resilience through technological innovation. First, it provides critical financial support for research and development in the medical sector, driving advancements in innovative drugs, medical devices, and diagnostic technologies. These innovations improve the efficiency of disease prevention, diagnosis, and treatment, reducing public health risks and bolstering the economy’s capacity to withstand shocks (39). Second, public health expenditure facilitates the upgrading of the medical technology industry by integrating advanced technologies such as biotechnology, artificial intelligence, and big data. These advancements inject new momentum into the economy, enhance the efficiency and coverage of public health services, and improve the adaptive and regenerative capacity of urban economies. Additionally, technological innovation in public health significantly improves cities’ emergency management capabilities. Innovations such as vaccine development, rapid diagnostic tools, and big data monitoring systems enable governments to respond swiftly to public health crises, minimizing disruptions to economic activity (40).
Public health expenditure also strengthens urban economic resilience by boosting per capita GDP. Improved healthcare infrastructure and higher-quality services contribute to better public health outcomes, increasing labor productivity and efficiency. A healthier workforce reduces the disruptive effects of illness on economic activities, raising labor force participation and driving economic growth. These factors support the growth of per capita GDP, providing cities with a more stable economic foundation and enhancing their capacity to resist and recover from external shocks (41). Moreover, public health expenditure optimizes social resource allocation and reduces health inequalities, ensuring that more people have equitable access to medical services. This improves overall social welfare, increases residents’ willingness to consume and invest, and drives income growth and economic development, creating greater economic buffers (42). As public health and income levels rise, demand for high-quality services also increases, spurring the development of high-value-added industries such as healthcare and service sectors. This diversification broadens economic growth channels, enhances economic flexibility, and further consolidates urban economic resilience (43).
4 Model, data, and methods 4.1 Model designThis study adopts a mediation effect model to analyze both the direct impact of public health expenditure on urban economic resilience and its indirect effects through mediating variables. The objective is to comprehensively reveal the mechanisms through which public health expenditure influences urban economic resilience.
Mediation effect analysis introduces mediating variables to clarify the intrinsic relationship between the primary explanatory variable and the dependent variable. This study identifies two key pathways: Public health expenditure promotes urban economic resilience through technological innovation. Public health expenditure indirectly enhances urban economic resilience by influencing per capita GDP. From an empirical perspective, if public health expenditure-induced changes in technological innovation and per capita GDP significantly improve urban economic resilience, these variables can be regarded as mediators. The two primary methods for mediation effect analysis are:
Stepwise Regression Method: This approach calculates the contribution of each independent variable to the dependent variable, constructing a regression model with strong explanatory power while maintaining low complexity.
Coefficient Product Method: This includes tests such as the Sobel test and the Bootstrap test. Compared to stepwise regression, the Sobel test is a widely used significance testing method for determining whether a mediating variable significantly links the independent and dependent variables.
Based on these theoretical foundations, this study first applies the stepwise regression method for preliminary validation and then employs the Sobel test to ensure the robustness of the results. Accordingly, a baseline regression model (Equation 1) and a mediation effect model (Equations 2, 3) are constructed to conduct the analysis and validation.
resit=β0+β1pubit+∑jβj×control+μt+δi+εit (1) Mit=α0+α1pubit+∑jαj×control+μt+δi+εit (2) resit=γ0+γ1pubit+γ2Mit+∑jγj×control+μt+δi+εit (3)Among the variables, resitrepresents urban economic resilience, pubit denotes public health expenditure, and Mit refers to the mediating variables, which in this study include technological innovation and per capita GDP. The index i = 1, 2, 3,…, 284 represents China’s 284 prefecture-level and above cities, while t = 2008, 2012,…, 2021 represents the year variable. Control includes control variables, εit is the random disturbance term, μt accounts for the time fixed effects, and δi captures city-specific fixed effects. Coefficients α , βand γ represent the respective coefficients.
4.2 Variable selection(1) Urban Economic Resilience ( resit ). Urban economic resilience is defined in this paper as a city’s ability to resist, recover, renew, and reconstruct in response to external uncertainties. The strength of this resilience can be measured using the sensitivity index method. With the actual GDP growth rate as the core indicator, this approach not only dynamically reflects the characteristics of urban economic fluctuations but also effectively controls for the influence of national economic cycle variations, ensuring the objectivity and comparability of the measurement. Furthermore, the sensitivity index method quantifies the strength of urban economic resilience while maintaining the continuity and consistency of the indicator, facilitating both long-term vertical tracking and horizontal comparisons across regions. The calculation formula (Equation 4) is as follows:
resiit=ΔGDPr,t/GDPr,t−1ΔGDPn,t/Gn,t−1 (4)Here, resit represents urban economic resilience, ΔGDPr,t/GDPr,t−1denotes the GDP growth rate of city i in year t, and ΔGDPn,t/GDPn,t−1 indicates the national GDP growth rate in year t. To ensure comparability, the continuity of the sensitivity index is maintained in this study.
(2) Explanatory Variable: Public Health Expenditure ( pubit ). Per capita urban health expenditure offers a strong theoretical foundation and statistical advantages. It accurately reflects individual-level benefits, enhances the reliability of cross-city comparisons, and mitigates the influence of population size and economic level. This provides a more robust framework for analyzing the relationship between public health expenditure and urban economic resilience. In this study, per capita urban health expenditure is used as a proxy for public health expenditure.
