This interim analysis from the ongoing international STAR registry reports rates of serious perioperative bleeding complications in patients on DOACs undergoing non-deferable on-pump CABG and/or single-valve surgery with intraoperative hemoadsorption. The main observation of this report is that the intraoperative use of a hemoadsorption device resulted in low rates of serious perioperative bleeding complications in patients on DOACs undergoing isolated CABG and/or single valve surgery before completing the recommended washout period. In addition, participating investigators reported that incorporation of intra-operative hemoadsorption in their routine surgical protocol was simple and safe since there were no device-related adverse events observed.
Tens of millions of patients are on DOACs worldwide and a significant number of them will require urgent surgical intervention during the course of their therapy [1, 2, 10]. In such a scenario, high perioperative bleeding rates of up to 23% have been reported [2]. Accordingly, current guidelines recommend that patients discontinue DOACs at least 48 h prior to surgery whenever possible with even longer periods required for patients with renal insufficiency [1, 5, 11].
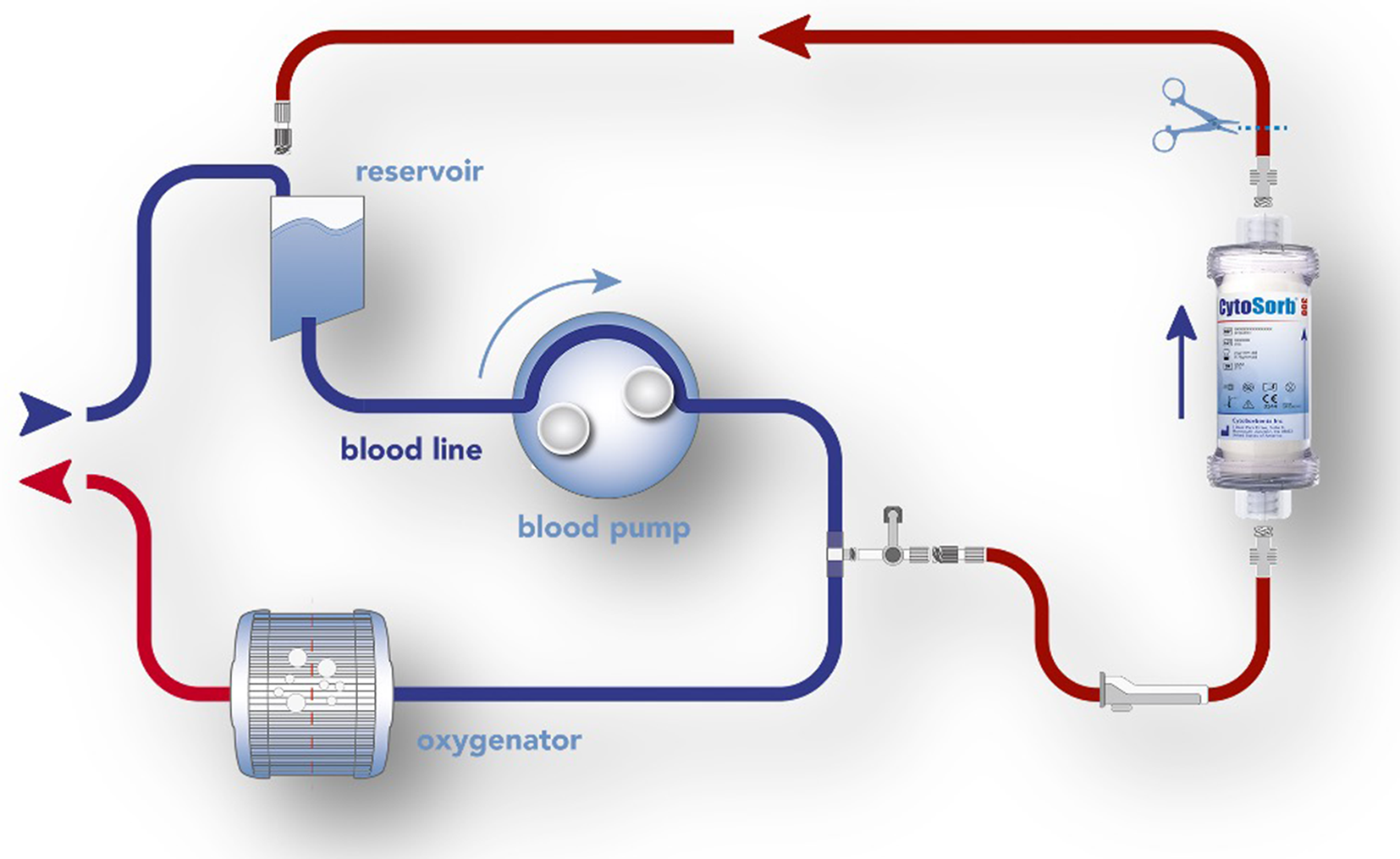
The CytoSorb hemoadsorption device (CytoSorbents, Inc., Princeton, NJ, USA) has been shown to effectively remove all DOACs from blood in the in-vitro setting [7]. CytoSorb is currently CE mark approved for clinical use for removal of cytokines, myoglobin, bilirubin, ticagrelor and rivaroxaban and can be easily integrated into any extracorporeal hemoperfusion circuit such as cardiopulmonary bypass, extracorporeal membrane oxygenation, continuous renal replacement therapy/continuous veno-venous hemofiltration or simple hemoperfusion [12]. CytoSorb is meanwhile used in various clinical settings in cardiac surgery [13].
