
記住我
Rheumatoid arthritis (RA) is an idiopathic disease characterized by inflammation in synovial tissues of joints, cartilage, and bones (1, 2). RA is thought to be driven by genetic and epigenetic factors, but environmental factors such as cigarette smoke and dust exposure also play crucial roles (3–5). Uncontrolled RA can lead to joint degradation, severe disability, reduced quality of life, comorbidities, and premature death, posing a significant societal burden (6–8). Approximately 70% of RA patients in India suffer from anxiety and depression (9). A cross-sectional, hospital-based study conducted in a tertiary care private multi-specialty hospital in Tamil Nadu revealed that the average annual medical expenditure for treating RA was 44,700 rupees ($543), with a median of 39,210 rupees ($476) (10). The global prevalence of RA varies, with an estimated 0.5 to 1% of adults affected (1, 11). The prevalence is generally higher in industrialized countries, possibly due to environmental risk factors, genetic predispositions, and underreporting in other regions (12). Recent reviews indicate that the prevalence of RA in India ranges from 0.28 to 0.7%, based on only four studies (13). There is a lack of nationwide epidemiological research on RA in India.
The Global Burden of Disease (GBD) database, established by the Global Burden of Disease Study, is a comprehensive repository maintained by the Institute for Health Metrics and Evaluation (IHME). It systematically quantifies and assesses the impact of major diseases, injuries, and health risk factors globally, regionally, and nationally (14, 15). This study leverages GBD 2021 data to analyze the incidence and prevalence of RA in India and estimates the disease burden and trends across different age groups, providing a basis for developing effective RA prevention and control strategies.
Materials and methods Data sourceThis study uses data from GBD 2019, analyzing data from 1990 to 2021 for both India and globally. The GBD database, maintained by the IHME, assesses the burden of 389 diseases or injuries and 88 risk factors across 204 countries. The GBD database is classified and defined based on the international classification of diseases (ICD) system. The codes for RA are ICD-9-714 and ICD-10-M05, M06, M08 (16, 17).
Search strategyData were retrieved using the GBD Result Tool available on the IHME website. The search was conducted under the “GBD Estimate” tab by selecting “Rheumatoid arthritis,” region, age, time, and study indicators. India comprises 31 geographical units: 28 states, the union territory of Delhi, Jammu and Kashmir combined with Ladakh, and other small union territories combined (Chandigarh, Dadra and Nagar Haveli, Daman and Diu, Puducherry, Lakshadweep, and the Andaman and Nicobar Islands).
Basic indicatorsThe report provides data on the incidence, prevalence, age-standardized incidence rates (per 100,000 persons), and age-standardized prevalence rates (per 100,000 persons) of RA in India from 1990 to 2021, broken down by year, gender, and age group. It also uses age-standardized disability-adjusted life years (DALY) rates (per 100,000 persons) to measure the disease burden caused by RA. The meaning of DALY is the loss of healthy life years due to early death and disability caused by diseases. The DALY consists mainly of years lived with disability (YLDs) and years of life lost (YLLs). The Autoregressive Integrated Moving Average model (ARIMA) was employed to predict RA incidence and DALY from 2022 to 2036 in India. Socio-Demographic Index (SDI) is a comprehensive indicator used to measure the development status of a country or region and is strongly correlated with health outcomes. The study also reports the prevalence rates across 31 geographical units and analyzes the relationship between the SDI and DALY rates in India.
Statistical analysisOur data comes from the GBD database, which provides data on the prevalence of diseases in different years, as well as disability-adjusted life years. We carefully reviewed the data to illustrate the incidence, prevalence and DALY of RA across different age groups and genders in India. Data were age standardized for analysis of morbidity, prevalence, and DLAYs to eliminate age composition disruptions. We use R 4.3.3 software to analyze and visualize the downloaded data.
As all GBD studies are conducted using publicly available data, no ethical approval was required.
Results Prevalence characteristics of RA in IndiaFrom 1990 to 2021, the incidence, prevalence, and DALY rates of RA in India have shown an increasing trend (Figure 1). All age-standardized rates were significantly higher in females than in males. In 2021, the incidence, prevalence, and DALY rates were 2.76–3.38 times higher than in 1990, with female incidence, prevalence, and DALY rates being 2.60–2.93 times those of males. The number of males affected by RA across all age groups increased from 224,505 in 1990 to 704,401 in 2021, while the number of females increased from 594,068 to 2,062,348. The age-standardized incidence rate (per 100,000 persons) in males increased from 6.32 in 1990 to 8.33 in 2021, while in females, it increased from 15.25 to 21.28. The age-standardized prevalence rate (per 100,000 persons) in males increased from 81.47 in 1990 to 113.32 in 2021, while in females, it increased from 220.81 to 315.44. The age-standardized DALY rate (per 100,000 persons) in males increased from 21.01 in 1990 to 23.94 in 2021, while in females, it increased from 49.19 to 57.07 (Table 1).

Figure 1. Incidence, prevalence, DALY, and their age-standardized rates (per 100,000 persons) of rheumatoid arthritis by gender from 1990 to 2021. DALY, disability-adjusted life years.