(3) Mediating Variables. Technological Innovation ( lninnoit ): Technological innovation plays a pivotal mediating role in the relationship between public health expenditure and urban economic resilience. By advancing the modernization of public health systems, fostering the development of the health sector, accelerating economic structural upgrades, and enhancing social stability and resource allocation efficiency, technological innovation strengthens the impact of public health spending, thereby bolstering urban economic resilience. This study analyzes the number of patent applications in each city to assess the level of technological innovation and its regional disparities, illustrating how public health expenditure fosters urban economic resilience through technological advancement. Using patent applications as a measure of technological progress is both scientifically sound and practical. Patent data directly reflects the output of technological innovation and is closely linked to public health expenditure in areas such as research and development investment and technological innovation. In this study, the number of patent applications per 10,000 people is measured using the logarithmic value.
Per Capita GDP ( lnpergdpit ): Per capita GDP serves as a key mechanism through which public health expenditure fosters urban economic resilience. It effectively captures the impact of public health spending on multiple dimensions, including economic growth, the labor market, economic structural adjustments, and social equity and stability. By increasing public health expenditure, labor productivity is directly enhanced, leading to higher per capita GDP, which in turn improves public health, optimizes industrial structure, promotes social welfare and equity, and ultimately strengthens urban economic resilience. In this study, the natural logarithm of per capita GDP is used as the measurement.
(4) Control Variables. The study includes the following control variables to account for additional factors influencing urban economic resilience: Industrial Structure: Measured as the ratio of value-added from the tertiary sector to value-added from the secondary sector. Openness to Trade: Measured as the ratio of total imports and exports (converted to RMB using the annual exchange rate) to GDP. Urban Land Use: Measured as the logarithm of the urban built-up area. Population Size: Measured as the logarithm of the urban permanent population. Urban Resident Income: Measured as the logarithm of the average income of urban residents. Scientific Expenditure: Measured as the ratio of scientific research expenditure to GDP.
4.3 Data sourcesThe 2008 global financial crisis prompted China to implement an economic stimulus plan, alongside significant increases in public health investment. Concurrently, the new healthcare reform plan was introduced, with the government expanding public health expenditure, thereby reflecting the long-term effects of this policy shift on urban economic resilience. Based on this context, the data used in this study consists of panel data from 284 cities at or above the prefecture level, spanning from 2008 to 2021. The data sources include the China Regional Economic Statistical Yearbook, China Urban Statistical Yearbook, and statistical bulletins from various provinces and cities. Missing data were addressed using linear interpolation. Descriptive statistics for the main variables are provided in Table 1.

Table 1. Descriptive statistical analysis.
5 Estimation and result 5.1 Benchmark regression analysisBefore empirically examining the relationship between public health expenditure and urban economic resilience, it is essential to address potential collinearity and data stationarity issues among the dependent variable, key explanatory variable, and control variables to avoid spurious regression results. A Variance Inflation Factor (VIF) test was conducted, showing a mean VIF of 2.19 and a maximum value of 3.28, both well below the critical threshold of 10. These results confirm the absence of multicollinearity among the variables, allowing for their inclusion in the regression model. Furthermore, a Hausman test comparing two-way fixed effects and two-way random effects models rejects the null hypothesis at the 1% significance level, validating the appropriateness of using a two-way fixed effects model for the analysis.
The two-way fixed effects model effectively controls for both time and individual fixed effects, thereby improving the accuracy of estimates concerning the impact of public health expenditure on urban economic resilience. This approach mitigates omitted variable bias, enhancing both the reliability and robustness of the results. The regression results using the two-way fixed effects model are presented in Table 2. Column (1) reports the results without control variables, where the coefficient for public health expenditure is 0.105 and significant at the 1% level, indicating that public health expenditure has a positive and significant effect on urban economic resilience. Columns (2) to (7) progressively introduce control variables, including industrial structure, foreign trade, urban construction land, population size, urban residents’ income, and scientific expenditure, using a stepwise regression approach. Across all models, the coefficients for public health expenditure remain significant at the 1% level, demonstrating its robust and stable positive impact on urban economic resilience. This finding suggests that public health expenditure directly strengthens a city’s ability to manage public health crises, reducing the adverse economic effects of such crises, ensuring the continuity of economic activities, and enhancing the city’s capacity to withstand shocks. Consequently, public health expenditure plays a crucial role in supporting the long-term stability and development of urban economies.
