The authors seem to ignore the crucial difference between gender incongruence and other types of common referrals at hospitals, such as temporary illness or illnesses that are not strongly linked to social acceptance. While initiating with a good reasoning of population adjustment, the authors fail to consider that the selected data points are in essence not independent. The latter issue limits the validity of regression models without random effects. In other words, generations, which are exposed to different societal views and experiences [2], are mixed up in the analyses.
Moreover, the start of data records corresponds to the time NCGI started offering treatments, making it reasonable to expect a “burn-in” bias effect.
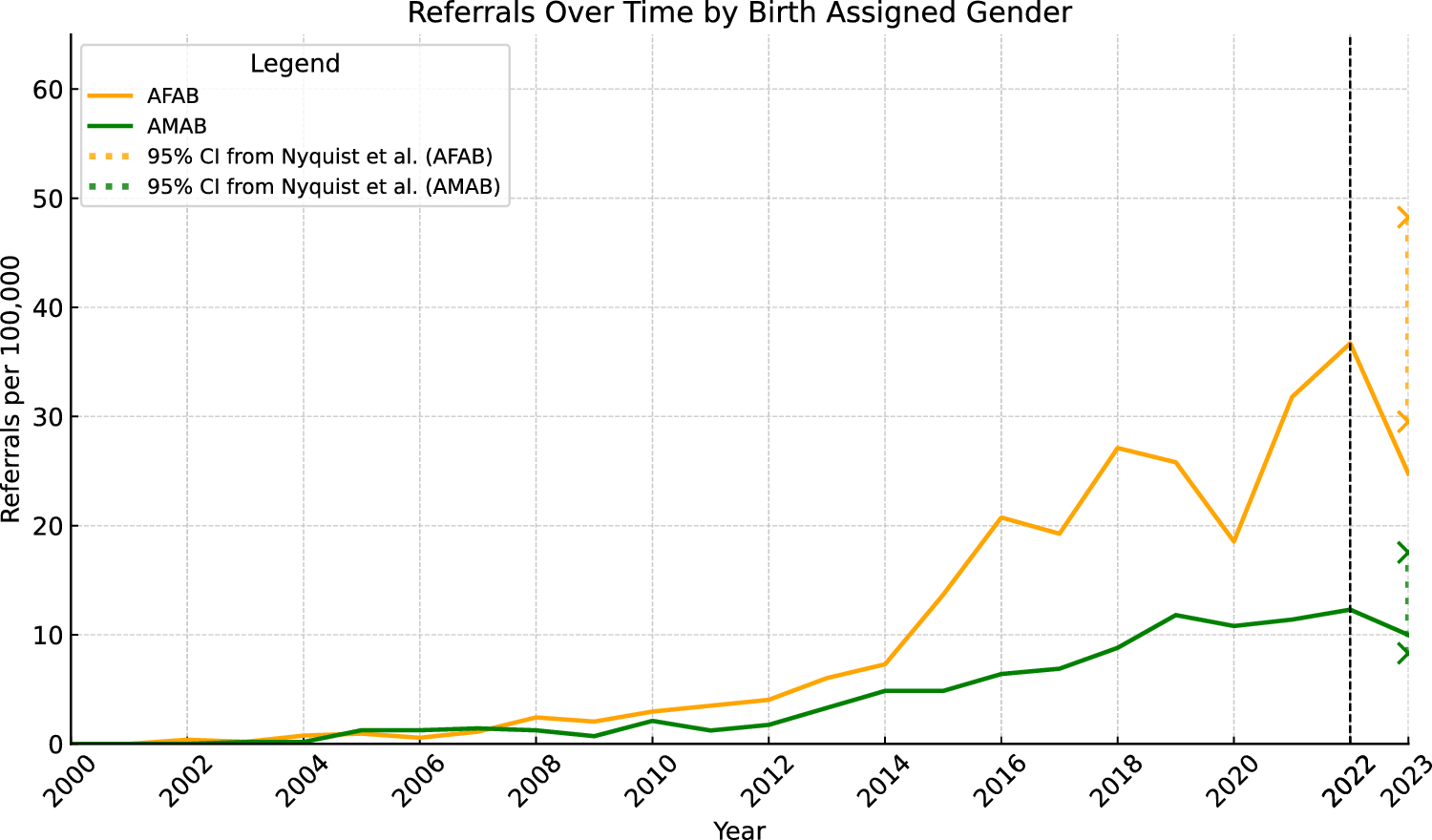
Further, increased acceptance induces a delayed effect. Therefore, the data span 2000–2022 with the corresponding burn-in effect is severely limited.
Additionally, contrasting the presented data to demographic trends of trans-population prevalence is crucial. For instance, a study conducted by Statistics Norway, [3] found that the transgender population in Norway aged \(>18\) lies around \(0.4\%\), peaking among the younger generations (\(0.7\%\)). Moreover, \(1.5\%\) of respondents claimed that their legal gender did not match their own experienced gender. Similar proportions can reasonably be expected in youth. Other studies around the world (e.g., [4] for Swedish population) place these percentages between 0.1 to 2.7% depending on the country and political situation. The peak in referrals in the article lies around \(0.04\%\), far below the lower bound of the mentioned population estimates. Following, increased healthcare seeking behaviours should be promoted as positive and not described as “dramatic” as in the article’s reference [11].
Finally, a global trend of increased utilisation of healthcare services has already been described 25 years ago [5]. Such trend, also more recently observed (e.g., USA [6]), suggests that the in-person frequency of healthcare-utilisation might not be stable in the general Norwegian population over the recent decades. Not correcting for this potential per-capita increase in healthcare-utilisation via all-cause-referrals limits the validity of the findings.
All these data features are ignored in the presented article and cited literature, possibly due to the hegemonic practice to consider gender incongruence as yet another “disorder” and hence applying classical, yet inappropriate statistical analyses. In that spirit, all cited articles try to explain referrals from isolated psychiatric and demographic variables, while the true phenomenon is much more complex to describe and interpret.









留言 (0)