NGS-based germline multigene panel testing is an efficient way to examine multiple genes involved in hereditary cancers at once, and it is also useful for patients suspected of having hereditary breast cancer [21]. While germline testing for BRCA1/2 is covered by National Health Insurance in Japan, multigene panel testing is fully self-funded. Thus, it is not performed widely because of the high cost and because the follow-up system after testing is not yet well organized [19, 20]. The current study summarized the current status of multigene panel testing at our institution. VUSs are often identified in multigene panel testing and it is important to follow-up any individuals who have VUSs, keeping in mind that the evaluation of a VUS can change, as demonstrated in this study.
Of the 37 variants found in the multigene panel test in this study, 29 (78.4%) were VUSs. Among the VUSs identified, many were in genes known to cause hereditary breast cancer, such as ATM, CDH1, CHEK2, PALB2, and RAD51D, in addition to BRCA1/2, as well as in genes responsible for other hereditary tumor syndromes, such as APC, MLH1, MSH3, and RET. Importantly, it should be noted with extreme caution that some of the VUS evaluations changed between the time of diagnosis and the present [22]. The BRCA1/2 gene is one of the most commonly tested genes, and the significance of many of the variants is considered to be confirmed because of the large amount of data available. However, in one of our study patients, with triple-negative breast cancer and a family history, the BRCA1 variant (c.5099C>T, p.Thr1700Ile) had changed from a VUS at the time of testing to likely pathogenic in the latest ClinVar database. Moreover, three of the genes that were previously identified as VUSs (BRCA2, c.2350A>G, p.Met784Val; CDH1, c.1018A>G, p.Thr340Ala; and RET, c.341G>A, p.Arg114His) are now determined by ClinVar to be benign. Thus, it is important to monitor individuals with VUSs, since a VUS can be classified as pathogenic or benign with the accumulation of data.
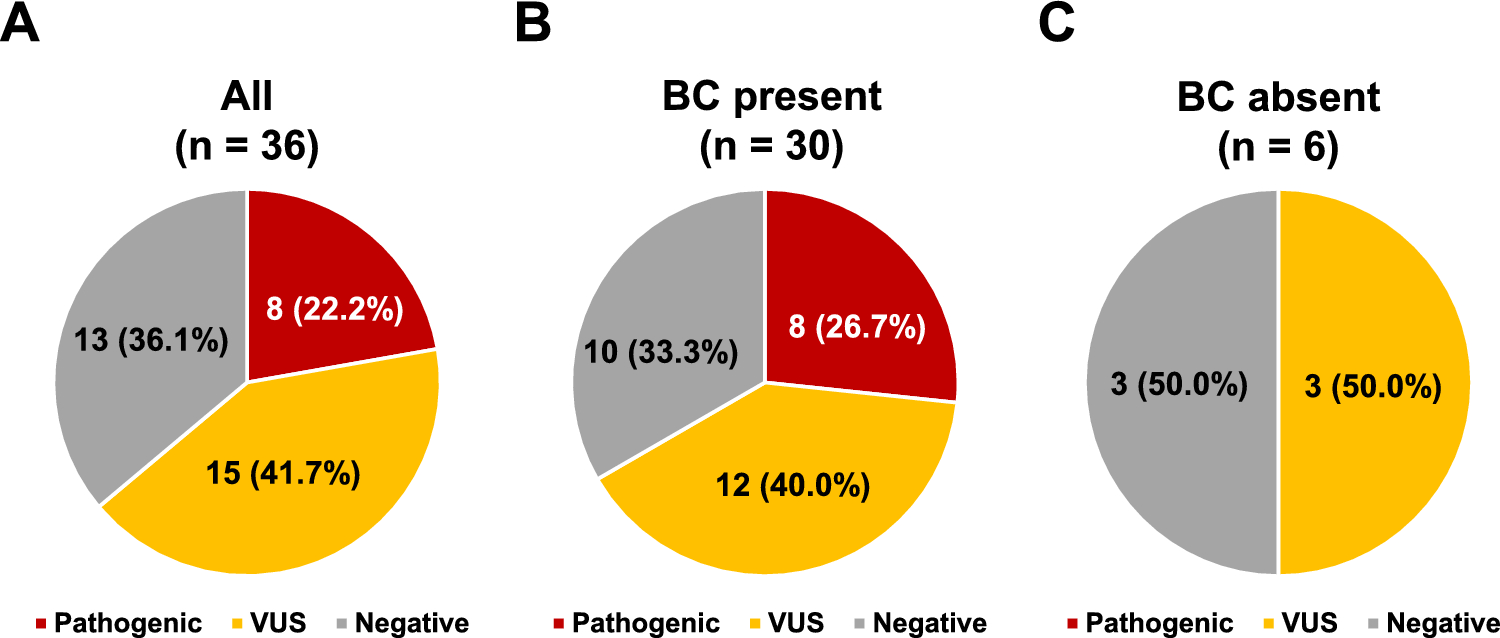
In terms of the percentage of individuals in this study who had a VUS, 15 of the 36 (41.7%) had a VUS only and no pathogenic variant. Previous reports have reported a high frequency of VUS in multigene panel testing, generally exceeding 40% [23,24,25,26]. As in our case, VUS is more likely to turn benign than pathogenic [27], so VUS should not be used to guide medical management, nor should treatment proceed based on VUS [28]. Taken together, a decision must not be made until the clinical significance of the VUS is known, and since the multigene panel testing will find a VUS in many individuals, many subjects will need ongoing follow-up.
