The main finding of the present study was that the relative frequency of accepted claims for men was twice the figure for women. The number of compensation claims by males was almost 2/3 of the total number of claims. This can be explained by the fact that the frequency of compensation claims by men where the cause was infection was much higher than the corresponding frequency for women. One study has reported that men are more involved in shared decision-making processes than women. Despite this, our study reveals that men have more compensation claims accepted. Our sensitivity analysis, where we removed infection as a reason for compensation claims, showed that there was no gender difference in acceptance without infection as the cause (p = 0.16). The literature demonstrates that men have a higher risk of infection following meniscal surgery [16, 17]. It has been stated that this might be due to different baseline bacterial colonization of the skin by the two genders, and also that it might be due to more hair growth and thus need for shaving in men [18]. In the NPE system, compensation claims because of infection tend to be accepted, amounting to almost 93% in our database. This is consistent with other papers on the topic [9, 10, 13, 14].
It is important to assess and reinforce changes due to treatment failures. Incident reports and complaint management are important factors of the “continuous improvement cycle” [19]. We believe this applies to both hospital level and national levels. On a hospital level this can be taken care of with proper quality systems, and a culture for constructive managing of the complaints and treatment errors [19]. On a larger scale, registry based studies like ours can be important factors for reinforcing changes in treatment and decision-making.
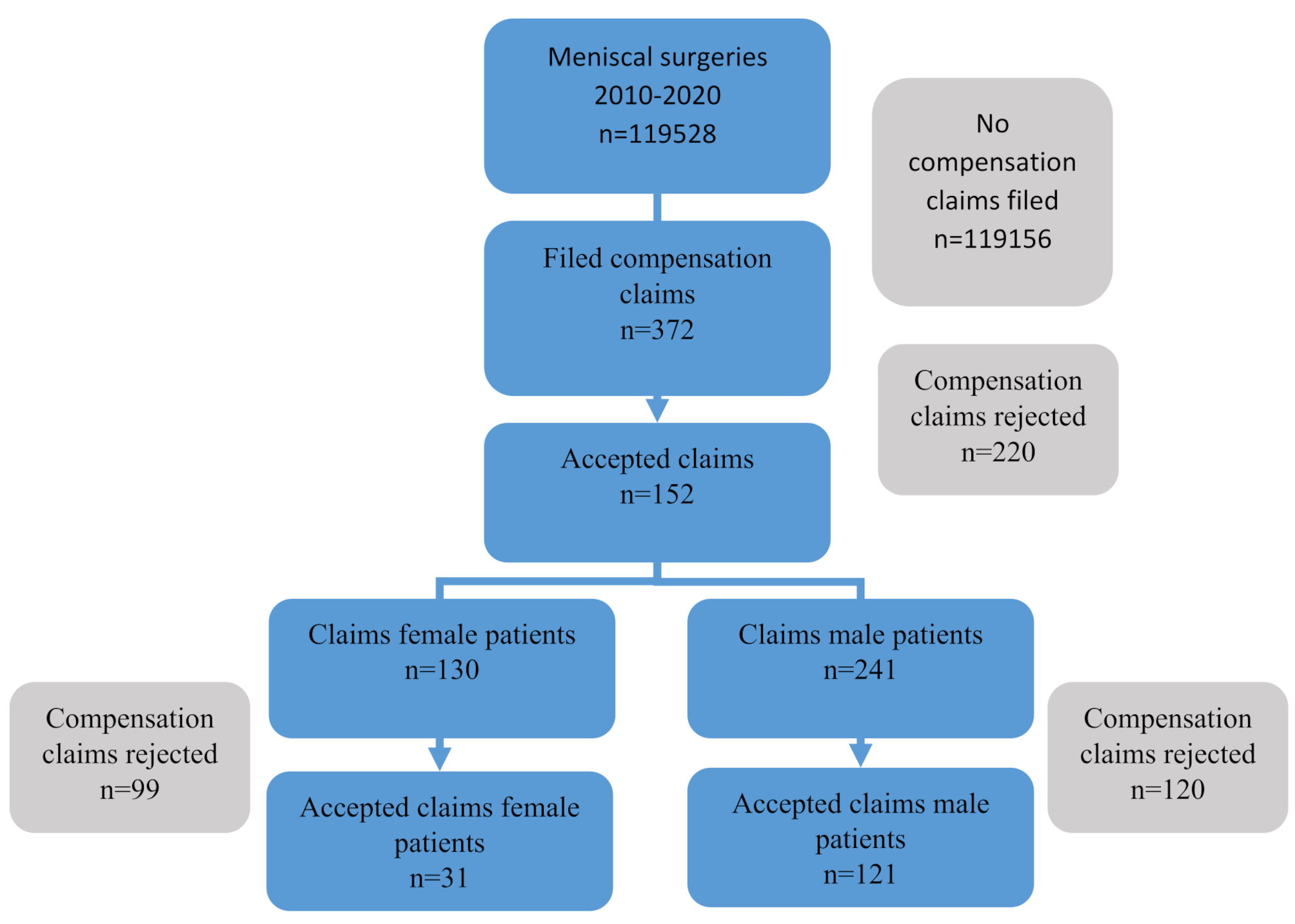
In the study period, 0.3% of patients filed a compensation claim and 0.13% were accepted. Pain was the single most frequent reason for filing a compensation claim, with 114 claims among the more than 119,500 surgeries (0.1%). Pain is the cardinal symptom of early osteoarthritis (OA), and some of the surgeries might have been performed on early OA where a meniscus injury was associated with, or part of the process in, the aging knee [20, 21]. As outlined in the results of the present study, compensation claims were most frequent in the higher age groups, which supports this assumption. These patients received compensation in fewer than 2% of the cases. Pain is a rather subjective complication, and no tests can be performed to confirm this treatment error. It can be due to intra-articular damage, such as cartilage lesions, progression of osteoarthritis, complex regional pain syndrome, arthrofibrosis, etc. It can also be due to the original condition, i.e. the problem was not solved by the arthroscopic procedure. Recent literature recommends alternative approaches to surgery for a degenerative meniscus injury [22, 23]. Our data do not discriminate between the different causes of pain. However, iatrogenic damage and complex regional pain syndrome are separate reasons for compensation claims. The former claims were filed in 3 (0.003%) cases, which were all accepted, while the latter were filed in 2 (0.002%) cases and neither of these was accepted. Many articles on complications of meniscal surgery do not report pain as a complication. Hagino et al. did not see any cases of complex regional pain syndrome in a study of more than 2.600 cases. 2 out of these cases did, however, develop postoperative infection, and 2 developed VTE [24]. Pajalic et al. published in 2018 a comprehensive article on 18,735 patients who underwent knee arthroscopy in Sweden [25]. They found an overall complication rate of 1.1%. The three most reported complications were complications not classified elsewhere (33%), thrombophlebitis (24%) and pulmonary embolism (14%) [25]. However, they only focused on complications in the 30 days following arthroscopic procedures in the knee [25]. This differs from our results, which show that 13 (0.01%) compensation claims were filed because of VTE or pulmonary embolism 2 of which (15%) were accepted.