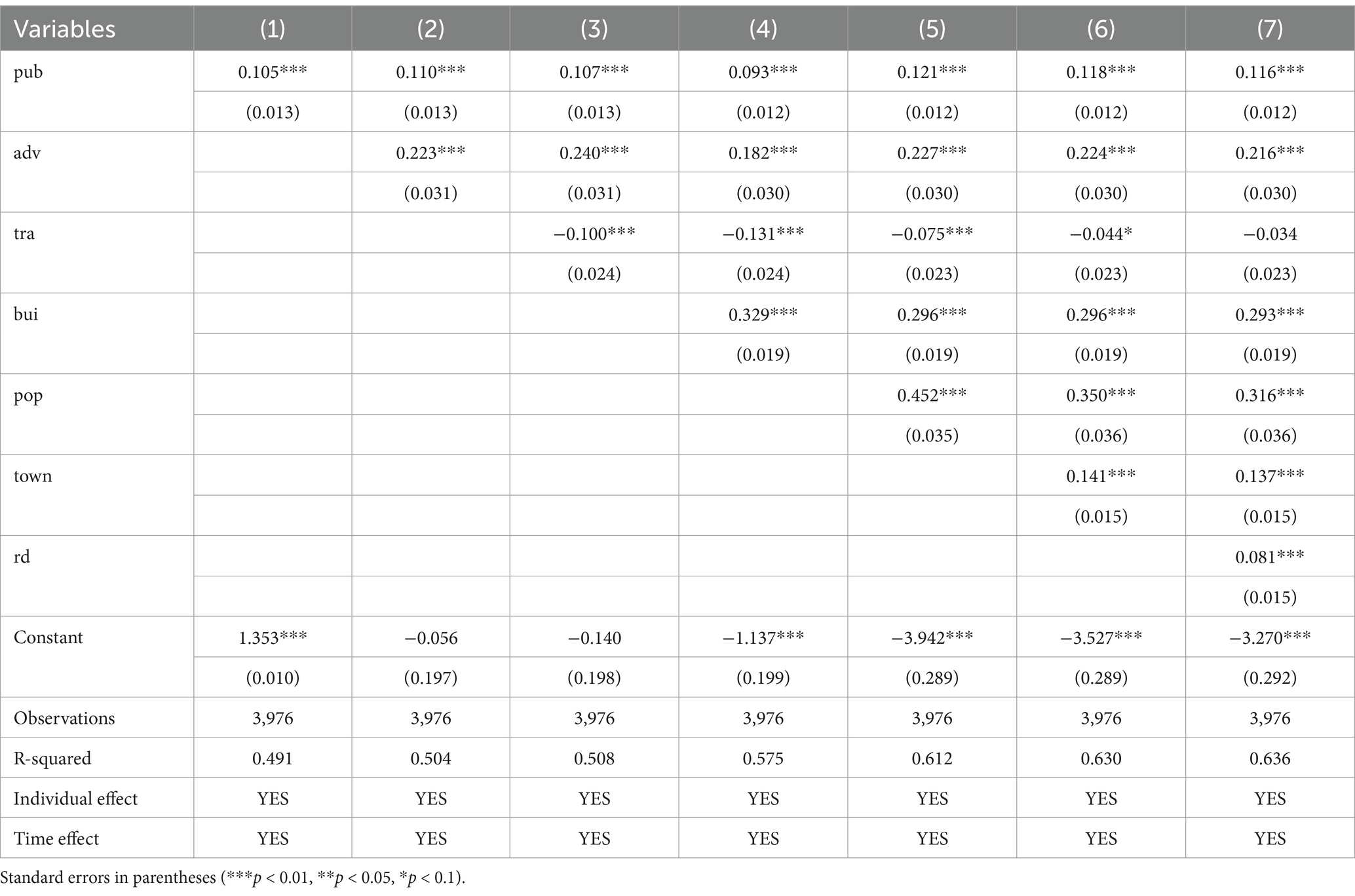
Table 2. Basic regression results.
The regression results indicate that several control variables—industrial structure, urban construction land, population size, urban residents’ income, and scientific expenditure—positively and significantly contribute to urban economic resilience, while foreign trade openness has a negative impact: A diversified industrial structure reduces reliance on a single industry, enabling cities to spread risks during economic crises or industrial shocks. This diversification enhances economic resilience and stability. Optimizing and rationally allocating urban construction land improves urban environments, unlocks growth potential, and strengthens the city’s capacity for sustainable economic development. High population size fosters greater consumer demand, creating larger and more diverse markets. This sustained demand provides consistent momentum for economic recovery and growth. Higher incomes not only boost consumption but also strengthen savings capacity. Under balanced market conditions, increased savings can translate into government expenditure and corporate investments, supporting infrastructure development and economic resilience. Greater investment in research and development drives technological advancements, fosters innovation, and diversifies economic systems. This provides a strong foundation for economic recovery and sustained growth, enhancing resilience against future shocks. Conversely, the coefficient for foreign trade openness is negative, indicating that higher levels of trade dependence increase a city’s exposure to external market fluctuations. During periods of global economic instability, external shocks are more likely to propagate through trade, capital flows, and supply chains, intensifying domestic economic volatility and undermining resilience.
5.2 Robustness tests 5.2.1 Excluding municipalitiesDue to their unique administrative status, industrial concentration, and resource advantages, municipalities often exhibit significantly different levels of economic development, policy support, and public health expenditure compared to other regions. These differences may introduce bias into the overall regression results. To address this, the municipalities were excluded from the sample to better reflect the actual development dynamics of ordinary regions and to provide a clearer understanding of the relationship between public health expenditure and urban economic resilience. Column (1) of Table 3 presents the results after excluding the four municipalities. The coefficient for public health expenditure remains significantly positive at the 1% level, confirming the robustness of the baseline regression model.