Of the 36 individuals tested in this study, 8 (22%) were found to have pathogenic variants, which represents a high frequency. This is partly because we included individuals from 2016 to 2019, before BRCA1/2 genetic testing was covered by National Health Insurance. During that period, individuals with a strong suspicion of heredity were being offered multigene panel testing instead of BRCA1/2-only germline tests, because of the high cost of both BRCA1/2-only and multigene panel testing. Consequently, the frequency of pathogenic variants of BRCA1/2 in this study was also high, (n = 5; 13.9%), compared with the commonly reported frequency of BRCA1/2 variants in breast cancer, which is 4%–5% [5].
In addition to BRCA1/2, we found variants in MLH1 and RNT1 among the pathogenic variants identified in this study. A patient with a variant in MLH1 identified is under surveillance for Lynch syndrome. RINT1 does not represent a moderate-penetrance breast cancer susceptibility gene [29], so surveillance was deemed unnecessary for an individual with a variant in RINT1. However, biallelic variants in RINT1 have been reported to cause liver failure and other problems [30, 31]; therefore, they could be considered an unaffected carrier, so genetic counseling was offered to provide this information. Taken together, each pathogenic variant identified by multigene panel testing requires a unique follow-up system and individualized care for every variant, since each gene has different penetrance, different organs susceptible to cancer, and in some cases may be associated with diseases other than cancer.
In Japan, National Health Insurance does not yet cover multigene panel testing of the germline, meaning patients must pay the full cost. If testing was covered by National Health Insurance, patients would have to pay only 10% to 30% of the cost, depending on their age. Moreover, all medical procedures based on test results not covered by National Health Insurance are not covered by this insurance and must be fully funded by the patient. For instance, if prophylactic resection or surveillance is required based on the results of multigene panel testing, the additional cost to the patient will be high. The benefit of performing multigene panel testing is that it improves the detection rate of genetic variants and increases the likelihood that a patient will be diagnosed with a hereditary tumor [19, 20]. The harm of testing is that if a variant is identified, many gene-based risk measures for familial tumors have not been established yet, and VUSs are also identified at high rates, which can lead to unnecessary anxiety and the disadvantages of excessive testing and treatment [19, 20].
This study has some limitations. First, it was retrospective in nature with a small number of samples; however, it enabled us to identify trends in germline variants in patients suspected of having hereditary breast cancer and demonstrate the features of multigene panel testing and points to be aware of. Second, the identification of germline variants by multigene panel testing is not yet widespread in Japan and there are many challenges for performing multigene panel testing, such as: (i) the cost of the test, which is not covered by National Health Insurance; (ii) the fact that surveillance and prophylactic resection based on the results of the gene test are at the patient’s own expense, and an adequate follow-up system after the test has not been established; (iii) the fact that VUSs are common and such patients require ongoing follow-up; and (iv) the gene panels covered differ depending on the testing laboratory, and are not standardized as they are subject to additions and deletions of genes at any time.
In conclusion, we reported on the current status of multigene panel testing performed for individuals with suspicious hereditary breast cancer in our institute. Our results demonstrate that multigene panel testing is a useful tool that can identify variants. One of the outcomes of this testing is that VUSs are frequently identified, and it is important to monitor these individuals because VUS evaluations can change over time with the accumulation of data. In Japan, the experience in genetic medicine that has been cultivated for hereditary breast and ovarian cancer treatment should be applied and utilized for patients with genetic variants other than BRCA1/2.





留言 (0)