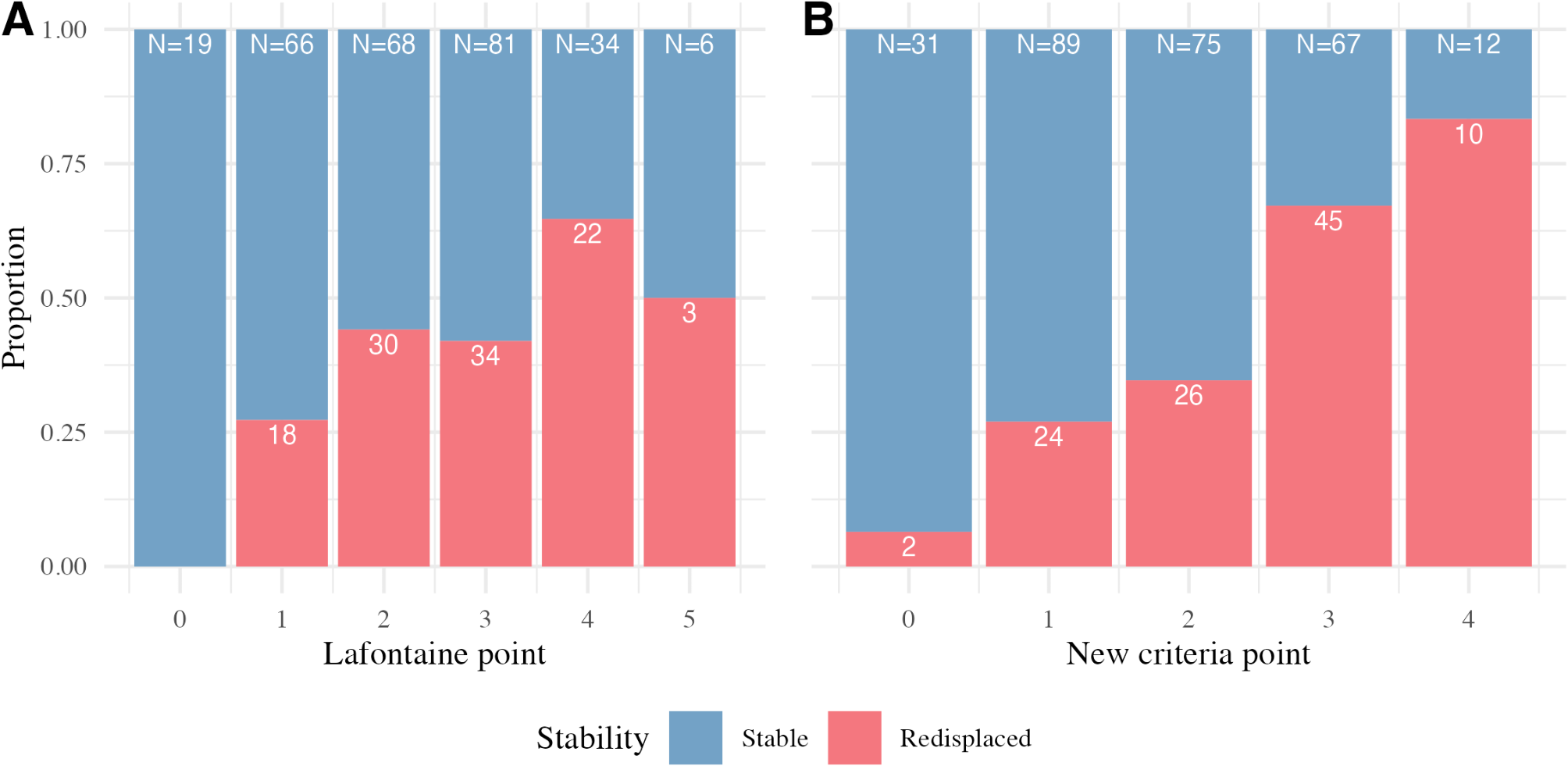
The Lafontaine criteria did not achieve the acceptable AUROC threshold of 0.7 in predicting fracture instability in our study. Of the original five predictors, age and associated ulnar fracture remained significant predictors, while initial dorsal angulation > 20° and intra-articular fractures were not associated with redisplacement. Dorsal comminution, though strongly associated with instability, had poor inter-rater reliability, limiting its clinical utility.
Lafontaine et al. [4] established that fractures with three or more instability factors were at a high risk of secondary displacement, and they recommended closed follow-up radiographic evaluation or surgical treatment for such fractures. While not originally intended as a diagnostic tool, Walenkamp et al. [3] found the Lafontaine criteria to be the most commonly used evidence-based definitions of unstable radius fractures in publications. Although immediate surgery for unstable fractures is desirable to promote early recovery, using the Lafontaine criteria to define instability could lead to overtreatment with operative fixation, potentially resulting in more complications, especially in the era of volar-locking anatomical plates [22, 23]. Therefore, a new clinical prediction tool is required to accurately define unstable radius fractures.