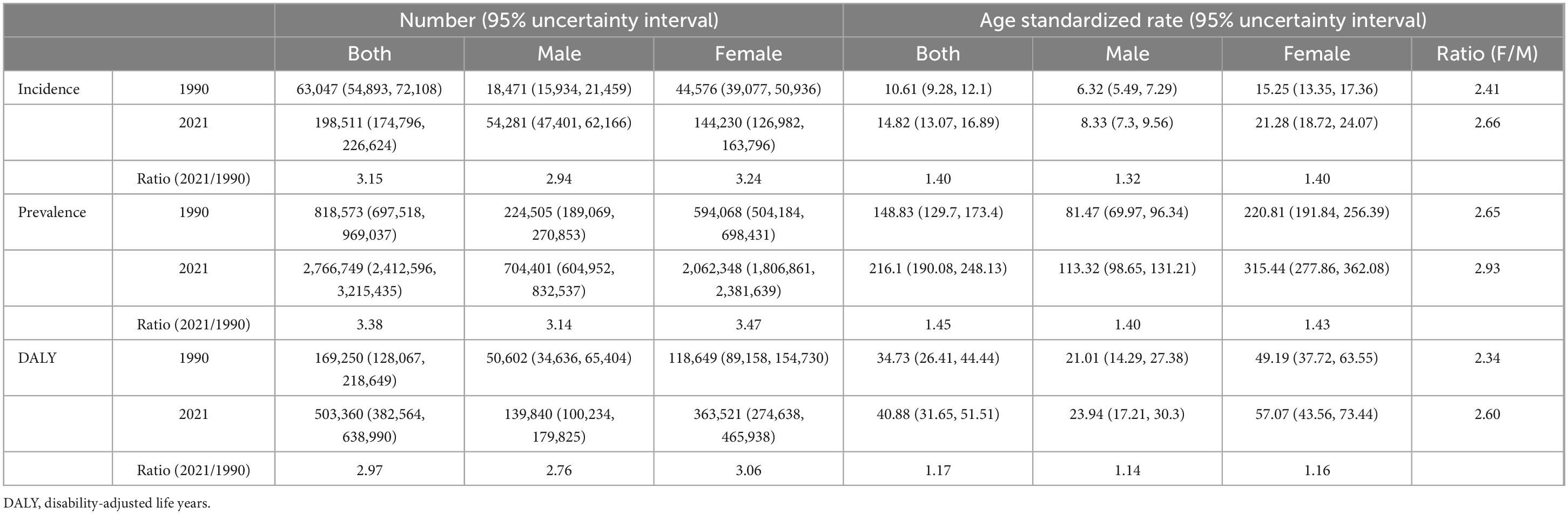
Table 1. Incidence, prevalence, and DALY of rheumatoid arthritis in India, 1990 and 2021.
The age group of 65–69 years showed the highest incidence rate, while the prevalence peaked at 75–79 years (Figure 2). ARIMA predictions suggest that from 2022 to 2036, incidence and DALY rate, will continue to rise, with a more stable trend in males compared to females (Figure 3).
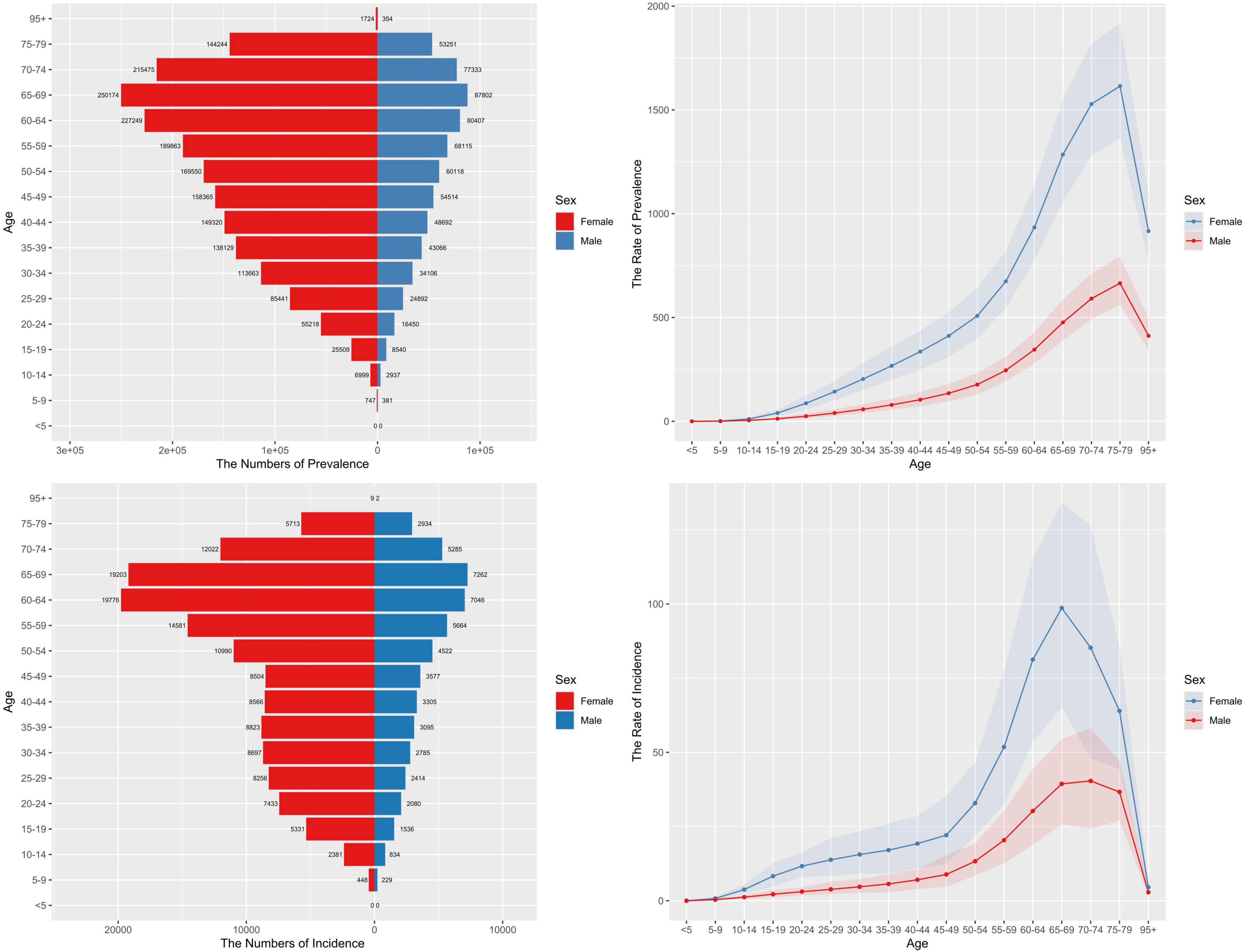
Figure 2. Number and rate (per 100,000 persons) of rheumatoid arthritis cases by age in 2021. DALY, disability-adjusted life years.
