
記住我


We will conduct a mixed methods systematic review to synthesis data from studies with diverse research designs. This approach will allow for a comprehensive understanding of complex issues by integrating both qualitative and quantitative evidence on digital health intervention experiences and outcomes. The review will adhere to the Joanna Biggs Institute (JBI) methodological guidance for conducting mixed methods reviews [27] and follow the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA 2020) guidelines [28] to ensure transparency, rigor, and replicability. This systematic review protocol is registered on PROSPERO (CRD 42024528122), the International Database of Prospective Register of Systematic Reviews, and is reported according to the PRISMA-P 2015 checklist [29] (see Supplementary File 1).
Eligibility criteriaA summary of the eligibility and exclusion criteria is presented in Table 1. Studies will be eligible for inclusion in the review if they meet the criteria outlined under study characteristics, populations, interventions, comparators and outcomes.
Table 1 Inclusion and exclusion criteriaStudy characteristicsThis review will include peer reviewed publications that include primary data with no geographic restriction. We will include qualitative, quantitative, and mixed method designs and exclude literature reviews, commentaries, case reports and case series, and conference and conceptual papers that do not report outcomes specific to feasibility, acceptability, and efficacy of the intervention. Studies published in English language between 1 January 2010 and 31 July 2024 will be included. This period is marked by rapid advancements in digital health and use of technology to support HIV care programs [30] and significant updates in HIV care guidelines. Since 2010, the global penetration of mobile wireless technologies, particularly smartphones with advanced computing capabilities and Internet access, has expanded rapidly with the rollout of 3G networks [31] facilitating their integration into healthcare and supporting the adoption of digital health interventions. Also, notable changes in HIV care protocols and standards, including the “test and treat” guidelines and approval of HIV self-testing [32], have redefined best practices, making it challenging to reliably compare findings from studies conducted before 2010.
PopulationStudies must include mobile populations aged 15 years and older either partially or completely. We have defined mobile populations broadly as individuals that relocate frequently or for extended periods and these include migrants, transients, immigrants, refugees, asylum seekers, mobile sex workers, and truck drivers. Migrants are sometimes defined on grounds of ethnicity or citizenship (foreigners or non-nationals). The age restriction is in line with the legal eligibility of HIV care services without a guardian/parent in most regions.
InterventionsIncluded studies must use a digital health intervention targeting one or more stages of the HIV care cascade (HIV testing, linkage to care, ART initiation, retention in care HIV treatment adherence and viral suppression). Digital health interventions include the use of digital technology, e.g., electronic health (eHealth), mobile health (mHealth), telemedicine and telehealth, either as a component or standalone strategy for delivering the intervention to mobile populations.
Comparators/controlStudies will be included regardless of whether they have a control group or not. Comparators may include standard of care or an alternative intervention.
OutcomesStudies included must report a feasibility, acceptability, or effectiveness outcome of the digital health intervention. Definitions of these outcomes vary widely in the literature, and we have considered broad definitions for this review. Feasibility can be measured by attrition, attendance, adherence, and retention in the intervention and qualitative feedback on intervention delivery [33]. Acceptability includes participant experiences and views on using digital technology such as usefulness and ease of use as well as perceptions on whether the intervention is satisfactory or agreeable [34, 35]. Efficacy is the intended effects and effect size estimations of the intervention and will include behavioral and biomedical metrics related to the HIV care cascade: (1) HIV testing uptake, (2) linkage to care, (3) ART initiation, (4) retention in care (clinic attendance, ART adherence, pill count, loss to follow up), and (5) viral suppression (viral load or other markers of treatment success including CD4 count and HIV related mortality or morbidity).
Data sourcesTo ensure comprehensive coverage of relevant literature from clinical, social, and technological perspectives, we will search PubMed, Web of Science, and EBSCOhost (Academic Search Premier, Africa-Wide information, CINAHL, Health Source: Nursing/Academic Edition, APA PsycInfo, APA PsycArticles). We will also review the bibliographies of retrieved studies for relevant citations. Using this approach will allow us to balance methodological rigor with feasibility by minimizing redundant results and maximizing the relevance and manageability of the review.
