
記住我


This study retrospectively included 83 patients with cervical spondylosis who were treated at our hospital from September 2022 to September 2023 as the experimental group, including 28 cases of the axial joint pain (Group A), 29 cases of the cervical radiculopathy (Group B), and 26 cases of the cervical myelopathy (Group C). Additionally, 29 individuals who underwent health examinations during the same period were selected as the control group (Group D). This research was conducted following the approval of our institution’s ethics review board (IRB number 2022JJ40696).
Inclusion criteria: (1) The patients with cervical spondylosis met the diagnostic criteria for one of the following types of cervical spondylosis: axial joint pain, cervical radiculopathy or myelopathy. ①For axial joint pain: classic symptoms of neck pain radiating to areas such as the medial scapula, chest wall, shoulder, and head, with no neurological deficits observed and pain induced by neck movement.②For cervical radiculopathy: classic symptoms such as neck pain radiating to the upper extremities, accompanied by weakness and/or numbness, positive spurling sign, and radiographic evidence of nerve root compression. ③For cervical myelopathy: classic symptoms including weakness in all four extremities and a sensory level indicating reduced or absent pain, touch, vibration, or position sense, clinical findings of weakness, hyperreflexia, or coordination changes, and radiographic evidence of spinal compression. ④ For healthy individuals: there were no symptoms or signs of cervical spondylosis, normal cervical spine curvature on X-ray, and no significant degenerative changes, disc herniation, spinal canal stenosis, or spinal cord compression on MRI. (2) Age between 35 and 70 years; (3) Possessing complete cervical spine MRI and X-ray imaging data; (4) Body Mass Index (BMI) between 18.5 and 23.9.
Exclusion criteria: (1) History of cervical spine trauma or previous head and neck surgery; (2) Severe cervical deformities, tumors, tuberculosis, or neurological diseases affecting the vestibular or visual systems; (3) Presence of infectious diseases or psychiatric disorders; (4) Poor MRI image quality that prevents delineation of muscle boundaries; (5) Presence of two or more mixed types of cervical spondylosis.
Examination methodsAll subjects underwent cervical spine MRI and X-ray examinations. Cervical spine MRI was performed using a MAGNETOM Verio 3.0 T magnetic resonance imaging system manufactured by Siemens AG, Germany. The scanning range was from the first cervical vertebra to the second thoracic vertebra, showing the entire vertebrae, intervertebral discs, bilateral appendages, and paraspinal soft tissues, using Spin Echo and Short Tau Inversion Recovery sequences. Slice thickness was 3.0 mm, inter-slice gap was 1.0 mm, and the matrix was 320 × 224. The lateral cervical spine X-ray scanning range was from the orbits to the upper thoracic segment, centered at the C4-5 vertebral level.
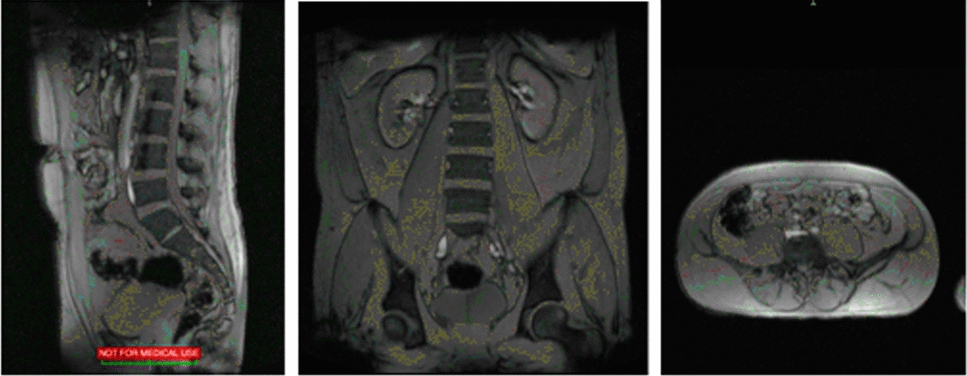
Imaging measurementsT2-weighted axial MRI images were obtained at the C3-4, C4-5, and C5-6 intervertebral disc levels, and the average of these measurements represented the final result. The study included deep flexor muscles, deep extensor muscles, and superficial extensor muscles of the cervical spine. The deep flexor muscles included the longus colli and longus capitis, the deep extensor muscles included the multifidus, semispinalis cervicis, semispinalis capitis, and rotatores, and the superficial extensor muscles included the splenius capitis, splenius cervicis, longissimus capitis, and levator scapulae. Using Image J software (version 1.52, USA), the CSA of each muscle group was measured by placing a graphical cursor around the region of interest, including the deep extensor area (DEA), deep flexor area (DFA), and superficial extensor area (SEA). The FI ratio is defined as the proportion of the fatty tissue area to the muscle CSA. Appropriate thresholds for the region of interest were set, and pseudo-coloring techniques were used to dye the gray areas of fatty tissue red, then the FI ratio of each muscle group was calculated, including the deep extensor fatty infiltration ratio (DEFIR), deep flexor fatty infiltration ratio (DFFIR), and superficial extensor fatty infiltration ratio (SEFIR), as shown in Fig. 1. All measurements were taken by two experienced orthopedic physicians, and the average value was used.