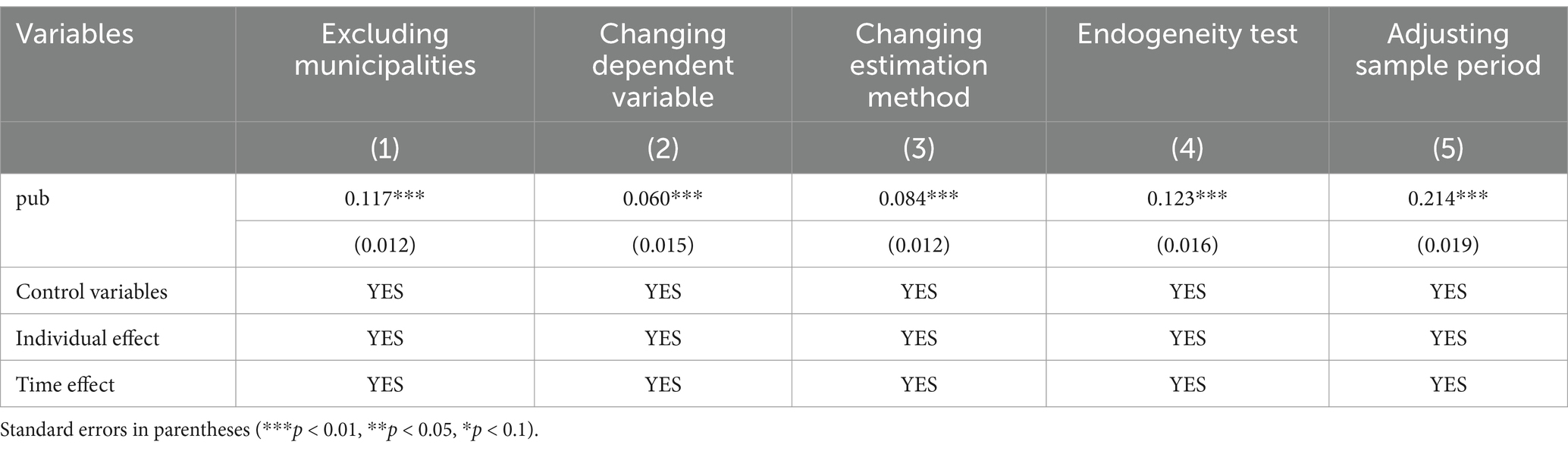
Table 3. Robustness test.
5.2.2 Changing the dependent variableThe findings thus far indicate that public health expenditure contributes to the enhancement of urban economic resilience. However, it remains necessary to determine whether this effect stems from the intrinsic role of public health or whether the integration of urban economic resilience in the economic domain influences the baseline regression results. To verify the reliability and generalizability of the model and ensure that the conclusions are not biased or overly dependent on the choice of the dependent variable, the robustness test is conducted by modifying the dependent variable. In this test, urban economic resilience is considered as a dynamic adjustment process. Drawing on the concept of the deviation share method, urban resilience is calculated by assessing the deviation of each city’s annual actual GDP from its actual GDP in 2008. The formula (Equation 5) used to calculate urban economic resilience for the 2008–2021 period is as follows:
resiit=GDPit−GDPi2008GDPi2008 (5)Where GDPit is the actual GDP of city i in year t, GDPi2008 is the actual GDP of city i in 2008, and resiit represents the urban economic resilience of city i during period t. A higher value for this indicator suggests that a city possesses stronger stability and corrective capacity, enabling it to navigate complex and dynamic internal and external environments more effectively. Such cities are better equipped to mitigate short-term shocks, restore economic order swiftly, optimize growth trajectories, reallocate resources, and achieve rapid economic recovery. Column (2) of Table 3 presents the results of this robustness test using the modified dependent variable. The regression results indicate that the coefficient for public health expenditure remains significantly positive at the 1% level, with the same direction as observed in the baseline regression. This further confirms the robustness of the baseline model and reinforces the reliability and scientific validity of the relationships between the variables.
5.2.3 Revising the estimation approachThe Tobit model, when applied within a fixed-effects framework for panel data analysis, leverages cross-sectional variations between individuals as well as temporal dynamics. This dual capacity allows the model to maximize the use of panel data, enhancing the efficiency of parameter estimation. It is particularly suited for contexts where truncated data and individual-specific effects coexist. Given that the quantified measures of urban economic resilience in this study are all non-negative, a fixed-effects panel Tobit model is adopted to more precisely examine the relationship between public health expenditure and urban economic resilience.
The model (Equation 6) can be expressed as follows:
res∗it=β0+β1pubit+β2Xit+ξi+εit (6)where res∗it represents the latent (unobserved) urban economic resilience for city i at time t; pubit denotes the core explanatory variable, public health expenditure; β1 is the coefficient of interest; ξi captures individual fixed effects, accounting for time-invariant heterogeneity across cities; and εit is the error term.
The fixed-effects panel Tobit model accommodates the non-standard distribution resulting from the interplay of fixed effects and data truncation. Traditional Ordinary Least Squares (OLS) estimation methods are therefore inadequate, and conditional maximum likelihood estimation (MLE) is instead employed. As shown in column (3) of Table 3, the regression results align closely with those from the baseline model, demonstrating that the baseline results are not overly dependent on specific model specifications. This reinforces the generalizability and robustness of the conclusions.