Search strategySupplementary Table 1 details a pilot search strategy for one of the databases (Web of Science) developed and tested after consultations with a digital health specialist (BM) and librarian (PM). Medical subject heading terms (MeSH) will be used where appropriate, and the primary search strategy will be modified to meet the specific syntax in each database.
Study selectionFollowing the search, all identified records will be downloaded to Endnote 20 (Clarivate Analytics) to manage citations and remove duplicates. The deduplicated list of citations will then be imported to Rayyan software [36] for screening. Screening will be conducted in two stages. The first stage will be done on Rayyan where two reviewers will independently screen the titles and abstracts against the predefined inclusion criteria. Studies that meet all criteria will be included in the second stage where full texts will be retrieved for more comprehensive review. These full texts will also be independently assessed by the two reviewers to confirm eligibility for inclusion in the final review. Reasons for exclusion of full texts that do not meet the inclusion criteria will be recorded and reported in the final review. To ensure consistency and rigor, any disagreements regarding study eligibility will be resolved through discussions between the reviewers. If consensus cannot be reached, a third reviewer (senior author) will be consulted to make a final determination. The results of the search will be presented in a PRISMA flow diagram to show the stages of identification, screening, eligibility and inclusion.
Data extractionTwo reviewers will independently extract data from studies included in the final review using a structured Microsoft excel form that will capture key details about each study as presented in Table 2. For quantitative studies, outcome data comprise of descriptive and/or inferential statistical results, while for qualitative studies, data comprise of themes or sub-themes.
Table 2 Summary of data that will be extracted to Microsoft excel formAssessment of methodological qualityStudies included in the final review will be assessed for methodological quality by two independent reviewers using the JBI critical appraisal instruments [37] (Supplementary File 2). JBI has appraisal checklists tailored to each study design and each checklist contains specific domains that assess quality, such as clarity of research questions, appropriateness of study design, recruitment strategy, data collection methods, reliability and validity of outcome measures, confounding factors, and adequacy of statistical or thematic analyses. Included studies will be scored on each domain to determine whether they meet the criterion or not and categorized into low, medium, and high quality. Any incongruities in appraisal that arise between reviewers will be discussed and resolved with the senior author. Regardless of the methodological quality, all included studies will undergo extraction and synthesis.
Data synthesis and analysisData synthesis and analysis will follow the convergent segregated approach based on the JBI methodology for mixed methods systematic reviews [27]. This method involves synthesizing qualitative and quantitative findings separately before integrating them to provide an enriched understanding of digital health interventions’ feasibility, acceptability, and efficacy in the context of HIV care for mobile populations.