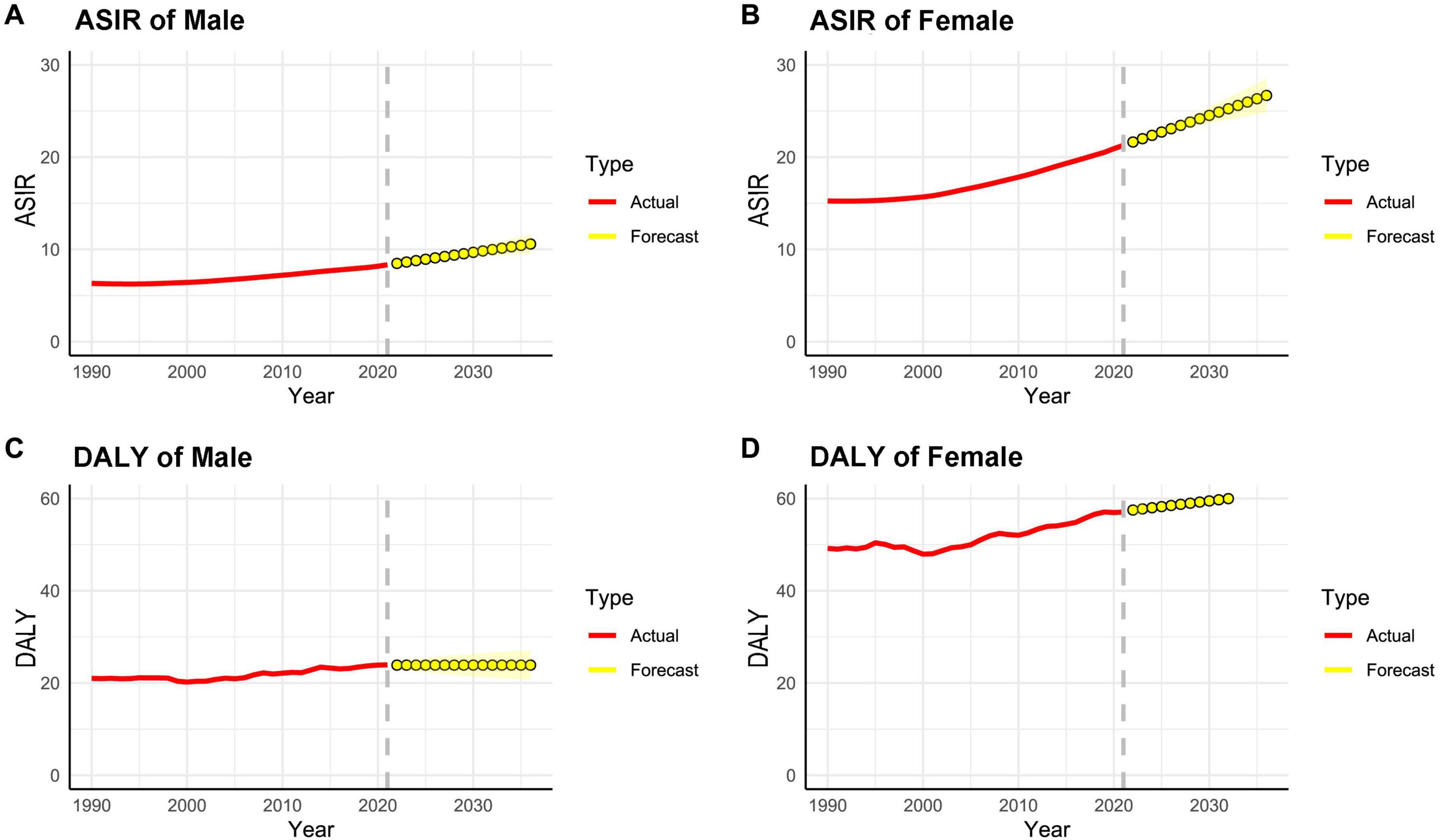
Figure 3. ASIR (A,B) and DALY (C,D) (per 100,000 persons) of rheumatoid arthritis predicted from 2022 to 2036 using ARIMA forecasting. ASIR, age-standardized incidence rate; DALY, disability-adjusted life years.
