
記住我


Learning taxonomies present valuable opportunities for advancing medical education and simulation, significantly enhancing learning outcomes [1]. Among these, Bloom’s taxonomy, originally introduced in 1956 and revised in 2001, is an essential framework for crafting and assessing educational objectives, focusing on three integral domains: cognitive, affective, and psychomotor [2, 3].
Recent discussions by Tuma and Nassar et al. illustrate Bloom’s taxonomy as a promising framework for clinical surgical education, presented in a simplified way with clinical examples [4]. However, there is a notable gap in its implementation within bariatric surgery training. Embracing this taxonomy in bariatric surgical education could effectively support curriculum development and improve the assessment of learning outcomes, thereby elevating training programs.
Particularly, the psychomotor domain plays a vital role in the training of bariatric surgeons, as it is indispensable for cultivating technical skills and manual dexterity [5]. While the cognitive and affective domains aid in knowledge acquisition and emotional investment, psychomotor skills are essential for hands-on practice [4, 6]. This domain facilitates a structured progression from basic imitation to expert-level performance, underscoring the importance of physical engagement in mastering surgical techniques [7]. By prioritizing the psychomotor domain, we can lay a solid foundation for future surgeons in the field of bariatrics [4, 6, 7].
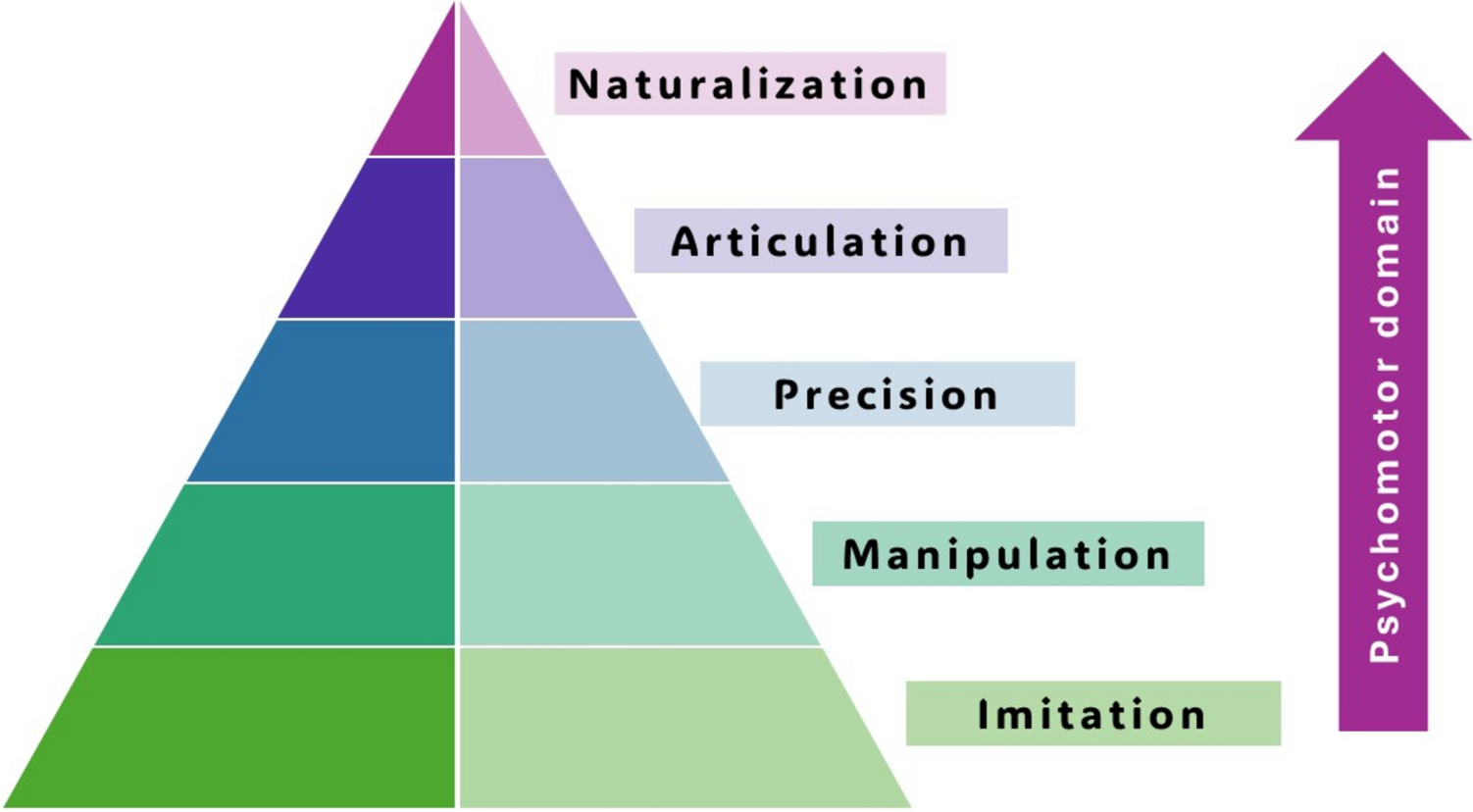
In the context of bariatric surgery training, skill development adheres to Bloom’s psychomotor taxonomy [8] (Fig. 1). The initial stage, imitation, involves the observation of surgeries to grasp the intricacies of operating room dynamics and the rationale behind clinical decision-making. This is followed by manipulation, where trainees engage in closely monitored practice sessions to cultivate confidence and develop necessary muscle memory [9].