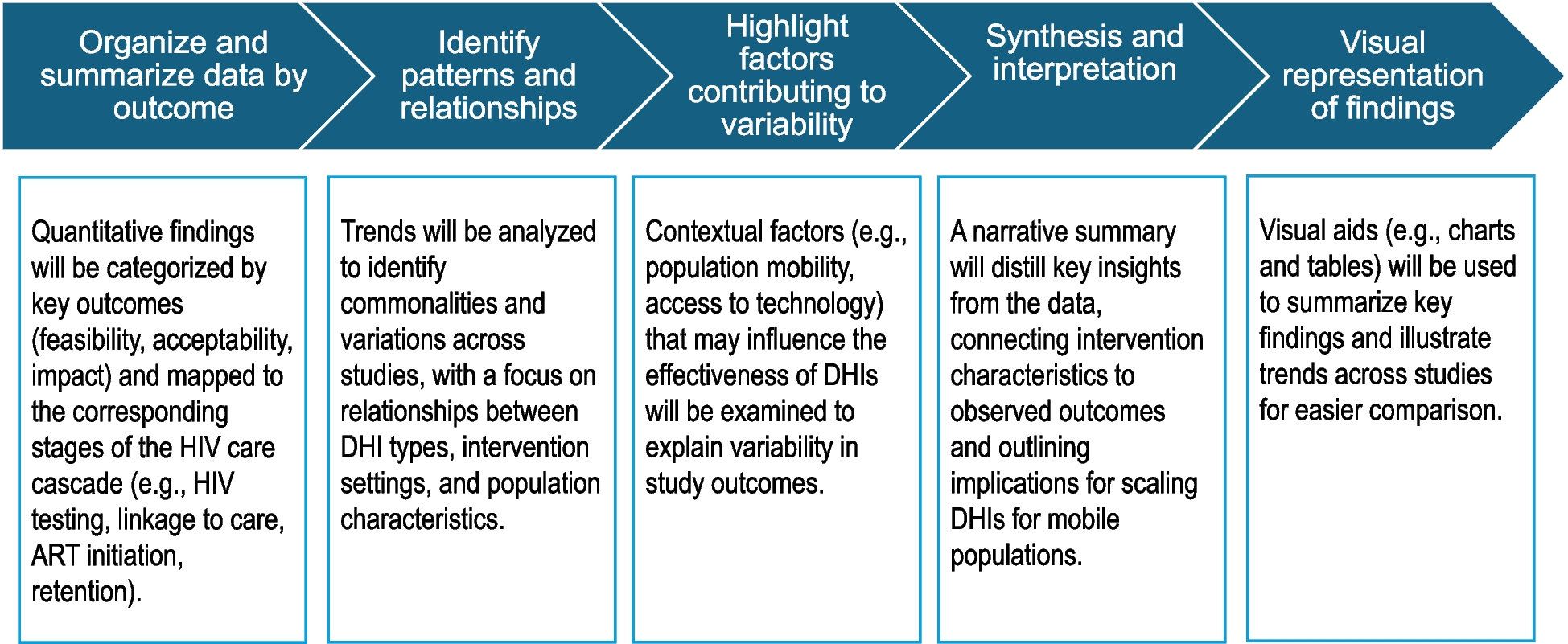
Quantitative dataBased on our initial preliminary searches, we anticipate significant heterogeneity in the study design, population characteristics, and intervention types across included studies. This variability may limit the feasibility of conducting a meta-analysis. If meta-analysis is not possible, we will conduct a narrative synthesis to systematically analyze and present the quantitative data. We will organize the data by outcome and provide a structured summary to capture and convey insights of the feasibility, acceptability, and impact of digital interventions across different stages of the HIV care cascade. The narrative synthesis will follow the steps outlined in Fig. 1.
Fig. 1
Narrative synthesis steps fir the quantitative data
If sufficient studies with comparable outcome measures are identified, a meta-analysis will be conducted to assess the feasibility, acceptability, and effectiveness of digital health intervention at each stage of the HIV care cascade (e.g., testing, linkage to care, treatment initiation, retention, and adherence). The meta-analytic approach will follow the steps presented in Table 3.
Table 3 Steps of the meta-analysis approachQualitative dataWe will categorize qualitative data into broad themes related to feasibility, acceptability, and factors influencing the implementation of digital health interventions, such as common barriers and facilitators. These themes will be further divided into sub-categories based on emerging patterns. For example, within the theme of acceptability, sub-categories might include “ease of use,” while “network stability” could emerge under feasibility. The qualitative data will then be pooled through the process of meta-aggregation [38], which involves grouping the findings into overarching themes that capture common patterns related to feasibility, acceptability, and impact. These findings will be summarized into key statements that represent collective insights across studies (e.g., privacy concerns). If meta-aggregation is not feasible, a narrative synthesis will be employed to summarize individual studies’ thematic findings, focusing on feasibility, acceptability, and implementation challenges such as barriers, facilitators, and user experiences with digital health interventions.
Mixed methods studiesThe quantitative and qualitative components will be synthesized separately as listed above for quantitative and qualitative components.
Integrating quantitative and qualitative dataOnce the quantitative and qualitative data are synthesized, they will be integrated based on their thematic similarities to produce a set of integrated findings. These findings will be presented in the form of action statements that align with the review questions [27]. The integration process will involve juxtaposing the quantitative and qualitative findings in a matrix:
One side of the matrix will contain findings from the qualitative synthesis (e.g., intervention components linked to acceptability or feasibility)
The other side will present findings on intervention effects (e.g., whether the intervention improved outcomes, had no effect).
The matrix will allow us to identify patterns and correlations, using qualitative data to explain variations observed in quantitative study findings.
留言 (0)