Geographical characteristics of RA prevalence in IndiaWe observed the DALYs in 31 geographical regions of India (Figure 4). The highest DALYs are in Uttarakhand, followed by Tamil Nadu and Telangana. Significant differences in prevalence were observed across 31 geographical regions (Figure 5). In 2021, Uttarakhand had the highest age-standardized prevalence rate (per 100,000 persons) among males (177.86), while Goa had the lowest (88.74). Among females, Tamil Nadu had the highest rate (401.26), while Madhya Pradesh had the lowest (232.53). Delhi ranked second in female prevalence (392.80) and ninth in male prevalence (131.10). Due to the lack of SDI data for the other small union territories combined, only 30 regions were analyzed (Figure 6). Overall, areas with high SDI showed a higher disease burden, with age-standardized DALY rates (per 100,000 persons) in all 30 regions in 2021 higher than in 1990. The highest DALY rate in 2021 was observed in Uttarakhand (63.40), while the lowest was in Kerala (28.79), despite both regions having similar SDI levels. Interestingly, Delhi, the region with the highest SDI, had a DALY rate (46.79) significantly higher than Goa, the region with the second-highest SDI (39.25).
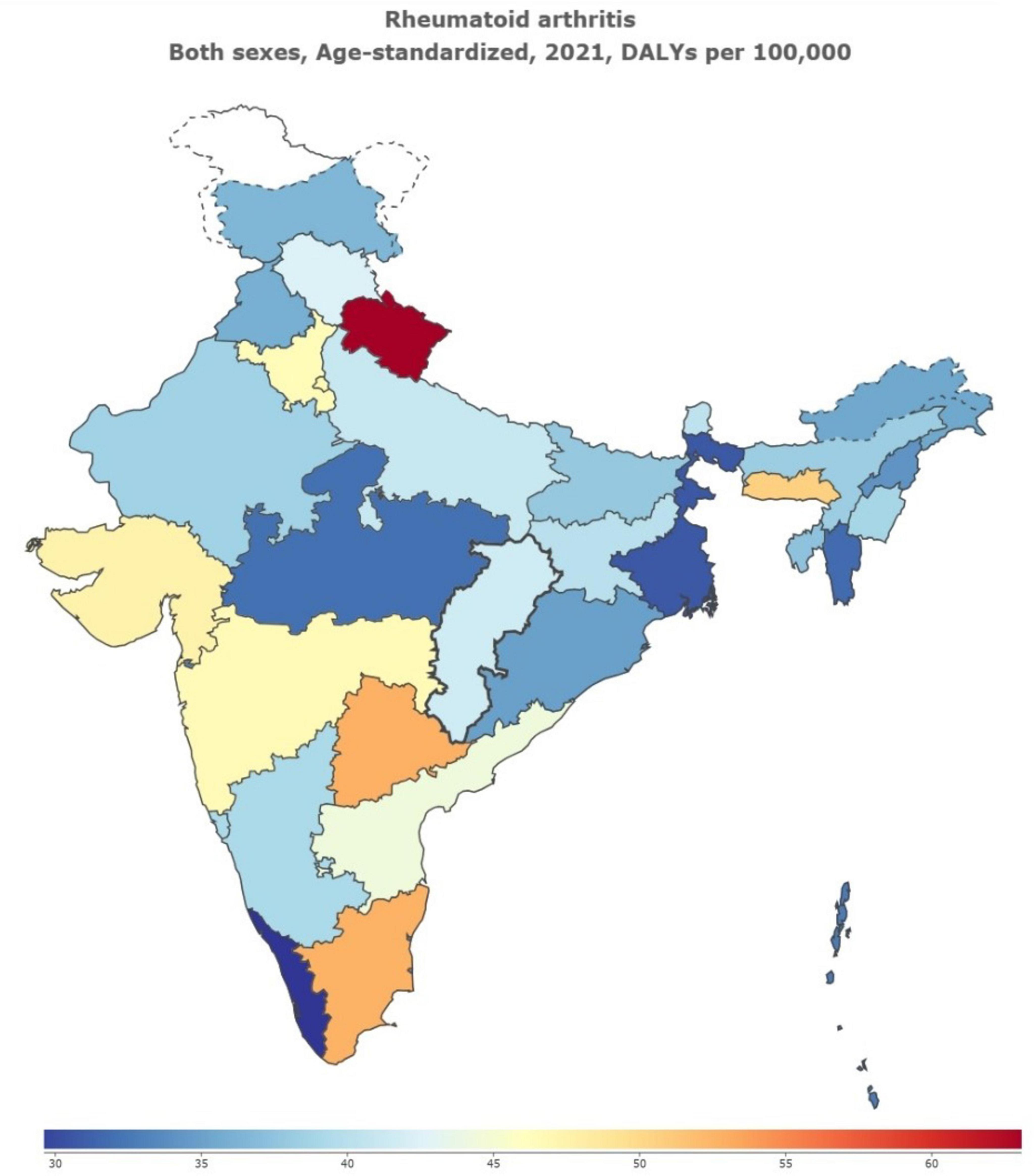
Figure 4. DALYs of Rheumatoid Arthritis in 31 Geographical Regions of India of 2021. DALY, disability-adjusted life years.
