This study evaluated patients who were ventilated in internal medicine wards.
The main results included: a 19% rate of successful weaning from ventilation; weaned patients were mostly fully independent prior to ventilation, ventilated with low PEEP values, had high hemoglobin and albumin levels alongside low CRP and lactate levels. Moreover, those who remained ventilated tended the need of vasopressor treatment, had positive blood cultures and lower GFR levels during hospitalization. Finally, in-hospital mortality was 60%, while the 30-days mortality rate was lower in the ones who were weaned from ventilation.
As previously hypothesized, the study cohort of ventilated patients in internal medicine wards are older, with a mean age of 79 years (range 69–85) and a low rate of independence prior to admission. Lieberman et al., found that the decision to ventilate in ICUs was significantly and independently influenced by age and a pre-hospitalization functional independence measure. In that study, the percentage of ICU ventilations in the 65 to 74, 75 to 84, and 85 + age groups was 62%, 45%, and 23%, respectively [2]. We assume that as a consequence, t older patients are treated and ventilated at the departments of medicine.
About one fifth of the patients in our study were successfully weaned from the ventilator. A similar finding was described by Xiao K et al. concerning adults (age > 60) with multiple organ dysfunction syndrome [10].
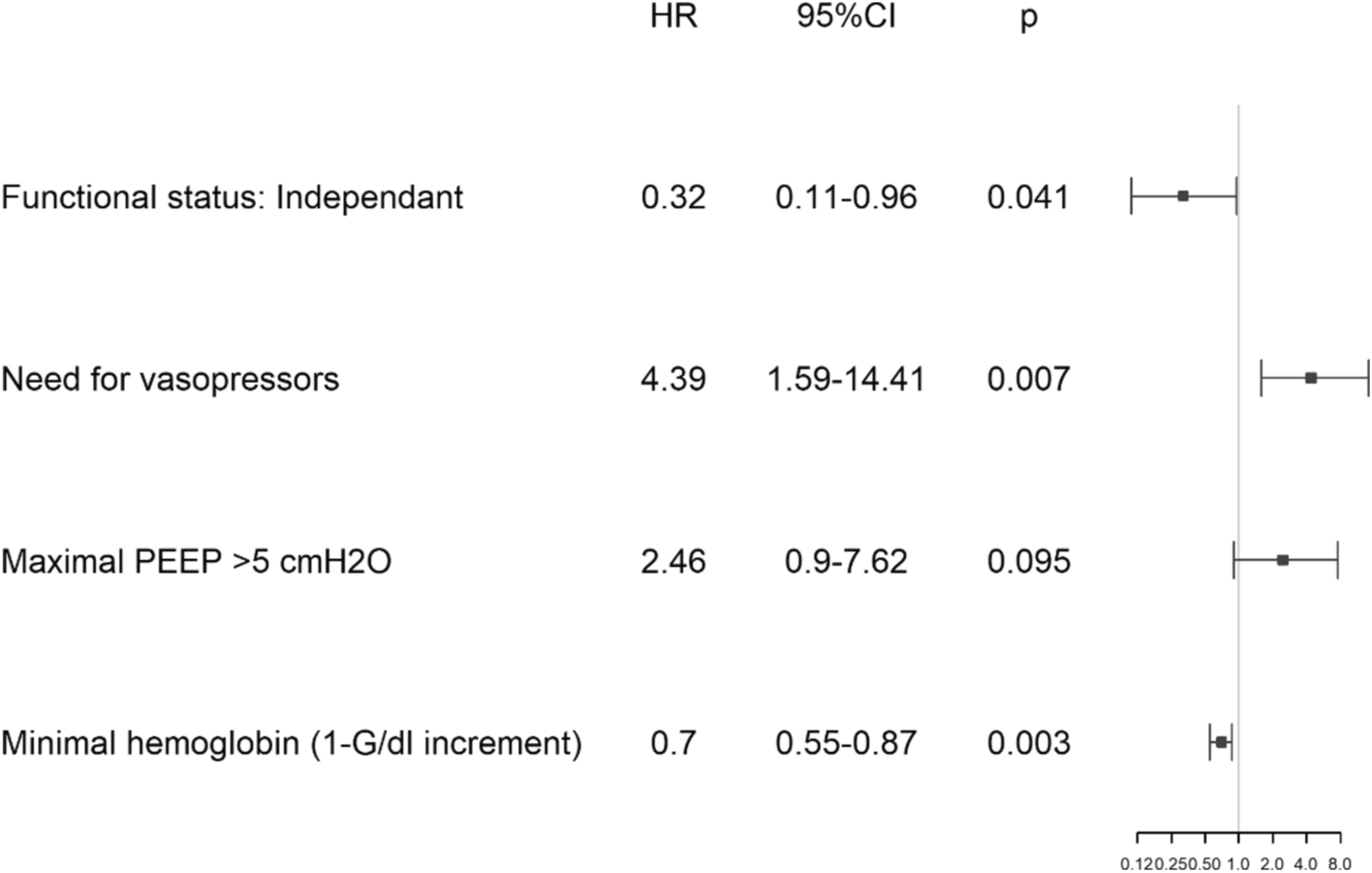
Esteban et al. concluded that survival among mechanically ventilated patients depends not only on the factors present at the start of mechanical ventilation (such as prior functional status characterized by limited activity), but also on the development of complications and patient management in the ICU, like the use of vasoactive drugs [3]. Fujii M et al. described that in ventilated adults over the age of 65 with community-acquired pneumonia, a low concentration of serum albumin, which is a marker for nutritional and inflammatory status, was associated with significant difficulty in weaning from mechanical ventilation [11]. Our study results support these findings and add several more parameters that might predict weaning from ventilation, such as higher hemoglobin and lower lactate and CRP levels. Although we found that the trough hemoglobin level during admission is a predicting factor to the ability to wean from mechanical ventilation (for every 1 g/dl increment of minimal hemoglobin level the risk of failure in weaning is reduced by 30%), low hemoglobin levels are not an absolute contraindication for weaning [5].
Another important finding was the trend towards failure in weaning in cases of high PEEP values ventilation, especially above 5 cmH2O. This might represent a severe oxygenation disorder in these patients which may pose a challenge to withdraw from mechanical ventilation.