5.2.4 Addressing endogeneityWhile public health expenditure likely exerts a positive effect on urban economic resilience, it is equally plausible that regions with higher resilience could influence public health spending, introducing potential reverse causality. This bidirectional relationship could result in endogeneity, wherein public health expenditure is correlated with the error term, compromising the consistency and unbiasedness of the regression estimates. To address this issue, a partial linear instrumental variable model (Equations 7, 8) based on double machine learning is constructed:
resit=θpub+gXit+εit (7)where IVitserves as the instrumental variable for pubit . In this study, we use the average public health expenditure of other cities within the same province during the same year as the instrumental variable. This measure reflects inter-city interactions in public health spending within a region, satisfying the relevance criterion for instrumental variables. Furthermore, historical data on public health expenditures from the previous year at the provincial level is used, as it is unlikely to be directly related to the current level of urban economic resilience, satisfying the exogeneity assumption. Using this methodology, an endogeneity test was performed, and the results are presented in column (4) of Table 3. The regression coefficient for public health expenditure is 0.123, statistically significant at the 1% level. These findings confirm that public health expenditure positively contributes to urban economic resilience, supporting the consistency and reliability of the baseline regression results.
5.2.5 Adjusting the study periodThe outbreak of COVID-19 in December 2019 triggered a sharp increase in public health expenditures. These abnormal changes in expenditure during the pandemic may render the regression results overly sensitive to data from these exceptional years, thereby affecting the model’s robustness. Additionally, the pandemic posed unprecedented challenges to urban economic resilience, with varying capacities among cities to respond. This may have altered the relationship between the variables and increased the instability of the regression results. To address this concern, the sample period was restricted to 2010–2019, excluding the years influenced by the pandemic. The regression analysis was then re-conducted, with results shown in column (5) of Table 3. The coefficient for public health expenditure is 0.214, statistically significant at the 1% level. These findings remain consistent with those from the baseline regression, confirming the robustness of the results when accounting for potential temporal effects.
5.3 Mechanism analysisThe preceding analysis established the positive effect of public health expenditure on urban economic resilience. The following section explores the underlying mechanisms driving this relationship. Specifically, we investigate whether technological innovation and per capita GDP serve as channels through which public health expenditure influences urban economic resilience. To this end, a stepwise regression approach is adopted. The regression results based on Models 2 and 3 are presented in Table 4.
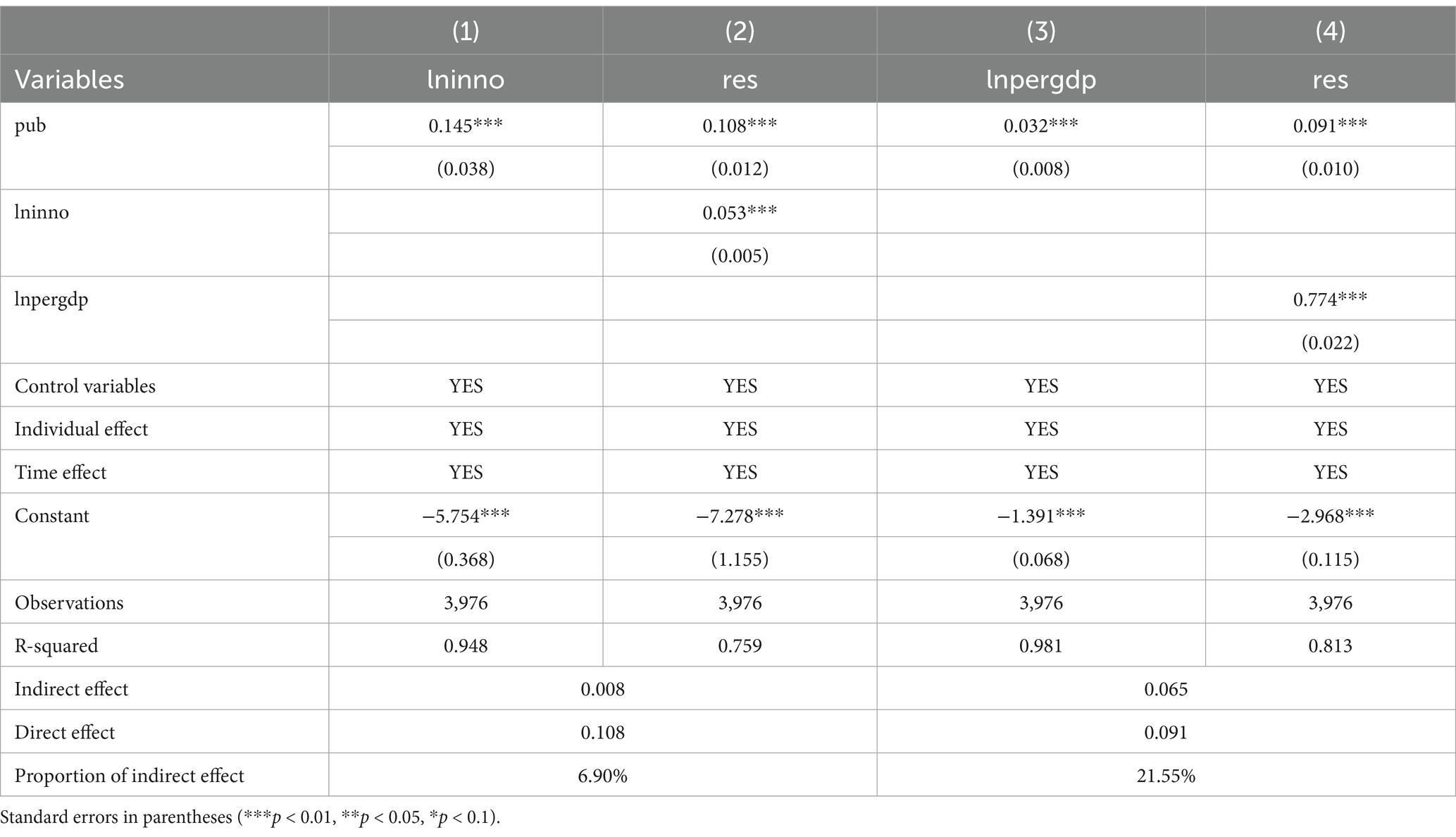
Table 4. Results of mechanism analysis.
