ESOS, as a malignant neoplasm, was first reported in 1941; however, few cases have been reported in contrast to skeletal osteosarcoma so far. ESOS arising from abdominal mesentery are extremely rare. To the best of our knowledge, there have been only 14 cases reported so far [13,14,15,16,17,18,19,20,21,22,23,24,25,26] (Table 1). Among them, the majority of cases arose from small bowel mesentery (10/14), 2 cases arose from sigmoid colon mesentery; besides, and only 1 case was report arising from transverse colon mesentery, besides 1 case did not clearly reported mass sites. This case we are presenting with is an ESOS arising from rectal mesentery; seemingly there has been no case reported before.
Table 1 Literature review of ESOS of the mesentery casesThe case is extremely rare, and there is no commonsense guideline. And because the preoperative diagnosis was more difficult, there were other primary malignant tumors in this case, which was a challenging point in this case.
Extraskeletal osteosarcomas (ESOS) is a kind of very rare disease. According to a literature report, the incidence of ESOS is around 1–2% of all soft tissue sarcoma [27]. Allan et al. reported the incidence of ESOS in soft tissue sarcoma is 1.94% (26/2100), while Lorentzon et al. reported that is 1.65% (4/242) [3, 4]. As reported by some groups, the age of patients with skeletal osteosarcoma is always below 30 years old; in contrast, ESOS is primarily with an older mean age of 47.5 to 61 [6, 7, 27,28,29,30,31,32]. Meanwhile, Nathalie E. J. van den Broek et al. argued that ESOS typically affected patients with an age between 50 and 70 [17]. According to a clinical features analysis by Sheila Thampi et al., the mean age for patients with ESOS is 60.7 years (range from 9 to 96; median age is 64 years) compared to 31.4 years (range from 0 to 99; median age is 20 years) for those with skeletal osteosarcoma [28]. Summarizing all above reports, regardless of the statistic details, it is a definite conclusion that patients with ESOS significantly tend to have an older age in contrast to patients with skeletal osteosarcoma. This age distribution characteristic between ESOS and skeletal osteosarcoma is also proved by the SEER database [28]. Depending on the data supported by Table 1, the mean age for patients with abdominal mesentery ESOS is 60.14 (range from 40 to 75; median age is 62 years). The patient in our case is 52-year-old female.
Gender distribution varies of ESOS in each cohort study have not a consensus. The reason for that perhaps is the low incidence of ESOS and cohort data insufficiency. Female predominance for ESOS was observed by Sheila Thampi et al., as did Choi et al. [7, 28]. However, the majority of case series described a male predominance [6, 11, 27, 29]. In some groups analysis, a ratio of males with ESOS versus females with that is 1.9:1 [17, 30]. From Table 1, we observed that, among abdominal mesentery ESOS, males are 8 cases (8/14), females are 6 cases (6/14).
According to previous literature reporting, distant metastatic disease, larger tumor size, TNM stage > 2, axial tumor site, positive margins, and older age are supposed to be adverse prognostic factors [6, 7, 27, 29]. Among these prognostic factors, distant metastatic disease at diagnosis can be confirmed to have an unfavorable prognostic impact by some studies [6, 28]. Distant metastases are the most common cause of death, which is in agreement with current literature, with lung being the most common site, followed by regional lymph nodes and liver [27, 30, 33,34,35]. Soft tissue, skin, and peritoneal metastasis have also been reported [17, 31]. Covello et al. supported the theory that skin metastasis could be a sign of widespread disease [35]. Larger tumor size is another adverse prognostic factor, which is supported by present and previous literature [23, 28, 29, 36]. It can be a definitely concluded observed by many groups that overall survival rate falls down as tumor size increases. Bane BL et al. observed all patients (6/7 patients, 85.7%) alive with no evidence of disease had tumor measuring less than 5 cm that were amenable to perform a complete surgery excision with margin negative. Whereas the overall survival rate fell down to 12.5% (2/16 patients) for tumor size greater than or equal to 5 cm [27]. A larger SEER database analysis was also able to confirm this former adverse prognostic impact of larger tumor size, with a matrix distribution of 10 cm, by using Kaplan–Meier (KM) methods with 95% confidence intervals and log-rank tests and the Fine-Gray proportional subhazard model [28]. Ahmad et al. observed that there was a significant survival decrease for tumor size > 10 cm through an univariate analysis; however, no such decrease remained in multivariate analysis [29]. This result anticipates that tumor size or volume is one of the main adverse prognostic factors but not the only one. Some other adverse factors may also occupy their positions to a certain extent.