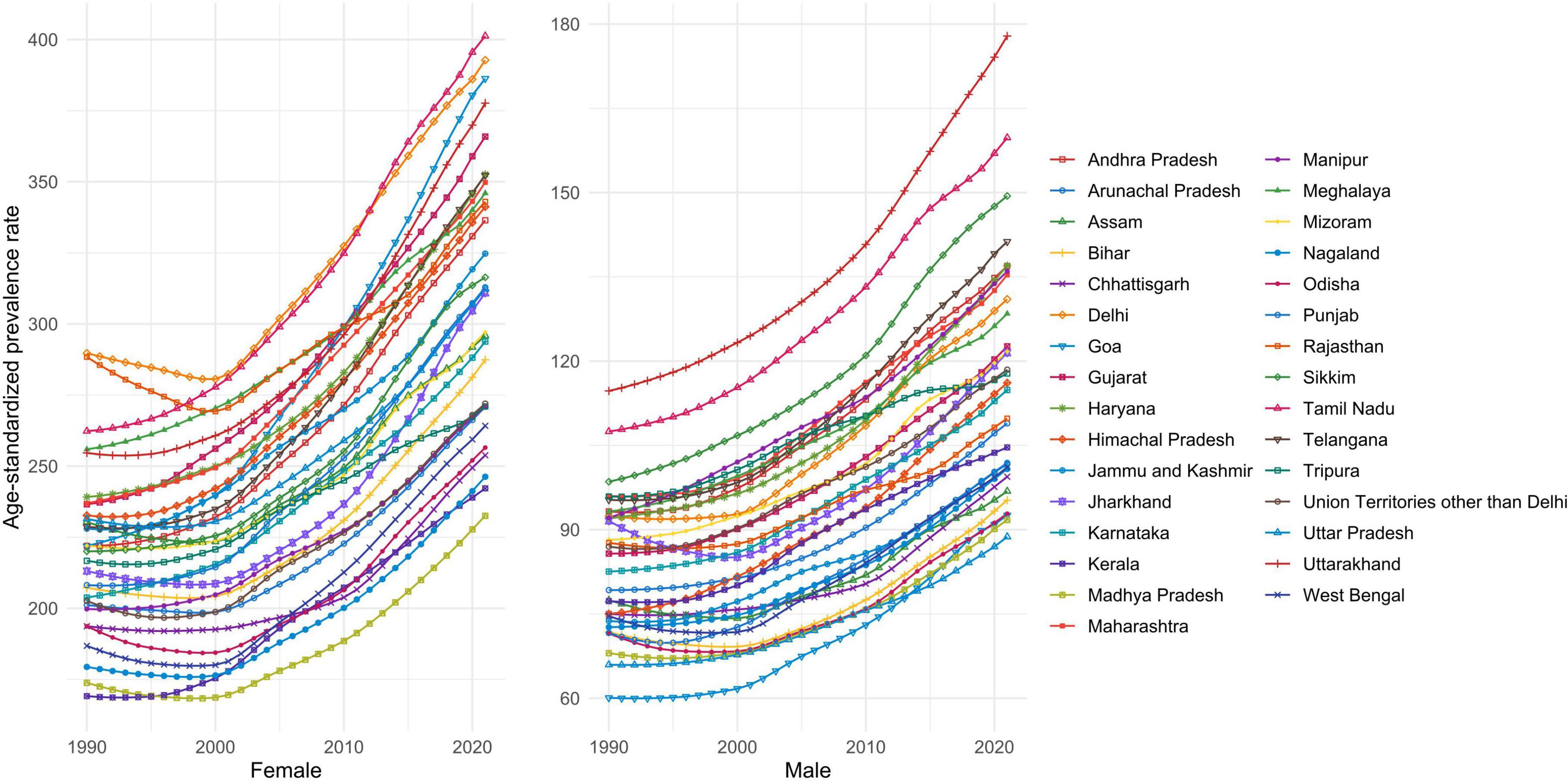
Figure 5. Age-standardized prevalence rates (per 100,000 persons) of rheumatoid arthritis across 31 geographic regions from 1990 to 2021.
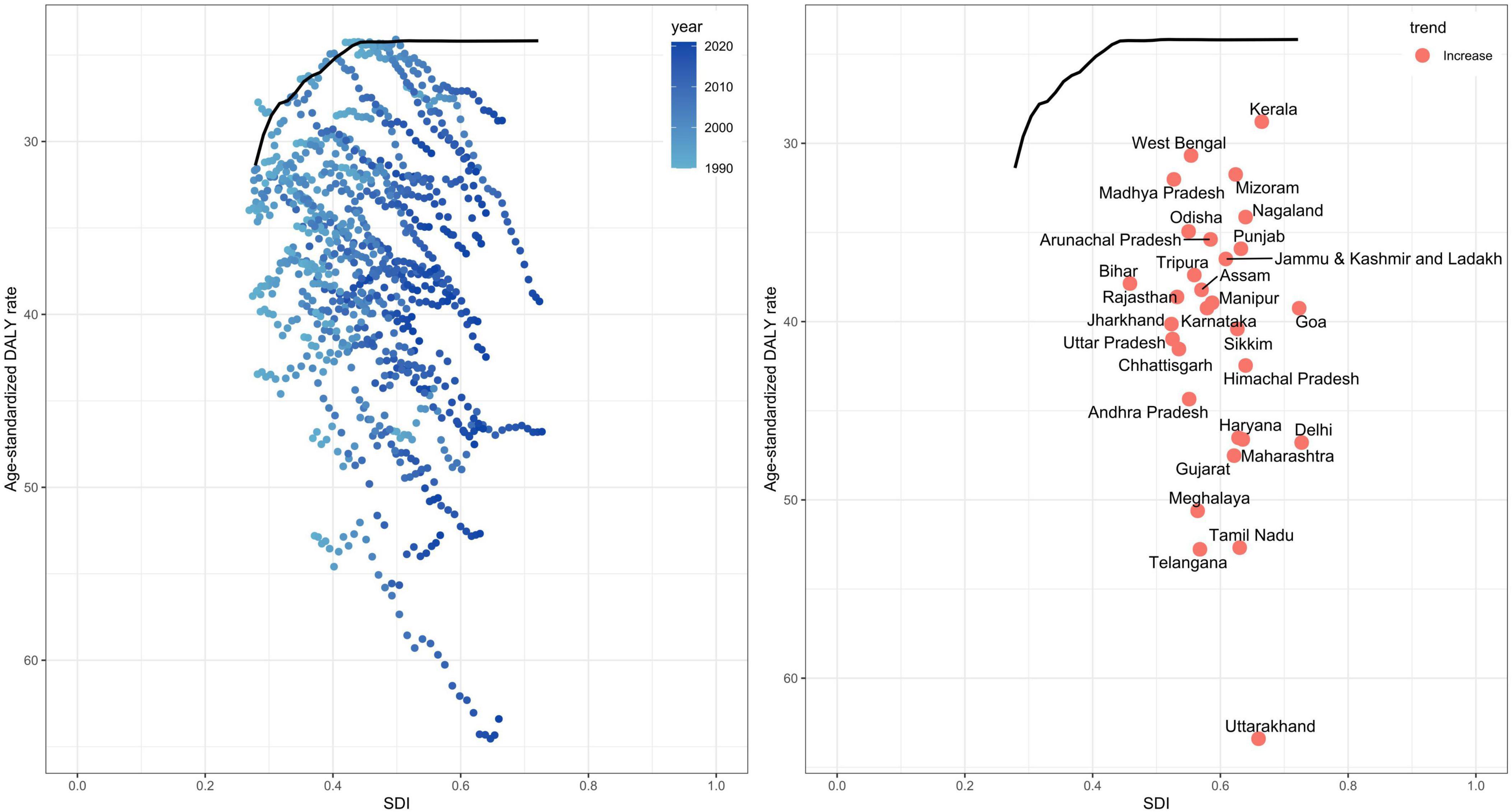
Figure 6. Relationship between age-standardized DALY rates (per 100,000 persons) of rheumatoid arthritis from 1990 to 2021 across 30 geographic regions and the SDI. DALY, disability-adjusted life years; SDI, Socio-Demographic Index.
DiscussionThis study provides a systematic overview of the burden of RA from 1990 to 2021 across India and its states. The age-standardized prevalence, incidence, and DALY rates of RA are rising across India, with a more pronounced increase from 2019 to 2021, and are predicted to continue rising over the next decade. Female rates are consistently higher and increase with age, varying across different states in India. These findings confirm that RA has become a significant public health concern in India.
Female RA incidence rates are 2.6–2.9 times higher than those in males. This gender difference may stem from multiple factors such as physiological differences, sociocultural influences, and lifestyle factors. Females may be more susceptible to autoimmune diseases due to differences in immune system functioning compared to males (18). Estrogen may play a promoting role in RA pathogenesis, while male hormone testosterone may have a protective effect (19–21). In the socio-cultural context of India, women may face greater barriers to accessing healthcare, such as unequal distribution of medical resources and prioritization of male family members’ health, which could lead to delayed diagnosis and treatment for female RA patients. This may result in higher prevalence and disease burden (22, 23). Indian women may also be more affected by certain lifestyle factors, such as a higher burden of household chores, fewer opportunities for physical activity, and potentially poor nutrition associated with poverty and low education levels (24–27).
In the analysis of the global burden of RA, the same trend was shown, namely, the proportion of women with RA was higher (28). Furthermore, in our results, we found that the prevalence of RA in India peaked at 75–79 years of age, again consistent with the results of the global RA burden, showing a clear age-specific pattern. Interestingly, however, our results show that the incidence is highest in the 65–69 age group, which may indicate that there is some delay in the diagnosis of RA in India, or that early diagnosis and treatment of RA need to be strengthened. In addition, the results of the global analysis show that RA is highly correlated with SDI, which