Column (1) of Table 4 shows that public health expenditure significantly enhances urban technological innovation. This increase drives the integration of disciplines such as medicine, information technology, and big data, addressing the specific needs of the public health sector for precise monitoring, disease diagnosis, and efficient prevention strategies. Moreover, it fosters interdisciplinary collaboration and accelerates the application of innovative technologies, leading to breakthroughs in emerging cross-disciplinary fields. Column (2) incorporates technological innovation into the regression model, where the mediating variable remains statistically significant at the 1% level. The Sobel test produces a Z-statistic of 3.59, indicating strong statistical significance, with the mediating effect accounting for 6.90% of the total effect. These findings suggest that public health expenditure promotes technological innovation, thereby enhancing cities’ ability to resist external shocks. This study further highlights that sustained investment in public health accelerates the development of advanced technologies, including telemedicine, diagnostic tools for public health emergencies, and health-focused big data solutions. These innovations optimize medical resource allocation, improve the efficiency and accuracy of healthcare services, significantly shorten emergency response times, and reduce healthcare costs. Collectively, these advancements enhance urban resilience, optimize structural configurations, and help cities transition to a new equilibrium in economic resilience.
Column (3) of Table 4 indicates that public health expenditure (pub) has a significant and positive effect on per capita GDP. This result suggests that public health investment improves the overall health of residents, reduces the incidence of disease, and alleviates the financial burden of healthcare. These improvements enable a more productive workforce, boosting labor efficiency and driving per capita GDP growth. Column (4) demonstrates that both public health expenditure and per capita GDP have statistically significant positive effects at the 1% level. This finding indicates that public health expenditure indirectly enhances urban economic resilience by increasing per capita GDP. The Sobel test confirms this relationship, with a Z-statistic of 3.97 and the mediating effect of per capita GDP accounting for 21.55% of the total effect. This substantial mediating role underscores the importance of per capita GDP as a pathway through which public health expenditure enhances urban economic resilience. The analysis further reveals that robust public health services reduce the prevalence of chronic illnesses, occupational diseases, and infectious diseases, enabling workers to participate in economic activities with greater energy and efficiency. This “health dividend” increases individual economic contributions and enhances collective labor productivity, ultimately strengthening the economic competitiveness of cities. Over the long term, the health dividend not only improves individual productivity but also enhances overall urban resilience by boosting collective economic performance.
5.4 Heterogeneity analysisUsing the economic regional divisions defined by the National Bureau of Statistics, the sample cities are grouped into three categories: 100 cities in the eastern region, 96 cities in the central region, and 84 cities in the western region. The regression results are presented in Columns (1), (2), and (3) of Table 5. For cities in the eastern region, the coefficient of public health expenditure is significantly positive at the 1% level, with the largest magnitude of 0.361. This indicates that public health expenditure has a clear and substantial promoting effect in this region. For cities in the central region, the coefficient is also significantly positive at the 1% level, with a moderate magnitude of 0.42, demonstrating a similar but slightly less pronounced effect. In contrast, the coefficient for cities in the western region is −0.029, non-significant, and the smallest among the three regions, suggesting that public health expenditure has a weak and non-significant suppressing effect on economic resilience in this area. These results reveal regional disparities in the response to public health expenditure, reflecting the uneven nature of regional economic development. In the eastern region, where economic development is more advanced and infrastructure is more robust, public health expenditure achieves higher marginal returns. This expenditure is more effectively converted into productivity gains and social stability, thereby exerting a significant positive impact on urban economic resilience. In the central region, where economic development is intermediate, public health expenditure helps address developmental gaps and improves public health outcomes. However, due to a relatively weaker economic base and less efficient resource allocation, the effect is somewhat lower than in the eastern region. Meanwhile, in the western region, where public health infrastructure is underdeveloped, new investments are often directed toward basic infrastructure construction. Such investments may take longer to yield economic benefits and may even temporarily suppress economic resilience due to the scale and time required for implementation.