ESOS is categorized into three main pathological subtypes depending on different matrix components: osteoblastic, chondroblastic, and fibroblastic [35]. Telangiectasis, small cell, and mixed type are another three pathological subtypes [27, 37]. One of the most common of these is the osteoblastic variant, and the typing in our individual case was of the same type. There have been several inconsistent cohort studies on the prognostic significance of the different pathologic subtypes. Chung EB et al. observed patients with ESOS with fibroblastic components fared better than the rest [11]. Whereas Lee JY et al. observed patients with the subtype of chondroblastic survived longer than those with osteoblastic subtype by an univariate analysis [30]. However, some clinical studies did not find the prognostic difference among these three main subtypes [27, 33]. Therefore, it seems that to understand the ESOS prognostic factors will likely require a greater understanding of the cell of origin of ESOS. In the presented case, the patient was a patient suffering from gynecologic cancer with postoperative recurrence. Predicting her prognosis remains a challenging task.
Given the rare incidence of ESOS, varied clinical characters, and differing treatment approaches among groups, there is little evidence regarding standardized protocols for ESOS. Based on data from the literature, current treatment options are based on wide resection, followed by postoperative adjuvant radiotherapy and chemotherapy [38]. According to the study, expanding the surgical scope reduces the local recurrence rate but has no significant effect on prolonging survival time [30]. Although multimodal therapy approaches were applied, including surgical resection, chemotherapy, and radiotherapy, previous literature reported dismal overall survival for patients with ESOS [7, 11, 27, 29,30,31,32,33]. According to the reports, 3-year overall survival of ESOS is approximately 61%, and 5-year overall survival is only 25% [7, 39]. However, complete surgical resection and negative surgical margin so far have been anticipated to be crucial effective treatments that have already performed comprehensively in carcinoma and osteosarcoma, though there is no adequate reliable data and a lack of multi-center cohort analysis trials on these two yet. Goldstein-Jackson et al. found that complete surgical resection was the only statistically significant prognostic factor for a better overall survival result in their univariate analysis [31]. Although a complete surgical remission is performed by most studies, local recurrences and even distant metastasis are still obstacles, which are the main unfavorable impacts on overall survival. As previous literature reported, the local recurrent rate is approximately 20%–69% [29,30,31, 33, 40]. In this individual case, a total mesorectal resection technique was used, and postoperative pathology suggested that no lesions were seen at the bilateral margins and that the liver occupying the line of perforation pathology suggested non-ESOS. to some extent, it suggests that the surgery has the potential to achieve radical resection. More data are still needed to confirm this.
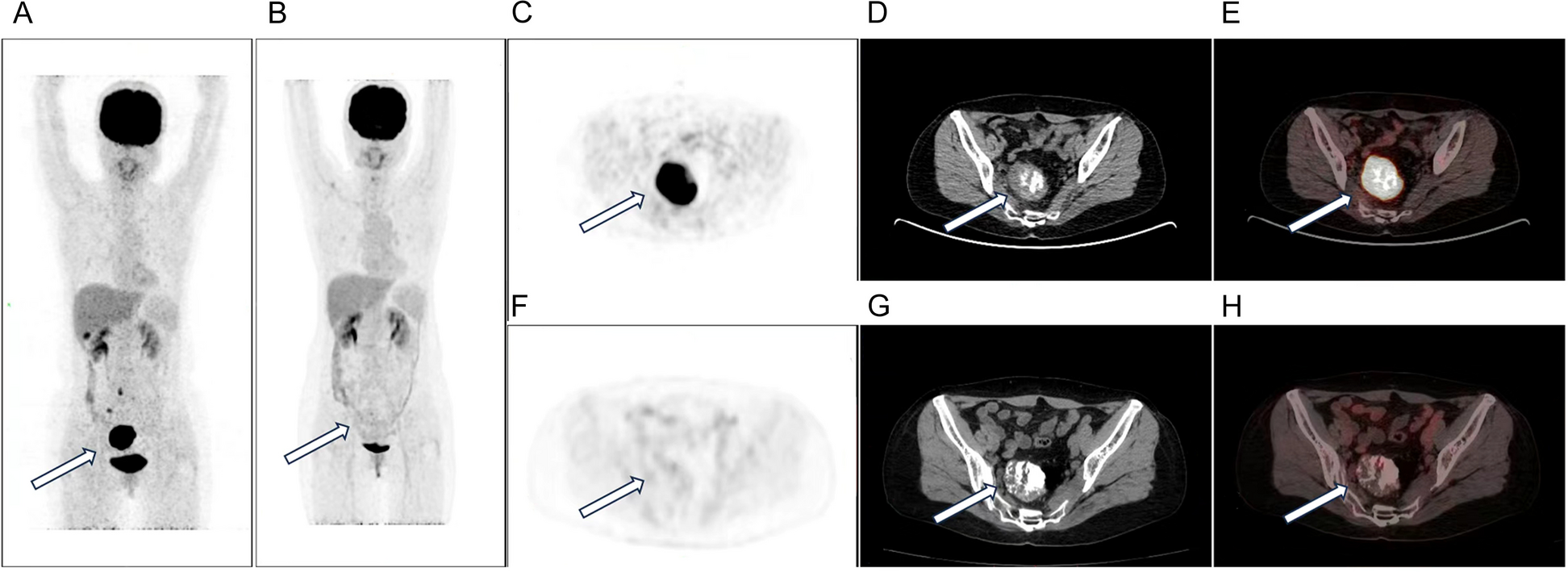