In addition to the Lafontaine criteria, we assessed new radiographic parameters, including the volar hook, ERLF angle, and MCR. Batra et al. [9] reported that an ERLF angle > 25°, indicative of radiocarpal malalignment, was highly associated with early and late fracture redisplacement. Rhee and Kim introduced the MCR as a measure of dorsal metaphyseal comminution, finding it significantly predictive of instability with excellent inter-rater reliability based on two raters [10]. LaMartina et al. [5] identified the volar hook as a strong predictor of final volar angulation and loss of volar angulation, while Mathews et al. [24] associated poor volar cortex reduction with redisplacement and malunion at 6 weeks.
In this study, the inter-rater reliability for the ERLF angle and MCR was below an acceptable threshold, limiting their reproducibility as predictors of fracture instability. The poor reliability of the ERLF angle in our study aligns with the findings of Garcia-Elias et al. [25], who reported limited reproducibility of radiolunate angle measurements, with a standard deviation of 5.2° among seven examiners. For the MCR, conflicting evidence exists. Rhee and Kim [10] reported excellent inter-rater reliability (ICC 0.812, 95% CI 0.721–0.886); however, their results were based on measurements by the two raters who developed the method, whereas our study evaluated the ICC among four raters who were potential users of the method. We found that measuring the width of the metaphyseal void on post-reduction radiographs was challenging, as reduced contrast and cast interference significantly decreased measurement reliability [26]. These factors potentially render the ERLF angle and MCR measurements unreliable.
The volar hook, or the restoration of volar cortical continuity in post-reduction radiographs, demonstrated favourable inter-rater reliability and was significantly associated with fracture instability in univariable analysis. However, its predictive value diminished when adjusted for other predictors, such as initial radial shortening, initial radial inclination, and dorsal comminution. Notably, Mathews et al. found that the volar hook was correlated with fracture redisplacement in univariable analysis; however, they did not perform multivariable analysis [24]. In contrast, our study conducted multivariable analysis and found that while the volar hook had significant predictive value in the univariable analysis, it was not significant after adjusting for other factors.
The updated criteria developed in this study included four predictors: age 56–74 years (1 point), age > 74 years (2 points), associated ulnar fracture (1 point), and initial radial shortening > 3 mm (1 point), with a score of two or more indicating instability. While associated ulnar fracture and age were part of the original Lafontaine criteria, we revised the age threshold from > 60 years into two categories based on population quartiles, allowing for better risk stratification without becoming overly complex. The addition of initial radial shortening, an established predictor of fracture instability, further highlights the relevance of initial displacement as a predictor of fracture redisplacement [27,28,29]. The updated criteria exceeded our target AUROC of 0.7, reflecting an improvement over the original Lafontaine criteria. However, the improvement was marginal and less substantial than anticipated, suggesting that the relationships among radiographic parameters may be too complex to be fully captured by traditional logistic regression models. Another consideration would be to include additional predictors from early follow-up x-rays, such as marginal secondary displacement at 1–2 weeks, which Schmidt et al. [30] found to be highly associated with malunion at 3 months. While this approach could lead to a longer wait time before making surgical decisions, it may significantly improve the discriminative ability of the criteria. Unfortunately, we do not routinely perform follow-up x-rays in the first week and therefore could not evaluate this predictor.
We applied stricter criteria for post-reduction alignment, specifically excluding fractures with dorsal angulation > 0°, to reduce the risk of redisplacement. Accepting a dorsal angulation of < 10° immediately after reduction could mean that fractures with an angulation close to 10°, such as 9°, would be considered acceptable. However, even a small collapse of 1–2° at follow-up would quickly classify these fractures as unacceptable, increasing the likelihood of redisplacement. Given the likelihood of an additional 5° of dorsal angulation in follow-up x-rays within the first week [30], our decision to use more stringent alignment criteria at the post-reduction stage is justified to better identify fractures at risk for redisplacement.
This study had several notable strengths. To our knowledge, it is the first to formally validate the performance of the Lafontaine criteria in predicting unstable distal radius fractures. Additionally, we utilised both inter-rater reliability and the strength of association to determine the suitability of the predictors for identifying unstable fractures.
However, this study had some limitations. Its retrospective nature may introduce selection bias, though the use of radiographic parameters minimizes this risk. One major limitation was the follow-up period of at least 4 weeks rather than the 6-week minimum used in some studies, which may have led to an underestimation of late redisplacement cases. Additionally, while our sample size was adequate for analysis, it was not large enough to assess complex interactions between radiographic predictors. This study was conducted at a single center, which may limit the generalizability of our findings. Moreover, we only evaluated radiological outcomes, which may not fully capture the differing functional outcomes based on a patient’s functional demands. Patients with higher functional demands, despite older chronological age, may benefit more from our criteria for acceptable alignment than those with lower functional demands [31, 32]. Future studies should validate these criteria in larger, multicenter cohorts with longer follow-up periods to enhance robustness and external validity.








留言 (0)