Wrong technique was the third most frequent reason for compensation claims in our data. 38 (0.03%) compensation claims were filed for this reason, and they were accepted in 45% of the cases. Our data do not reveal whether the errors were caused by inexperienced surgeons, who either did not use the technique correctly or chose the incorrect technique at the outset. Examples could be that the surgeon tried to use cortical fixation for a meniscal root tear but placed the suture channels incorrectly, or that the surgeon did not realize that there was a root tear in the first place, and therefore did not address it. Nevertheless, little has been written about wrong techniques. Inexperience can also lead to higher surgical time, which increases the likelihood of complications. In 2006, Reigstad et al. found a complication rate of 5% in 876 cases, but only 0.7% had therapeutic consequences. In their data they found that the time spent on the procedure was the only factor that influenced the rate of complications, thus not the use of a tourniquet [26]. In a larger study by Gowd et al. of almost 79,000 arthroscopic knee surgeries, only small increases in surgical time increased the risk of complications such as postoperative infections, sepsis and readmissions [27].
Impaired function/instability and nerve lesion complaints were filed in 25 (0.02%) and 22 (0.02%) cases respectively. The patients received compensation in 8% and 14% of the cases.
Delayed treatment/surgery
21 patients (0.02%) filed a claim for compensation for delayed treatment or surgery, and 7 (33%) of these were successful. This seems reasonable, as many meniscal tears are chronic. A patient with a long relevant medical history is not likely to benefit from faster treatment, and according to Pihl et al., there is no subgroup that benefits more from meniscal surgery than others [28]. In addition, shorter time to surgery was not a success factor [28]. It seems, however, reasonable to treat patients with acute trauma more promptly. When a repair of the meniscus is indicated, it is advised to do this as soon as possible [29]. This can explain the figure of 33% who received compensation in this group.
Wrong or no indication
16 (0.01%) patients filed a claim for this reason, and almost all of them (93%) were granted compensation. The mean age and volume of meniscal resection continued to rise in this period [30, 31], despite the questionable results of arthroscopy for degenerative knees [32, 33]. The study of Kise et al. indicates that one can achieve good results with supervised exercise alone in this group of patients [34]. This may be the reason why such a high percentage received compensation in this group.
Limitations of the study
In Norway, there is unfortunately no registry based on meniscal surgery. This means that we cannot determine whether our findings from the NPE are caused by different frequencies of filing complaints based on gender, or whether there actually is a difference in complications between the genders. However, other papers support the findings of gender differences [9, 10, 13, 14, 35], especially with regard to infection. Another limitation is the criteria for the NPE to accept compensation claims. Studies show that we can expect more complications than the 0.13% of accepted claims in the NPE [2, 36]. The vast difference in frequency between the types of claims accepted may also in turn affect whether people bother to file a claim or not, i.e. because compensation for infections is more often granted than for pain, people experiencing pain as a treatment error after meniscal surgery might be less likely to file a compensation claim in the first place. Further, the NCSP classification does not discriminate between the different types of meniscal sutures. We therefore have no data on possible differences between all-inside, inside-out and outside-in techniques in cortical sutures for meniscal root tears. However, the literature suggests that there is no difference [3]. Also, our study only included patients going through surgery, and not other treatment options such as physiotherapy or knee joint injections. All the patients in the study were all from one single country, and this may of course affect the generalizability of the study. Finally, being a cross-sectional study, we cannot perform causal inference. Such studies may also be susceptible to bias [37].
Strengths of the study
The main strength of this study is that we examined more than 119,000 procedures over a period of 10 years. To our knowledge, there are no studies outnumbering the present study with respect to included subjects on compensation claims on meniscal knee surgery. In addition, the NPR and NPE registries have high consistency and completeness, and patients are unable to opt out. Hence, the figures are trustworthy [38] and reflect current practice and risk with this common knee surgery procedure. Collection of data on inferior outcomes is a powerful tool to study weak aspects of our current care in all fields of medicine and in this particular study meniscal surgery is in focus. This is valuable information for both knee surgeons and caregivers, and can be used to prevent treatment errors in the future. Our data suggest that additional precautionary measures should be taken when operating on men. Although the relative frequency of infection is low in both men and women, our data indicate a much higher relative frequency of infection following knee meniscal surgery in male patients. This study demonstrates the importance of reducing treatment errors when providing health care and to prevent to such errors to occur.







留言 (0)