
記住我

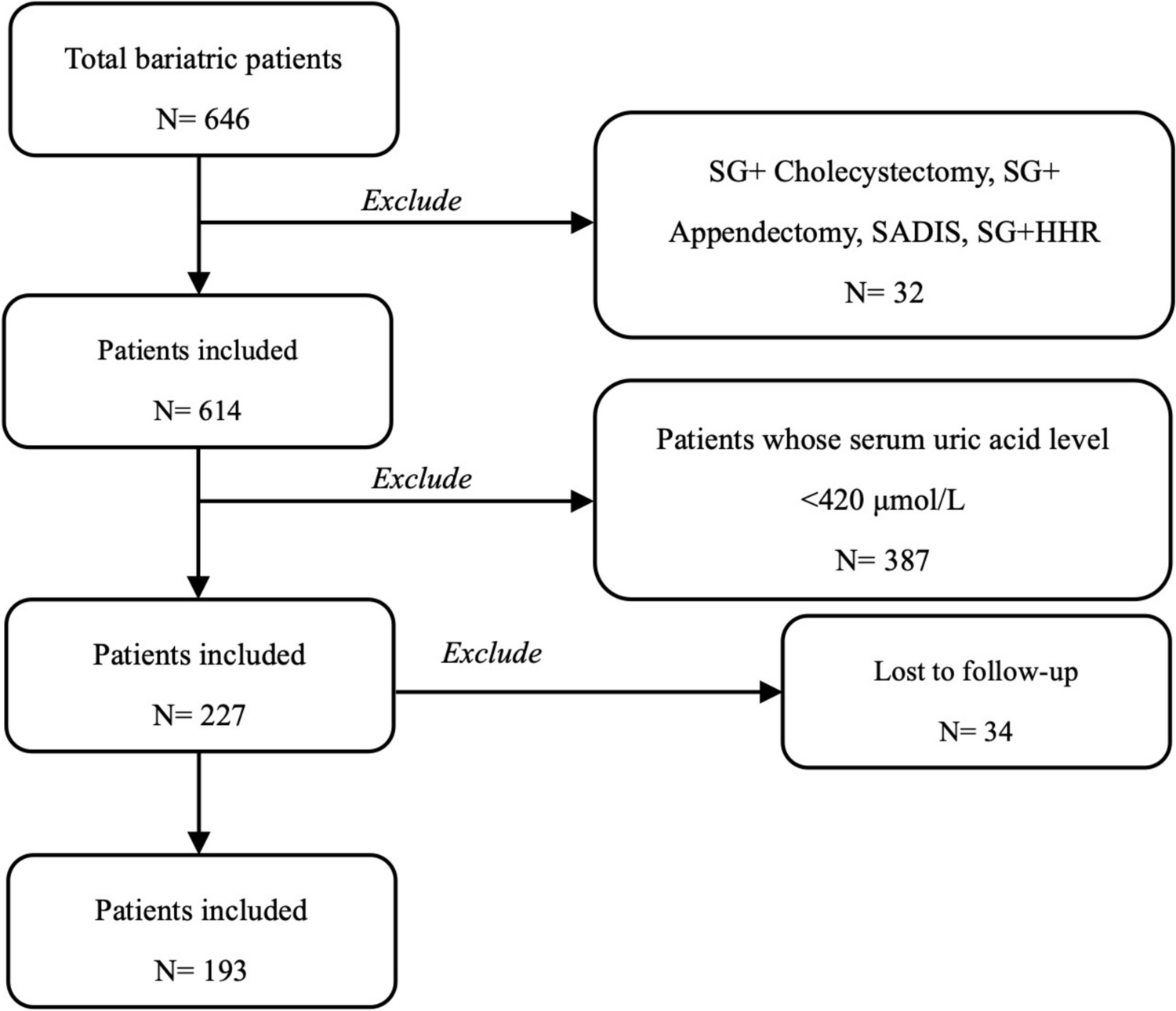

From the time of protocol implementation, between November 2023 and July 2024, 53 youth had surgical consults, and 46 (86% conversion rate; mean age 16.5 ± 1.9 years, mean BMI 53 ± 9.7 kg/m2; 70% (32/46) female, 80% (37/46) Hispanic, 87% (40/46) publicly insured) underwent LSG, with 93% (43/46) using obesity pharmacotherapy preoperatively; Table 1). Over half of the participants (54%, 25/46) self-selected early reinitiation of an obesity pharmacotherapy (median [IQR] time to re-initiation 5.1 weeks ([3.7, 8.4]). The three youth who were not on an obesity pharmacotherapy prior to surgery self-selected the standard of care arm and remained off medication after surgery. Of those who reinitiated an obesity pharmacotherapy, 56% (14/25) resumed their pre-surgery regimen, with 52% (13/25) starting more than one agent. The medications reinitiated postoperatively included semaglutide (17/25), phentermine (11/25), topiramate (7/25), metformin (7/25), and tirzepatide (2/25; Table 2). At surgical consult, and at 1-, 2-, and 3-months postoperatively, there were no missing data points, with a complete dataset available for all 46 youths. At 6 months postoperatively, the following number of youths had not yet reached the time point at the time of publication: Early Reinitiation (n = 9) and Standard Care (n = 11). Consequently, primary and secondary data were analyzed for the following sample sizes: Early Reinitiators (n = 16/25) and Standard Care (n = 10/21).