Fig. 1
Measurement of cross-sectional area and fatty infiltration ratio of cervical paraspinal muscles. A: Measurement of the region of interest area using Image J software, where 1 and 2 represent the deep extensor area, 3 and 4 represent the superficial extensor area, and 5 and 6 represent the deep flexor area. B: Pseudo-coloring technique was used to dye the fatty tissue red, with the yellow part representing the fatty tissue of the target muscle group. The FI ratio is defined as the proportion of the fatty tissue area to the muscle CSA
Using the Picture Archiving and Communications Systems, the C2-7 Cobb angle was measured on lateral cervical spine X-ray images to assess cervical curvature. As shown in Fig. 2, a parallel line is drawn along the inferior endplate of the C2 vertebral body and another along the inferior endplate of the C7 vertebral body. Perpendicular lines are then drawn from these parallel lines, and the angle formed between the perpendicular lines is measured. The acute angle is taken as the measurement value, known as the Cobb angle. If the cervical curvature is lordotic, the Cobb angle is recorded as a positive value; if kyphotic, it is recorded as a negative value. The magnitude of the value indicates the degree of lordosis or kyphosis.
Fig. 2
C2-7 Cobb angle measurement method: A parallel line (A) is drawn along the inferior endplate of the C2 vertebral body and another parallel line (B) along the inferior endplate of the C7 vertebral body. Then, perpendicular lines (C and D) are drawn from lines A and B, respectively. The acute angle between lines C and D is the C2-7 Cobb angle
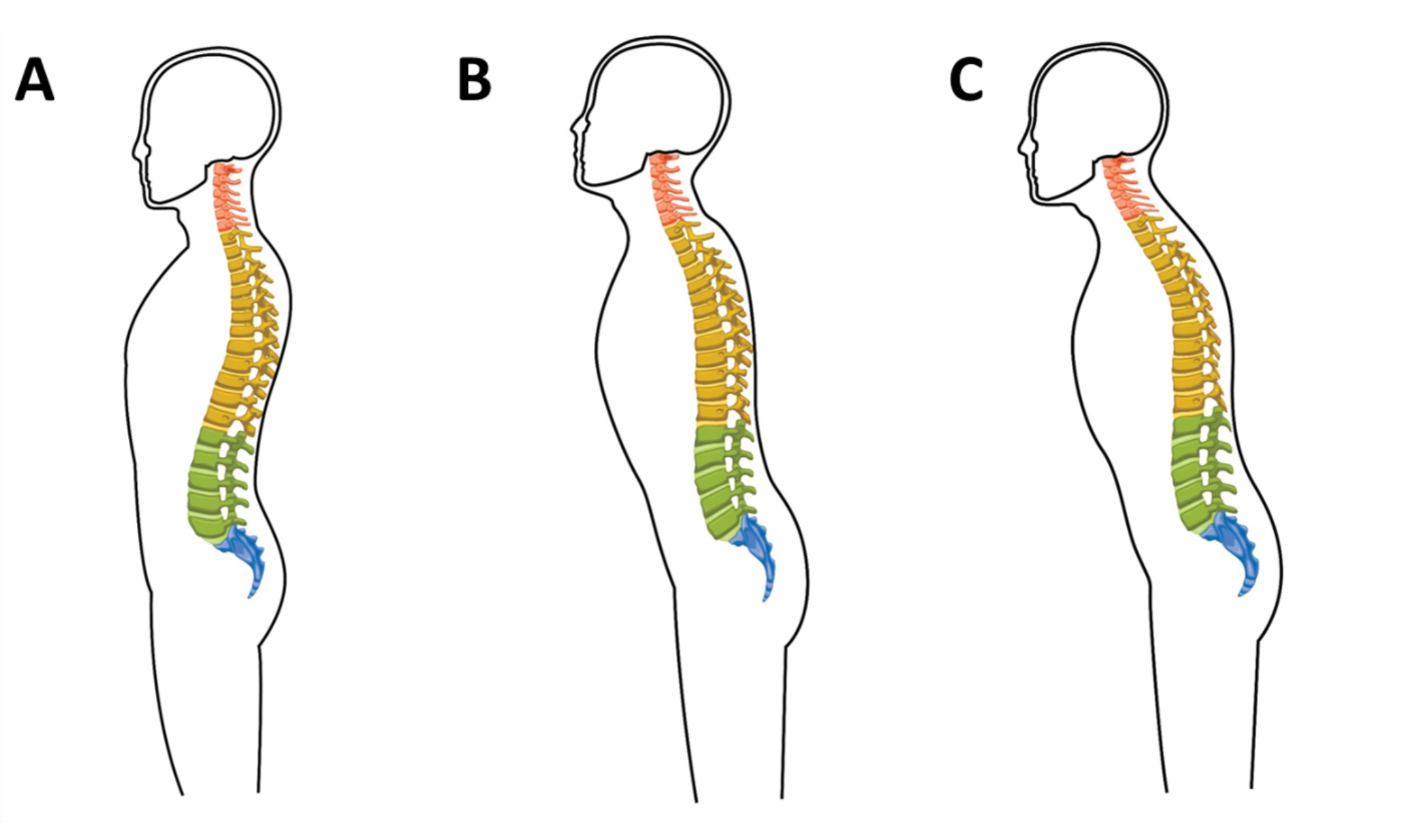
Intervertebral disc degeneration grading assessmentMRI T2WI mid-sagittal images clearly show the condition of the intervertebral disc, including the nucleus pulposus structure, the boundary between the annulus fibrosus and nucleus pulposus, signal intensity, and disc height. Given the multiple segments of the cervical spine and varying degrees of degeneration, the C5-6 segment, located at the center of the cervical lordosis and bearing significant stress, was chosen for analysis as it is the earliest and most commonly affected segment in