Chemotherapy remains controversial about regimens and effects [23, 29, 31]. Ahmad et al. reported they received an unsatisfied effective rate by applying doxorubicin-based regimens, while cisplatin-based chemotherapy was not active either [29]. However, S. Y. Goldstein-Jackson et al. obtained more favorable results with a more aggressive multiagent chemotherapy strategy [31]. Therefore, they recommend that patients with ESOS be treated with polychemotherapy regimens including doxorubicin, ifosfamide, cisplatin, and possibly methotrexate and adequate surgery. Wang et al. observed that there was no significant survival benefit between the group of patients with methotrexate, adriamycin, and cisplatin-based chemotherapy regimens and the group of patients with adriamycin or ifosfamide chemotherapy regimens. Even no survival difference between those who received chemotherapy and those who did not receive was found in his study [37]. In our presenting case, a multi-regimen of chemotherapy and gene-targeting drug bevacizumab were given before a thorough surgery, and a 18F-FDG-PET-CT followed, which confirmed “occupying lesion reduced slightly with a decreased glucose metabolic activity." It seemingly suggests that a proper multi-regimen may be effective for abdominal mesentery ESOS; furthermore, bevacizumab could be certified to be one of the useful medicine supplements for ESOS. The patient underwent a postoperative chemotherapy regimen of liposomal camptothecin in combination with carboplatin for recurrence of ovarian malignancy. Perhaps these drugs may also have some effect on ESOS.
Radiotherapy is a predisposing factor for the development of bone and soft-tissue sarcomas [41]. Whereas palliative radiotherapy is considered a substitute approach for the patients with ESOS who have no opportunity to complete a surgical resection, who tolerate chemotherapy, or who are in advanced stage. Radiotherapy has been reported to be beneficial in reducing the volume of tumors and local recurrence but not beneficial in increasing the overall survival rate [7, 37].
This is a rare case and the type of pathology could not be clarified preoperatively to clarify the chemotherapy regimen. When the diagnosis is difficult, MDT does have helpful implications. However, in this case, the patient was fully communicated with preoperatively and agreed that the results of intraoperative exploration would determine the subsequent treatment. When the diagnosis is difficult, there should be a sense of suspicion of ESOS. In the case of preoperative diagnostic difficulties, further examination is needed, and if necessary, puncture biopsy is performed if the site is suitable. Particular attention is paid to those with a history of ESOS.
ESOS should also be considered when imaging demonstrates an intraperitoneal solid cystic or calcified mass [38]. The imaging features of ESOS lack distinctive characteristics. The diagnosis of ESOS should be made in the context of the clinical presentation as well as imaging and pathologic findings and only after the possibility of a primary bone tumor or metastasis of a bone tumor to the soft tissues has been ruled out. Combining clinical and imaging findings, it is necessary to differentiate it from liposarcoma, gastrointestinal mesenchymal tumor, or calcified hemangioma. In conclusion, this report illustrates that ESOS originating from the rectal mesentery should be considered in the differential diagnosis of intra-abdominal malignant mesenchymal tumors. The optimal treatment of mesenteric ESOS remains a topic that requires in-depth study.



留言 (0)