also explains the differences in the prevalence of RA between Indian states. However, in some non-high-income regions, the prevalence of RA is significantly lower than in India, and whether this is related to the level of regional diagnosis and regional living standards needs further discussion and research. As for the change in prevalence, the reason for the increase in prevalence in recent years is also the change in diagnostic criteria. In 2010, the American College of Rheumatology (ACR) and the European League against Rheumatism (EULAR) jointly issued a new classification standard for RA. At the heart of the guidelines is a desire to be able to diagnose and intervene earlier in RA, whereas previous criteria were more inclined to diagnose “confirmed RA.” Therefore, the prevalence may increase (29).
The prevalence of RA varies considerably across different geographical unit in India, with regions like Uttarakhand and Tamil Nadu showing significantly higher prevalence rates compared to states like Goa and Madhya Pradesh. These disparities can be partially attributed to differences in the SDI and environmental factors. Environmental factors such as climate, dietary habits, and levels of pollution exposure in different regions may also influence the incidence of RA (30, 31). For instance, the cold and damp climates in certain areas may exacerbate RA symptoms, while regions with higher levels of industrialization might face increased pollution exposure, contributing to higher RA incidence. In regions with higher SDI, RA may be diagnosed more frequently, which does not necessarily indicate a lighter RA burden in low SDI regions. On the contrary, the actual burden in these areas might be underestimated due to inadequate diagnosis and treatment. It is noteworthy that Kerala, despite having a higher SDI, has the lowest disease burden, largely due to its efficient public health system and high-quality medical services. Kerala’s public health system is widely accessible, with well-developed primary healthcare facilities and a relatively equitable distribution of medical resources (32–34). This is a model worth emulating in regions like Uttarakhand. The economic gap leads to disparities in medical-related services among different regions. For instance, the economy can directly affect the development of hospitals and medical technologies in a region, thereby influencing the diagnosis and active treatment of RA. Moreover, the economy also impacts the educational level of a region. Regions with a higher educational level are more helpful in self-protection and early diagnosis of RA compared to those with a lower educational level (35, 36).
