Since Denny Brown and Robertson first described the phenomenon of DAC in UDS, a limited number of researchers have explored its clinical significance in the subsequent decades. While previous studies examined DAC expression in men with BOO, OAB, and women with LUTs, there are currently no specific studies addressing the characteristics and clinical significance of DAC in women with SUI. According to the ICS definition, SUI is characterized by the involuntary loss of urine during exercise, coughing, or sneezing [13]. Some studies suggest that 61% of patients with clinical symptoms of SUI exhibit USI, while others indicate that approximately 90% of SUI patients show positive UDS changes [14, 15]. However, guidelines underscore the importance of physical examination and history collection, noting that preoperative urodynamics may not significantly impact cure rates or complication rates for SUI patients [16, 17]. Presently, urodynamic parameters commonly used in the diagnosis of SUI include Abdominal Leak Point Pressure (ALPP) and Maximum Urethral Closure Pressure (MUCP). However, the current study highlights the limitations of these parameters, one study noted that the level of VLPP did not predict the success of outcomes after Burch or autologous fascia sling procedures [18]. Another study suggested that the range of MUCP values might be too restricted to detect meaningful differences in sphincteric health [19]. Consequently, there is currently no alternative urodynamic evaluation index for SUI.
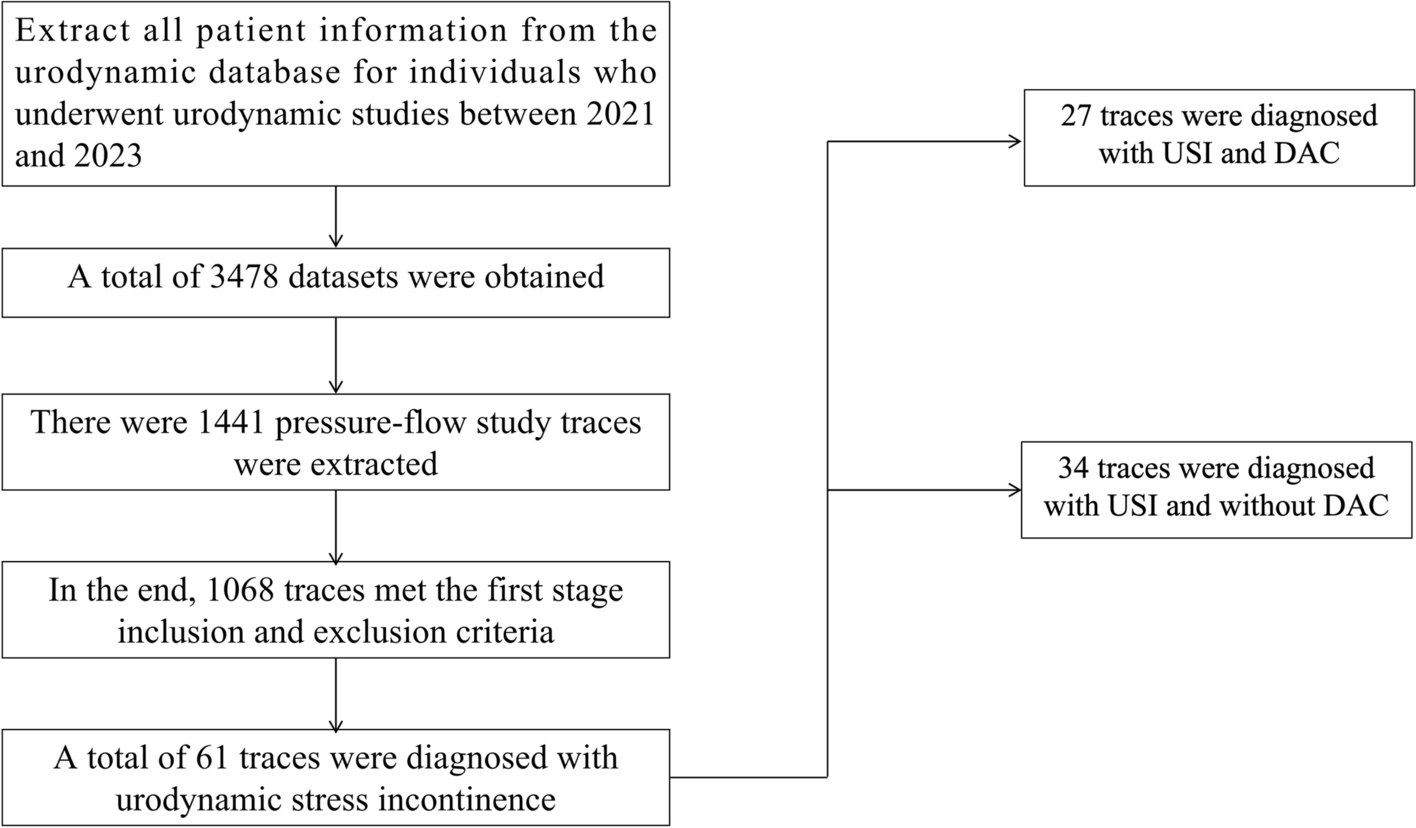
In a study focusing on the characteristics of DAC in males with BOO, a 12.5% incidence of DAC in females with USI was observed. Analyzing urodynamic traces from 1,068 patients in our study, we identified 27 cases representing a combination of USI and DAC and 44.3% (27/61) among all included USI patients. This incidence aligns with previous literature reports [6,7,8,9,10]. Intriguingly, our study revealed that DAC predominantly occurred in female patients with pure USI, deviating from previous findings associating DAC more with BOO and DO patients. Based on the two main hypotheses regarding the current mechanisms of DAC, the first suggests that it is may related to artifacts, while the second proposes that it is may associated with pathophysiological changes in bladder function [7, 8]. In this study, we implemented strict quality control procedures for UDS across all included samples, leading us to believe that the potential pathophysiological mechanism underlying DAC in pure USI patients is more likely aligned with the second hypothesis. However, the specific mechanism of its occurrence