The international STAR Registry is designed to capture high-fidelity data with the use of CytoSorb for antithrombotic removal in everyday clinical practice [6]. The current analysis focused on bleeding outcomes after CABG and/or single valve surgery in order to minimize any impact on postoperative bleeding by more complex surgery (i.e. aortic surgery or multiple valve procedures). In a recently published first analysis of the STAR registry, all types of surgery were analyzed, including complex aortic surgery, heart transplantation or combination procedures, resulting in higher UDPB and BARC-4 bleeding rates compared with the current analysis, which was intended to evaluate the impact of the device on antithrombotic related bleeding without any potential confounding due to the additional bleeding risk associated with more complex and higher risk procedures [6]. Consistent with global prescribing trends, patients in the STAR Registry were more frequently on apixaban followed by rivaroxaban and edoxaban. The overall median time from last dose to surgery in our cohort was 28.9 h, which is substantially shorter than the guideline recommendation of at least 48 h [5]. However, surgeons routinely report that their standard washout period is longer as many of their elderly patients have concomitant renal or hepatic disease, resulting in slower drug metabolism and washout. It is worth noting that in a previous analysis of cardiac surgery patients on DOACs, a longer withdrawal period, particularly in patients with reduced renal function, was essential for safe on-pump cardiac surgery [14]. The authors concluded that, despite official recommendations, patients should not be considered for elective cardiac surgery within 10 days of stopping DOAC treatment [14]. The current report was representative of an all-comer population that included approximately 1/3 of patients with some degree of renal insufficiency and to a certain extent, liver disease. Of note, for dabigatran compared to other DOACs, renal excretion is the dominant elimination pathway, but all DOACs are eliminated to a certain extent by the renal pathway as mentioned by Chen et al. All DOAC therapies are eliminated by the kidneys to varying degrees, and changes in renal clearance must be taken into account when dosing these agents. Dabigatran has the highest fraction eliminated renally at 80%, of its clearance pathway, followed by edoxaban, rivaroxaban, apixaban, and betrixaban: 50%, 35%, 27%, and 11%, respectively [15].
A study published by Hassan et al. analyzed 25 consecutive patients on apixaban who underwent cardiac surgery, 13 with CytoSorb and 12 without. In their analysis, the preoperative washout interval was 0.6 ± 1.2 days in the CytoSorb vs. 1.3 ± 0.9 days in the control group (p < 0.001). Despite the shorter washout interval, the authors concluded that no BARC-4 bleeding complications did occur in the CytoSorb group and chest tube drainage was significantly lower [10].
The bleeding rates observed in the current analysis (UDPB ≥ 3: 4.8% and BARC-4: 3.2%) are similar to rates observed among patients not on DOACs and compare favorably to rates of bleeding complications reaching 23% that have been reported in the literature for patients on DOACs [2]. In addition, we observed a low surgical revision rate of 1.6% compared to a recent analysis by Hassan et al., who reported a surgical revision rate of 11.4% (4/35) in a cohort of DOAC-treated patients undergoing cardiac surgery prior to recommended washout compared to less than 2% in the control group [16]. In the current literature, incidence of surgical revision in DOAC patients varies between 6.28% and 11.8% [14, 17].