Table 1 Clinical and safety outcomes between early obesity pharmacotherapy reinitiators and standard care in a clinical cohortTable 2 Obesity pharmacotherapy selection pre- and postoperatively in a clinical cohort including mean time to reinitiation after laparoscopic sleeve gastrectomy in those who self-selected early reinitiation (n = 25). Over half (56% [14/25]) resumed their pre-surgery regimen, with 52% (13/25) starting more than one agentChange in Weight TrajectoryFigure 1 demonstrates the within subject change in percent BMI from surgical consult to last anthropometric point available to highlight individual response across the cohort between groups. At 3 months postoperatively, the mean (SD) change from surgical consult in absolute BMI (kg/m2) was −10.5 (2.0) kg/m2 for early reinitiators and −7.3 (2.3) kg/m2 for standard care, representing a difference of −3.2 kg/m2 (p \(\le\) 0.001, Table 2). The correlating mean (SD) percentage change in BMI at this time was −19.4% (4.8%) for early re-initiators and −14.7% (4.4%) for standard care, with a difference of −3 percentage points (p < 0.001). At 6 months postoperatively, the mean change in absolute BMI was −13.5 (1.7) kg/m2 for early reinitiators (missing data n = 9) and −8.9 (1.7) kg/m2 for standard care (missing data n = 11), showing a difference of −4.6 points (p < 0.001). The mean (SD) percentage change in BMI at 6 months was −24.3% (4.7%) for early reinitiators and −18.4% (4.3%) for standard care, with a difference of −5.9% (p = 0.004). Additionally, at 3 months postoperatively, youth in the early reinitiation group demonstrated a greater reduction in %TWL and %EWL compared to standard care, representing a difference of −4.4% and 6% respectively (Table 3). Mixed effect multivariate regression analysis, adjusting for baseline BMI, age, and sex, was conducted for each arthrometric measure and revealed that early reinitiation significantly reduced absolute weight (kg), BMI (kg/m2), percent BMI, percent TWL, and percent EWL at 3 and 6 months postoperatively compared to standard care (Table 4). At 6 months, mean differences between groups with 95% confidence intervals included: BMI: −4.6 (−5.94, −3.25), p < 0.001; %BMI: −6.5 (−9.13, −3.86), p < 0.001; %TWL: −5.9 (−8.52, −3.25), p < 0.001; %EWL: −8.2 (−14.69, −1.63), p < 0.001; Table 4).
Fig. 1
Waterfall plot demonstrating the individual change in percent BMI postoperatively compared to baseline between early obesity pharmacotherapy reinitiators (n = 25) compared to standard care (n = 21) from a clinical sample
Table 3 Change in weight trajectory overtime between early obesity pharmacotherapy reinitiators and standard of care in a clinical cohort from initial surgery consult date to 6-months post-operativelyTable 4 Change in weight trajectory overtime between early obesity pharmacotherapy reinitiators and standard of care assessed utilizing a multivariate mixed-effects linear regression model controlling for baseline body mass index, age at time of consult, and sex in a clinical cohortSemaglutide Sub-AnalysisA sub-analysis was conducted on youth who were taking semaglutide 2.4 mg weekly (n = 18) for at least 3 months prior to LSG and then reinitiated the medication immediately postoperatively (median [IQR] time to reinitiation 5.0 weeks [3.7, 8.4]. Early reinitiators (n = 17) experienced greater reduction in both absolute BMI and %BMI change at 3 months (median [SD[ BMI [kg/m2]: −10.7 [2.1] vs. −7.3 [2.3]; p \(\le\) 0.001; %BMI: −20 [5.4] vs. −14.7% [4.4]; p < 0.001) and mo. 6 (BMI [kg/m2]: −13.3 [1.7] vs. −8.9 [1.7]; p < 0.001; %BMI: −24% [5.1] vs. −18.4% [4.3]; p = 0.02) compared to the standard care (n = 21; Fig. 2). Mixed effect multivariate regression analysis, adjusting for baseline BMI, age, and sex, was conducted for each arthrometric measure and revealed that early reinitiation significantly reduced absolute weight (kg), BMI (kg/m2), percent BMI, percent TWL, and percent EWL at 3 and 6 months postoperatively compared to standard care (Table 4).