Given the increasing burden of RA in India and the pronounced differences across gender and regions, public health strategies should focus on the following areas: (1). Enhancing Identification and Treatment of RA Among Women: The identification and treatment of RA in women should be a priority, especially in rural and low-SDI regions where healthcare resources are limited. This can be achieved through the enhanced training of healthcare professionals and by raising public awareness about RA (37, 38). (2). Regional Health Planning: Due to the significant variation in RA burden across different regions, health policies need to be more flexible and adapted to the specific circumstances of each state. For instance, regions with a high burden, such as Uttarakhand and Delhi, require more intensive prevention and management strategies (13). (3). Promoting Early Diagnosis and Intervention: Early diagnosis and intervention are crucial in reducing the long-term burden of RA. The government should consider expanding RA screening programs, particularly among high-risk groups such as women and the elderly, and improving patients’ self-management capabilities (13, 39). (4). Research and Data Collection: Although substantial progress has been made, further support is necessary for epidemiological research on RA in India. This research is essential to better understand the specific factors contributing to gender and regional disparities. Increased research efforts will aid in developing more targeted interventions.
Our study still has some limitations, for example, data may be scarce for some states, so differences between different Indian states need to be explained more rigorously. In addition, our research data comes from 1990 to 2021, and our calculation and prediction are all based on this period. For future prediction, more recent data or updated data may be required to calculate more accurately.
ConclusionThis study, based on GBD 2021 data, reveals a growing burden of RA in India from 1990 to 2021, with the trend expected to continue. Notably, the burden is higher among females, and there are considerable regional differences in prevalence. These findings suggest that enhanced early diagnosis and treatment, especially in females and high-burden regions, are critical to reducing the disease’s impact. Efforts should focus on improving healthcare accessibility and providing targeted interventions to reduce the overall burden of RA in India.
Data availability statementPublicly available datasets were analyzed in this study. This data can be obtained from the IHME website at https://vizhub.healthdata.org/gbd-results/.
Ethics statementEthical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributionsWS: Data curation, Writing – original draft. XL: Visualization, Writing – original draft. HZ: Writing – review and editing. HL: Writing – review and editing.
FundingThe authors declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by funding from the Natural Science Foundation of Tianjin (No. 23JCYBJC00700) and the Tianjin municipal health and Health Committee (No. TJWJ2024QN046).
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statementThe authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AbbreviationsGBD, Global Burden of Disease; RA, rheumatoid arthritis; DALY, disability-adjusted life years; SDI, Socio-Demographic Index; IHME, Institute for Health Metrics and Evaluation; ICD, classification of diseases; YLDs, years lived with disability; YLLs, years of life lost; ACR, American College of Rheumatology; EULAR, European League against Rheumatism.
Footnotes References1. Di Matteo A, Bathon J, Emery P. Rheumatoid arthritis. Lancet. (2023) 402:2019–33.
2. Gravallese E, Firestein G, Koscal N, Ling E, Longo D, Messenger L, et al. What is rheumatoid arthritis? N Engl J Med. (2024) 390:e32.
3. Scherer H, Haupl T, Burmester G. The etiology of rheumatoid arthritis. J Autoimmun. (2020) 110:102400.
4. Alam J, Jantan I, Bukhari S. Rheumatoid arthritis: Recent advances on its etiology, role of cytokines and pharmacotherapy. Biomed Pharmacother. (2017) 92:615–33.
6. Roodenrijs N, van der Goes M, Welsing P, Tekstra J, Lafeber F, Jacobs J, et al. Difficult-to-treat rheumatoid arthritis: Contributing factors and burden of disease. Rheumatology (Oxford). (2021) 60:3778–88.
7. Cross M, Smith E, Hoy D, Carmona L, Wolfe F, Vos T, et al. The global burden of rheumatoid arthritis: Estimates from the global burden of disease 2010 study. Ann Rheum Dis. (2014) 73:1316–22.
8. Vergne-Salle P, Pouplin S, Trouvin A, Bera-Louville A, Soubrier M, Richez C, et al. The burden of pain in rheumatoid arthritis: Impact of disease activity and psychological factors. Eur J Pain. (2020) 24:1979–89.
9. Singh G, Mahajan N, Abrol S, Raina A. Anxiety and depression are common in rheumatoid arthritis and correlate with poor quality of life in Indian patients. Reumatologia. (2021) 59:386–93. doi: 10.5114/reum.2021.112351
PubMed Abstract | Crossref Full Text | Google Scholar
10. Bagepally B, Kumar S, Sasidharan A, Haridoss M, Venkataraman K. Household catastrophic health expenditures for rheumatoid arthritis: A single centre study from South India. Sci Rep. (2023) 13:15385. doi: 10.1038/s41598-023-42623-y
PubMed Abstract | Crossref Full Text | Google Scholar
11. Almutairi K, Nossent J, Preen D, Keen H, Inderjeeth C. The prevalence of rheumatoid arthritis: A systematic review of population-based studies. J Rheumatol. (2021) 48:669–76.
12. Finckh A, Gilbert B, Hodkinson B, Bae S, Thomas R, Deane K, et al. Global epidemiology of rheumatoid arthritis. Nat Rev Rheumatol. (2022) 18:591–602.
13. Handa R, Rao U, Lewis J, Rambhad G, Shiff S, Ghia C. Literature review of rheumatoid arthritis in India. Int J Rheum Dis. (2016) 19:440–51.