Fig. 1
The stages of Bloom’s psychomotor domain, illustrating the progression from basic imitation to advanced naturalization in skill development
Advancing to the precision phase, practitioners perform surgical steps with a significant degree of autonomy, emphasizing accuracy and patient safety. The articulation stage requires the integration of multiple skills, enabling trainees to execute surgeries independently while also guiding less experienced colleagues [10, 11]. Finally, naturalization is achieved when surgical competencies become instinctual, allowing trainees to operate proficiently and autonomously, demonstrating a high level of mastery without the need for supervision [12].
The 2001 revision of Bloom’s taxonomy delineated the cognitive domain into six hierarchical levels: remembering, understanding, applying, analyzing, evaluating, and creating (Fig. 2). This revised framework facilitates a movement from basic memorization to higher-order cognitive tasks like critical thinking and innovation, operationalized through action-oriented verbs such as “analyze” and “create” [3, 6]. At the initial stages, trainees focus on remembering key facts, such as the surgical steps and patient criteria. As they progress, they move to understanding, where they can explain the rationale behind procedures, followed by applying, where they start performing specific tasks under supervision. As trainees gain more experience, they advance to analyzing surgical situations, identifying complications, and evaluating patient outcomes [4].
Fig. 2
The revised Bloom’s taxonomy, highlighting the hierarchical levels from remembering to creating
Bloom’s taxonomy continues to facilitate growth as trainees move toward higher cognitive tasks. In the evaluating stage, they critically assess surgical outcomes, making decisions based on evidence and patient progress to refine their techniques. At the highest level, creating trainees is expected to innovate or propose new approaches to bariatric surgery. Learning curves vary for each individual, but applying Bloom’s taxonomy provides a clear structure for assessing and demonstrating a trainee’s level of competence, helping to tailor education and skill development to each stage of their training, ultimately fostering more effective learning in bariatric surgery [13].
In the context of bariatric surgery training, this taxonomy serves as a complement to the development of psychomotor skills. Trainees initially commit protocols to memory and comprehend their underlying principles. Following this foundational stage, they practice surgical techniques under supervision, engage in the analysis of procedural challenges, and conduct evaluations of outcomes to refine their methods. Ultimately, they reach a stage where they can innovate and execute intricate procedures independently [6, 7].
The integration of cognitive and psychomotor training in surgical education poses distinct challenges. Trainees may demonstrate exceptional technical abilities yet struggle with critical thinking or creative problem-solving if the curriculum fails to adequately balance these domains. Programs such as observerships and fellowships, particularly those associated with the Young International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO), are pivotal in bridging this gap [7, 14, 15].
Observership allows trainees to observe complex surgeries within high-volume centers, providing valuable insights into operating room dynamics, clinical decision-making, and surgical strategies. These programs prioritize understanding and analysis—allowing participants to enhance cognitive skills, particularly critical thinking and adaptability, without direct involvement in surgical performance [7, 16, 17].
Conversely, fellowships deliver immersive experiences where trainees actively engage in surgical procedures under the mentorship of expert surgeons [7, 18]. These programs focus on the application and refinement of psychomotor skills, alongside the critical evaluation of outcomes and the innovation of surgical techniques. Collectively, observerships and fellowships foster a comprehensive integration of cognitive and technical training, cultivating surgeons who excel not only in operative proficiency but also as adept decision-makers and innovators within the realm of bariatric surgery [19].
The implementation of structured checklists to assess mastery across the taxonomy levels is vital for optimizing the learning trajectory. These checklists facilitate systematic tracking of progress within both cognitive and psychomotor domains, identifying specific areas for improvement, thereby enhancing training outcomes and promoting holistic skill development [19].
留言 (0)