Fig. 2
Change in percent body mass index between early semaglutide reinitiators (n = 18) vs. standard care (no obesity pharmacotherapy, n = 21) from a clinical sample
Eating BehaviorsWhile all youth (n = 46) reported a 50% reduction in hunger on the AEBQ [34] completed 2 and 4 weeks postoperatively, scores for food responsiveness and emotional overeating remained elevated. Compared to standard care, early reinitiators demonstrated a significant reduction in emotional overeating, food avoidance, hunger, food responsiveness and an increase in slowness in eating on the self-reported AEBQ at 3 and 6 months postoperatively (Fig. 3). At 6 months, mean differences between groups with 95% confidence intervals (Early reinitiators: n = 19; Standard care: n = 11) included: emotional overeating: −4.0 (95% CI: −4.0, −3.9), p < 0.001; food responsiveness: −3.4 (−4.0, −2.9), p < 0.001; hunger: −3.0 (−4.0, −3.0), p < 0.001). Mixed effect multivariate regression analysis, adjusting for baseline BMI, age, and sex, was conducted for each eating behavior sub-category captured on the AEBQ and revealed that early re-initiation significantly reduced food responsiveness, emotional overeating, and hunger at 3 and 6 months postoperatively compared to standard care (Table 5). At 6 months, mean differences between groups with 95% confidence intervals included: emotional overeating: −3.5 (95% CI: −4.38, −2.69), p < 0.001; food responsiveness: −2.7 (−3.45, −1.92), p < 0.001; hunger: −2.6 (−3.34, −1.87), p < 0.001; Table 5). No negative compensatory eating behaviors (restricting, purging, binge episodes) were reported during monthly visits with a registered dietitian. Additionally, 24-h dietary recalls showed that post-operative nutritional intake was adequate for age and weight, meeting all micro- and macronutrient requirements.
Fig. 3
Change in self-reported Adult Eating Behavior Questionnaire scores, completed by the youth participants between early obesity pharmacotherapy reinitiators (n = 25) vs. standard care (no obesity pharmacotherapy, n = 21) from a clinical sample
Table 5 Change in self-reported adult eating behavior questionnaire from baseline at 3 and 6 months postoperatively overtime between early obesity pharmacotherapy reinitiators and standard of care assessed utilizing a multivariate mixed-effects linear regression model controlling for baseline body mass index, age at time of consult, and sex in a clinical cohortSafety and TolerabilityNo significant differences were observed between the early reinitiation and standard care groups in rates of urgent care or emergency room visits (n = 4 vs. 3), unplanned readmissions (n = 2 vs. 3), or reoperations (n = 0 vs. 0) within 30-, 60-, or 90-days post-surgery. In the early reinitiation group, unplanned readmissions occurred for patient 1 (emesis and syncope on post-op day 40 after 1 dose of semaglutide 0.5 mg) and patient 2 (dehydration and poor oral intake intolerance on post-op day 88 after 4 doses of tirzepatide 2.5 mg weekly). In the standard care group, unplanned readmissions occurred for patient 1 (dehydration and poor oral intake intolerance on post-op day 7), patient 2 (constipation and dehydration on post-op day 47), and patient 3 (abdominal pain and cholecystitis on post-op day 95). Urgent care or emergency room visits in the early reinitiation group were for vomiting (post-op day 45, patient on phentermine 15 mg daily), constipation (post-op day 65, patient on metformin 1000 mg twice daily and phentermine 15 mg daily), and headache/vomiting (post-op day 76, patient on semaglutide 2.4 mg weekly). In the standard care group, visits were for vomiting (post-op day 27), constipation (post-op day 46), and nephrolithiasis (post-op day 85).
留言 (0)