Nearly half of our study population were hemodynamically unstable and needed vasopressors support. Despite this, the main vasopressor in use was dopamine, which is not the first-line vasopressor therapy considered for septic shock [12].
The relationship between pH and arterial blood gas tests with our study outcomes were not included in the study because of their relatively limited use in internal medicine wards and preference for venous blood sampling.
Hersch et al. reported that in-hospital survival rates (discharged alive from hospital) among ventilated patients in the internal medicine wards was 20% compared to 38% in ICU-ventilated patients [1]. In comparison, Lieberman et al. demonstrated an in-hospital mortality rate of 53.0% in ICUs compared with 68.2% in non-ICU wards, however, these results were not independently and significantly affected by hospitalization in ICUs [2]. Our study results demonstrate similar results of an approximate 60% in-hospital mortality rate amongst internal medicine patients.
Another finding of our study revealed that the length of hospitalization among patients weaned from ventilation was significantly longer than those who remained ventilated. This finding can be explained by the time necessary for recovery from ventilation due to de-conditioning in the weaned group.
This study is one of only few to have surveyed ventilated patients in internal medicine wards. This reality largely exists only in Israel and was considered one of the advantages of the Israeli medical system during the COVID-19 pandemic. Importantly, the need to ventilate patients in internal medicine departments might exist during future pandemics or in pressing situations, hence the importance of this study and its results.
There are several limitations to our study. Firstly, its retrospective design and its limited randomized selection and confounders. Second, the exact causes of admission and ventilation were not detailed, mainly because of the retrospective design and overlap causes, like: pneumonia, sepsis, acute CHF and COPD exacerbation. Furthermore, the weaning process from ventilation was not preformed according to a structured protocol and was mostly based on the clinical judgment of the treating physicians, this fact might affect the study's outcomes. Future prospective research should include a structured weaning protocol. Lastly, the use of un accepted definition of gastrointestinal bleeding (using 80 mg IV Pantoprazole) mainly because of the retrospective design and lack of data.
In conclusion, the rate of weaning from ventilation in the department of medicine is low, with higher mortality rates. Various favorable clinical parameters might predict successful weaning.








留言 (0)