cervical disc degenerative disease. The severity of disc degeneration at the C5-6 segment was evaluated using the Pfirrmann grading system on sagittal T2WI sequences to assess the extent of intervertebral disc degeneration [16, 17] (Fig. 3). The grading assessments were conducted by two experienced orthopedic physicians. In cases of disagreement, a reassessment and discussion were carried out, and a third physician made the final judgment.
Fig. 3
Pfirrmann grade of disc. Grade 1: Homogeneous, bright white structure, clear distinction of nucleus and annulus, hyperintense, isointense to cerebrospinal fluid signal intensity, and normal height of intervertebral disc; Grade 2: Inhomogeneous with or without horizontal bands, clear distinction of nucleus and annulus, hyperintense, isointense to cerebrospinal fluid signal intensity, and normal height of intervertebral disc; Grade 3: Inhomogeneous, gray structure, unclear distinction of nucleus and annulus, intermediate signal intensity, and normal to slightly decreased height of intervertebral disc; Grade 4: Inhomogeneous, gray to black structure, lost distinction of nucleus and annulus, intermediate to hypointense signal intensity, and normal or moderately decreased height of intervertebral disc; Grade 5: Inhomogeneous, black structure, lost distinction of nucleus and annulus, hypointense signal intensity, and collapsed disc space height of intervertebral disc
Statistical methodsThe data were analyzed using SPSS 26.0 software. Measurement data were described using mean ± standard deviation, and categorical variables were expressed using frequency and percentage. Quantitative data following a normal distribution were compared between two groups using the t-test, while comparisons among multiple groups were performed using ANOVA; non-normally distributed data were analyzed using the rank-sum test. If statistical differences were found in the ANOVA, post-hoc pairwise comparisons were conducted using the LSD-t method. Correlation analysis between variables was performed using Pearson correlation analysis, with the correlation coefficient (r) used to measure the strength of the correlation. P < 0.05 indicated statistical significance.
留言 (0)