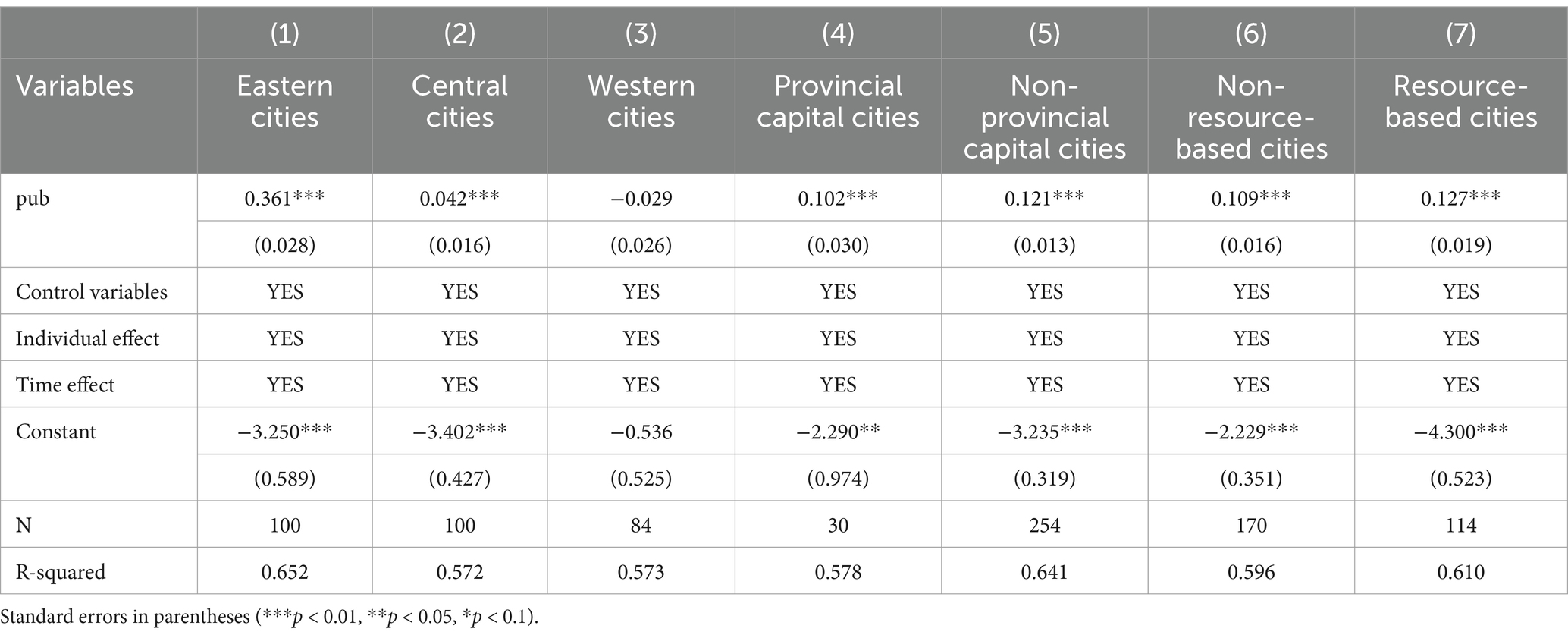
Table 5. Heterogeneity analysis.
To explore the differing effects of public health expenditure on economic resilience in provincial capital cities versus non-capital cities, the sample is divided into 30 provincial capital cities and 254 non-capital cities for regression analysis. The results are shown in Columns (4) and (5) of Table 5. For provincial capital cities, the coefficient for public health expenditure is 0.102, which is statistically significant at the 1% level, indicating that public health expenditure has a positive impact on economic resilience in these cities. For non-capital cities, the coefficient is 0.121, also statistically significant at the 1% level, showing that public health expenditure similarly promotes economic resilience. Notably, the coefficient for non-capital cities is larger than that for provincial capital cities, suggesting that public health expenditure has a more substantial impact on the economic resilience of non-capital cities.
The findings of the study reveal that public health expenditure has a more significant effect on improving the economic resilience of non-provincial capitals compared to provincial capitals. This is because non-provincial capitals typically have weaker public health infrastructure and resource allocation, making their economic resilience more vulnerable. In contrast, provincial capitals already possess stronger economic resilience, making further improvements more challenging. As a result, non-provincial capitals have greater potential for enhancing their economic resilience, which explains why public health expenditure has a more substantial impact in these cities.
Following the National Plan for Sustainable Development of Resource-Based Cities (2013–2020) and the 14th Five-Year Plan for Promoting High-Quality Development in Resource-Based Areas, the 284 cities in the sample are categorized into 170 non-resource-based cities and 114 resource-based cities. The regression results are presented in Columns (6) and (7) of Table 5. The results show that public health expenditure has a statistically significant positive effect on economic resilience at the 1% level in both types of cities. Specifically, the coefficient for non-resource-based cities is 0.109, while for resource-based cities, it is 0.127. These findings suggest that the positive impact of public health expenditure on economic resilience is more pronounced in resource-based cities. The study finds that resource-based cities, confronted with challenges such as resource depletion and environmental pollution, must urgently undergo industrial transformation to strengthen their sustainability. Increasing public health expenditure can improve the living conditions of urban residents and enhance the economic resilience of cities.
6 Further analysis based on spatial effectsAs the economy transitions toward high-quality development, the free flow of labor, capital, and technology has significantly enhanced intercity collaboration and interaction, strengthening the spatial interconnections of urban economic resilience. Cities with high levels of public health expenditure often act as exemplars, guiding neighboring cities to improve resource allocation efficiency. This demonstration effect expands through imitation, amplifying the overall impact. From a spatial perspective, this study systematically examines the spatial mechanisms between public health expenditure and urban economic resilience, focusing on whether public health expenditure enhances economic resilience through spatial spillover effects.
