In this report, we describe a rare case of solitary PJ polyp with dysplasia in the colon in which we were able to observe surface structure details. Focal high-grade dysplasia was found within the epithelium of the polyp, suggesting the need for pathological evaluation via en bloc resection of the solitary PJ polyp. To our knowledge, there are few endoscopic reports of a solitary colonic PJ polyp with high-grade dysplasia.
Solitary PJ polyps are less common in the colon. We conducted a literature search in PubMed for case reports published between 1996 and 2023. The following search terms were used: “solitary Peutz–Jeghers polyp” AND (“colon” OR “rectum”). We identified nine case reports [5,6,7, 9,10,11,12,13,14], which are summarized in Table 1. Among the nine cases, five had polyps in the sigmoid colon. The polyp was pedunculated in six cases. Moreover, in the study reported by Iwamuro et al., 39 of 51 solitary PJ polyps were found in the colorectum (21 in the sigmoid colon), and 40 cases showed a pedunculated morphology [15]. These findings characterize solitary PJ polyps as having a predilection for the sigmoid colon and a pedunculated morphology. In addition, the polyp heads were often reported to be lobulated (Table 1). A pedunculated polyp with a lobulated head may be characteristic of solitary PJ polyps; however, in this case, the head of the polyp was relatively smooth, and the stalk of the polyp was indistinct. These findings did not fit the previously reported characteristics of typical PJ polyps.
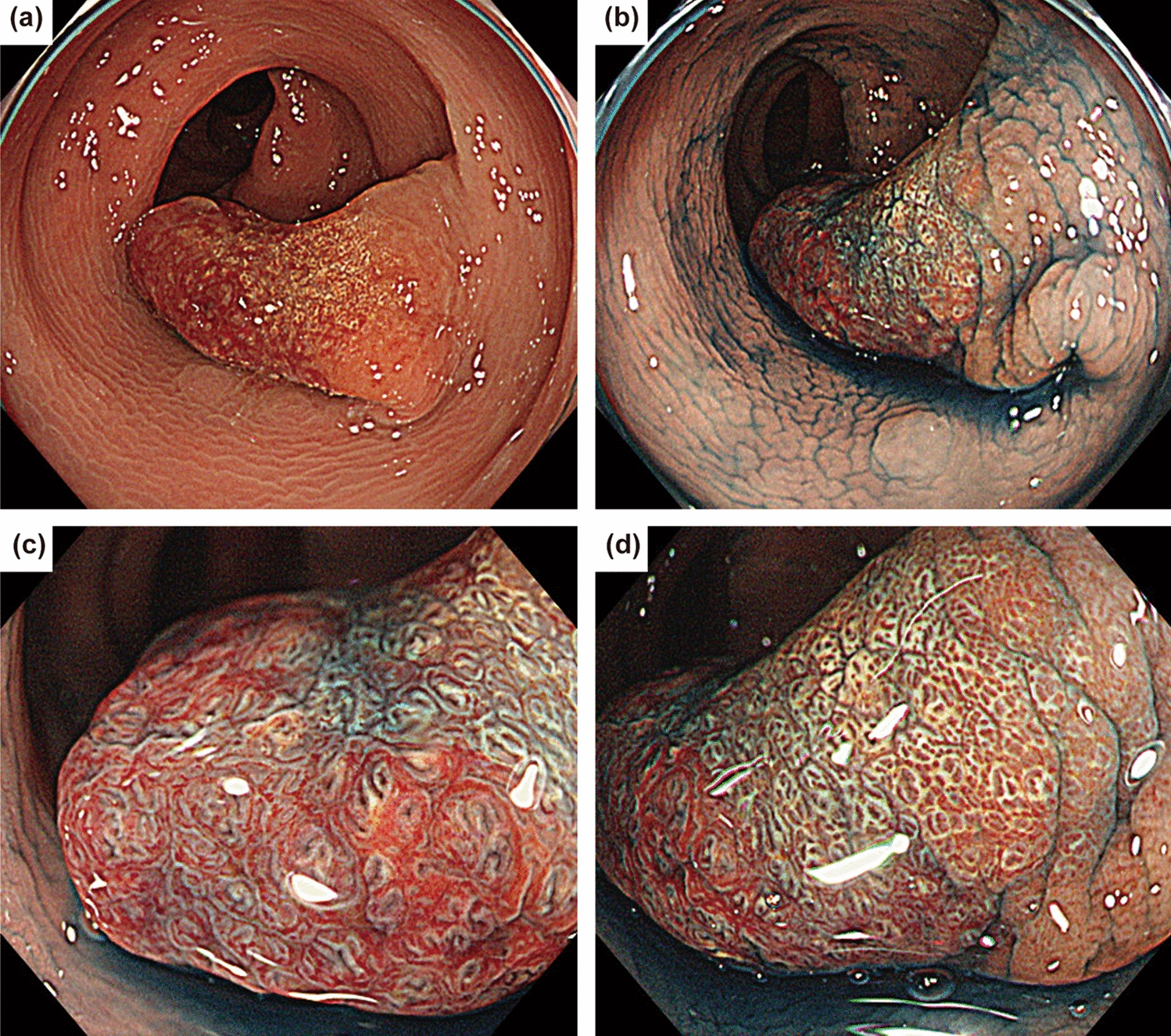
Table 1 A case study summary of solitary Peutz–Jeghers polyps in the colorectumSolitary PJ polyps are often difficult to distinguish from colorectal adenomas by endoscopy. Tsujii et al. reported large tubular or gyrus-like pit patterns on magnified endoscopic observations of solitary colonic PJ polyps [6]. In our case, the polyp had a tubular or branch-like pit pattern, and we diagnosed it as an adenoma-like lesion. However, the observed findings, such as the mixture of different surface patterns and enlargement between pits, differed from those of typical adenomas and may indicate a point of differentiation between adenomas and solitary PJ polyps. In addition, dilated glandular orifices were conspicuous when indigo carmine was sprayed, suggesting dilation of the glandular ducts due to epithelial hyperplasia of the mucosa, which is a pathological feature of PJ polyps. Further studies are needed to clarify the endoscopic features of solitary PJ polyps.
One clinical implication of this case arises because solitary PJ polyps can harbor dysplasia. Previous studies on the malignant potential of solitary PJ polyps have been controversial. Several case series have reported no recurrence after the resection of solitary PJ polyps and a low risk of cancer morbidity [15,16,17]. However, these studies also included solitary PJ polyps that developed in gastrointestinal tracts other than the colon. In contrast, in three of nine case reports of solitary PJ polyps in the colon, the polyps contained adenomas or high-grade dysplasia (Table 1). In a study investigating syndromic and sporadic PJ polyps, 7 of 87 (8.0%) sporadic PJ polyps had dysplasia, at a significantly higher rate than that observed in syndromic PJ polyps [18]. In addition, a methylome analysis showed potential features of the colorectal cancer epigenome in a solitary PJ polyp [12]. These findings suggest that solitary PJ polyps may harbor dysplastic changes and require pathological evaluation via en bloc resection. However, the incidence of invasive cancer, recurrence, and appropriate surveillance intervals for solitary PJ polyps with dysplasia have not been clearly reported and should be clarified in further case series.
In conclusion, solitary PJ polyps are rare colorectal polyps and may harbor dysplasia. Solitary colonic PJ polyps should be resected en bloc and pathologically evaluated for dysplasia.







留言 (0)