14. Murray C, GBD 2021 Collaborators. Findings from the Global Burden of Disease study 2021. Lancet. (2024) 403:2259–62.
15. GBD 2019 Demographics Collaborators. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950-2019: A comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396:1160–203. doi: 10.1016/S0140-6736(20)30977-6
PubMed Abstract | Crossref Full Text | Google Scholar
16. GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396:1223–49.
17. Zhang M, Li M, Hu H, Li X, Tian M. Global, regional, and national burdens of rheumatoid arthritis in young adults from 1990 to 2019. Arch Med Sci. (2024) 20:1153–62. doi: 10.5114/aoms/183955
PubMed Abstract | Crossref Full Text | Google Scholar
18. Sciarra F, Campolo F, Franceschini E, Carlomagno F, Venneri M. Gender-specific impact of sex hormones on the immune system. Int J Mol Sci. (2023) 24:6302.
20. Gupta P, Sheoran A, Gupta P, Mahto S, Jain P, Varshney A, et al. Association of sex hormones and androgens with disease activity in premenopausal females with rheumatoid Arthritis. Mediterr J Rheumatol. (2023) 34:152–8.
21. Cutolo M, Villaggio B, Craviotto C, Pizzorni C, Seriolo B, Sulli A. Sex hormones and rheumatoid arthritis. Autoimmun Rev. (2002) 1:284–9.
22. Sharma I, Pandit B, Pathak A, Sharma R. Hinduism, marriage and mental illness. Indian J Psychiatry. (2013) 55:S243–9.
24. Muhammad T, Pai M, Kumar M, Sekher T. Multiple socioeconomic risks and cognitive impairment among older men and women in India. Dialogues Health. (2023) 2:100119.
25. Jain U, Angrisani M, Langa K, Sekher T, Lee J. How much of the female disadvantage in late-life cognition in India can be explained by education and gender inequality. Sci Rep. (2022) 12(1):5684. doi: 10.1038/s41598-022-09641-8
PubMed Abstract | Crossref Full Text | Google Scholar
26. Reed M. The labor force participation of Indian women before and after widowhood. Demogr Res. (2020) 43:673–706.
27. Kiss P, Depypere H, De Meester M, Vingerhoets I, Van Hoecke M, Braeckman L. Need for recovery after work and associated risk factors in working menopausal women. Maturitas. (2024) 187:108054.
28. GBD 2021 Rheumatoid Arthritis Collaborators. Global, regional, and national burden of rheumatoid arthritis, 1990-2020, and projections to 2050: A systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. (2023) 5:e594–610.
29. Aletaha D, Neogi T, Silman A, Funovits J, Felson D, Bingham C III, et al. 2010 rheumatoid arthritis classification criteria: An American college of rheumatology/European league against rheumatism collaborative initiative. Ann Rheum Dis. (2010) 69:1580–8.
30. Zou W, Fang Y, Xu D, Zhu Y. Increasing global burden of rheumatoid arthritis: An epidemiological analysis from 1990 to 2019. Arch Med Sci. (2023) 19:1037–48.
31. Guan S, Zheng J, Sam N, Xu S, Shuai Z, Pan F. Global burden and risk factors of musculoskeletal disorders among adolescents and young adults in 204 countries and territories, 1990-2019. Autoimmun Rev. (2023) 22:103361. doi: 10.1016/j.autrev.2023.103361
PubMed Abstract | Crossref Full Text | Google Scholar
32. Sathyan A. Balancing health-care privatization in Kerala: The imperative of public sector intervention. Indian J Public Health. (2024) 68:128–9. doi: 10.4103/ijph.ijph_1284_23
PubMed Abstract | Crossref Full Text | Google Scholar
33. Joseph S. Impact assessment of accreditation in primary and secondary public health-care institutions in Kerala. India. Indian J Public Health. (2021) 65:110–5. doi: 10.4103/ijph.IJPH_827_20
PubMed Abstract | Crossref Full Text | Google Scholar
34. Krishnan A, Varma R, Kamala R, Anju R, Vijayakumar K, Sadanandan R, et al. Re-engineering primary healthcare in Kerala. Public Health Action. (2023) 13:19–25. doi: 10.5588/pha.22.0033
PubMed Abstract | Crossref Full Text | Google Scholar
35. Jain Y, Govindasamy H, Kaur G, Ajith N, Ramasamy K, Ramachandran P. Microplastic pollution in high-altitude Nainital lake, Uttarakhand, India. Environ Pollut. (2024) 346:123598. doi: 10.1016/j.envpol.2024.123598
PubMed Abstract | Crossref Full Text | Google Scholar
36. Kala P, Thapliyal N, Pandey H, Piyush A, Maheshwari S, Chaudhary V. Medical students’ perspective on online teaching during pandemic: Experience from a Government Medical College in Uttarakhand. India. J Educ Health Promot. (2021) 10:473. doi: 10.4103/jehp.jehp_113_21
PubMed Abstract | Crossref Full Text | Google Scholar
37. Shankar S, Handa R, Aneja R, Marwaha V, Ammini A, Aprajita V. Bone mineral density in Indian women with rheumatoid arthritis. Rheumatol Int. (2009) 29:377–81.
38. Pati S, Sahoo K, Samal M, Jena S, Mahapatra P, Sutar D, et al. Care-seeking pathways, care challenges, and coping experiences of rural women living with rheumatoid arthritis in Odisha, India. Prim Health Care Res Dev. (2019) 20:e83. doi: 10.1017/S146342361900032X
PubMed Abstract | Crossref Full Text | Google Scholar
39. Malaviya A, Kapoor S, Singh R, Kumar A, Pande I. Prevalence of rheumatoid arthritis in the adult Indian population. Rheumatol Int. (1993) 13:131–4.
留言 (0)