6.1 Spatial autocorrelation testSpatial autocorrelation is a prerequisite for spatial regression models. Testing for spatial autocorrelation ensures the inclusion of spatial factors, avoiding biases caused by traditional models that overlook spatial dependencies. This test also reveals whether variables influence adjacent regions, i.e., whether spatial spillover effects exist. In this study, Moran’s I index is constructed using a spatial adjacency matrix and a spatial economic-geographic nested matrix to test for spatial effects between public health expenditure and urban economic resilience. Table 6 reports the Moran’s I indices for urban economic resilience from 2008 to 2021 under both matrices. The results indicate that urban economic resilience passes the significance test at the 1% level, with the mean Moran’s I index greater than 0. This confirms the existence of significant positive spatial relationships. The study reveals that the underlying logic of economic networks between cities highlights the crucial role of enhancing the economic resilience of core cities in strengthening the risk resistance of surrounding cities and the broader region, particularly within the context of regional integration and coordinated development.
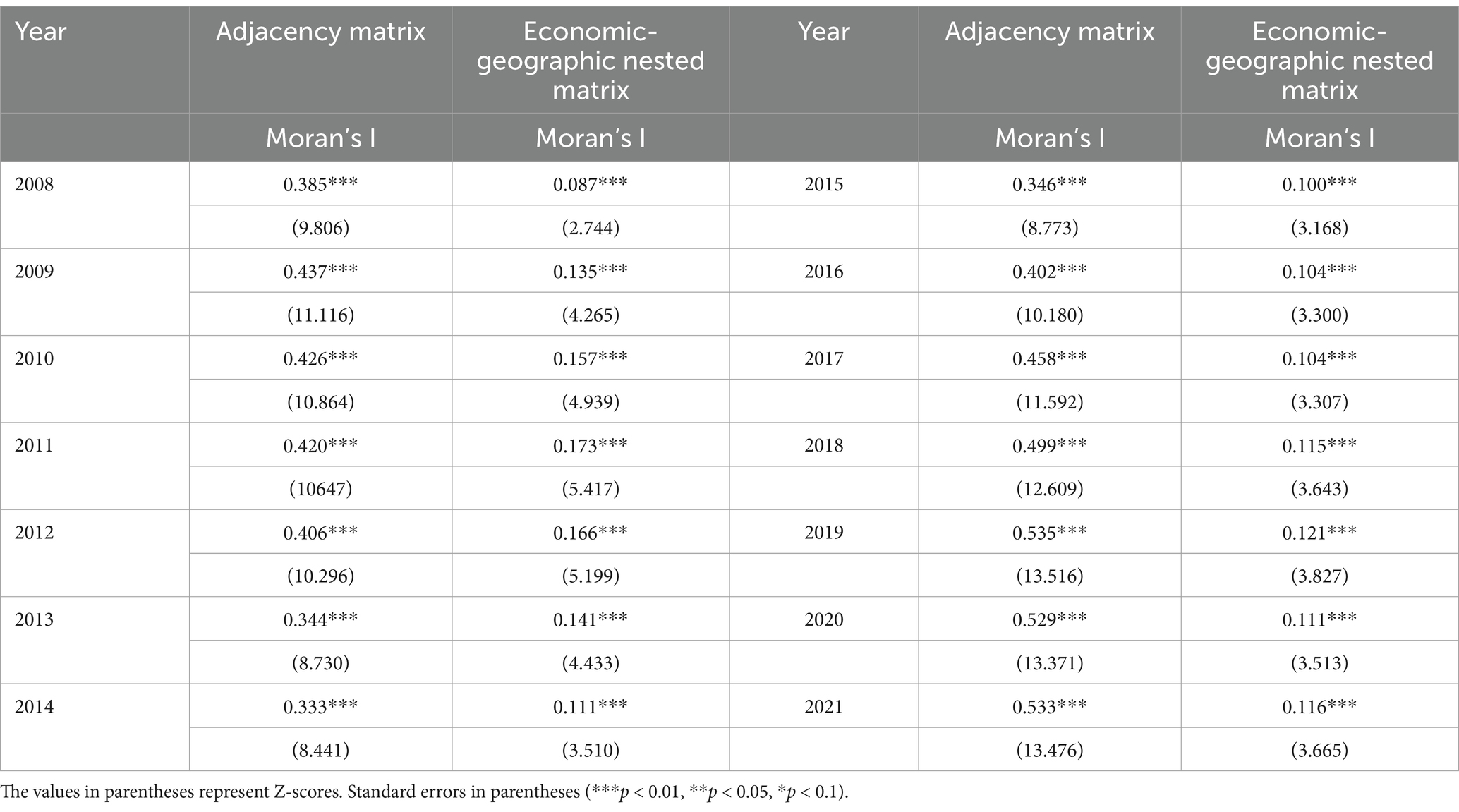
Table 6. Moran’s I index for urban economic resilience.
6.2 Spatial econometric model designTo evaluate whether public health expenditure exhibits spatial spillover effects on urban economic resilience, this study employs the OLE-SAR and SEM-SDM modeling frameworks, establishing the following regression models (Equations 9, 10):
resit=μi+γt+ρWresit+β1pubit+β2Xit+θ1Wpubit+θ1WXit+ωit (9)
留言 (0)