By adopting checklists for hemostasis and a dedicated algorithm for surgical preoperative planning in elective cases, bleeding rates can be further reduced [18]. Similarly, the same authors reported an increased red blood cell (RBC) transfusion rate of 39.5% in DOAC patients compared to less than 20% in controls [16]. Therefore, the results of the present analysis, with less than 2% of surgical revisions and 24.2% of patients receiving RBC transfusion, are almost comparable to control patients not on DOACs, suggesting a significantly lower incidence of major postoperative bleeding complications with the use of intraoperative hemoadsorption.
To date, only a few studies with smaller single-center cohorts have been published on this topic. Only one study reported bleeding outcomes in isolated CABG patients with prior rivaroxaban treatment. The authors reported no surgical revisions in the CytoSorb treated group (n = 7) compared to 2 surgical revisions in the control group (n = 5). All patients treated with rivaroxaban and the use of adsorption showed a significant reduction in drug levels in the anti-factor Xa assay [16]. In another observational case series from 2 centers, the use of intraoperative hemoadsorption in patients on apixaban undergoing different types of cardiac surgery (there were no BARC-4 bleeding events and no surgical revisions in the CytoSorb group compared with 3 and 1 in the control group [10].
It is also noteworthy that no serious device-related adverse events were observed. This important observation is consistent with other published reports and may provide an important advantage for hemoadsorption over the use of reversal agents that may be associated with serious thrombotic complications in this setting. Moreover, DOAC reversal agents are expensive: Andexanet al.pha ranges from $10,000 to $12,000, idarucizumab from $5,000 to $6,000 [2]. Specifically, for andexanet al.fa, the approved reversal agent for apixaban and rivaroxaban, there are published reports of significant intraoperative complications associated with heparin reversal and resistance during CPB and high risk for thrombotic postoperative complications. Various reports [19,20,21,22] warn about the off-label use of andexanet al.fa in CPB-assisted cardiac surgery due to the anticipated development of heparin resistance and anticoagulant rebound. Similarly, a Direct Healthcare Professional Communication letter issued by the European Medicines Agency advises against the use of this reversal agent prior to heparinization since it causes unresponsiveness to the anticoagulant effects of heparin [23]. A recently published comment discussed the problems associated with reversal agents such as andexanet al.pha and the authors concluded that it seems advisable to avoid preoperative administration of andexanet al.pha in cardiothoracic procedures involving the use of a heart–lung machine; they also mentioned alternative methods for eliminating DOACs, such as hemoadsorption [24]. Intraoperative hemoadsorption is increasingly recognized as a valid alternative with a favorable safety profile and recently the latest ESAIC guidelines for the management of major perioperative bleeding [25] include a Class 2 C recommendation for the use of hemoadsorption as an adjunct in patients on ticagrelor or rivaroxaban undergoing emergency cardiac/aortic surgery on cardiopulmonary bypass to reduce bleeding complications. Moreover, Mair et al. recently published their experience with off-pump CABG and antithrombotic removal by using a stand-alone hemoperfusion pump intraoperatively [26].
Just recently, a group from Oslo published their experience with intraoperative hemoadasorption in 8 emergent apixaban-treated patients presenting with acute type-A aortic dissection. Røed-Undlien and colleagues were able to prove a significant removal of apixaban by intraoperative hemoadsorption as reflected by a significant decrease in apixaban concentrations. Interestingly the authors reported that 50% of the patients received 2,000IE of prothrombin complex concentrate (PCC) and one patient received recombinant activated factor VII (rFVIIa). Intraoperative administration of factor VII per se represents a severe bleeding event as per the UDPB definition. Of note, no surgical revisions have been reported by the authors [27].
In conclusion, these interim results from the ongoing International Safe and Timely Antithrombotic Removal (STAR) Registry show lower rates of major bleeding compared to historical cohort rates in patients on DOACs undergoing cardiac surgery before completion of the recommended washout period. Hemoadsorption appears to be a feasible, safe and potentially effective solution for reducing perioperative bleeding in this patient population.








留言 (0)