requires further in-depth research to explore. Then we compared the differences in classical parameters between the included patients with or without DAC with the urodynamic diagnosis of pure USI. Higher MCC values were found in the DAC group, At the same time, the DAC group had a more delayed onset of strong desire to void. One study suggested that the volume at which women leak first on urodynamic testing is not associated with outcomes, this study is the first to focus on the relationship between bladder volume and SUI, but it cannot explain our observed results well [19]. For the comparison of the parameters of the voiding phase, we found that the DAC group had higher Qmax and Pdetqmax. Previous studies on the Qmax have found that can be used to exclude bladder outflow obstruction or detrusor underactivity [5]. Qmax is a parameter of bladder function, At the same time, this index is a capacity dependent tolerance and individual difference index. One study also pointed out that women aged 65 years and older with SUI had significant decreases in Qmax, Pdetqmax [20]. Previous data showed that patients with DUA, after Middle urethral sling (MUS), had greater voiding dysfunctions than women without DUA, with no significant differences in SUI cure rates [21]. Larger Qmax and Pdetqmax was found in the DAC group, which may indicate better voiding function in the DAC group.
In a study published by Paulo Rodrigues on the occurrence of DAC in the adult female population, the observed DAC was divided into three subtypes based on morphological characteristics [11]. In a study on DAC in children, A.C. Ruarte also identified morphological characteristics of DAC and provided detailed descriptions [6]. Interestingly, in our study, we also found that the morphological characteristics of DAC in pure USI patients could also be divided into three subtypes, but the classification and morphological characteristics were different from those of Paulo Rodrigues. Nevertheless, our morphological classification aligns closely with A.C. Ruarte's description of the morphological characteristics of DAC in children. The morphological description of Type3 DAC in our study is similar to the description of Type1 DAC in Paulo Rodrigues' study, this type of DAC is often found after both the flow rate and the detrusor pressure had returned to zero, the incidence of Type3 DAC in our study was 22.2%, this type of DAC was observed in 7% of A.C. Ruarte's study.Type3 DAC exhibits a tendency toward longer uroflow times during the urination phase when compared with Type1 and Type2 DAC. The morphological description of Type1 DAC in our study is shown in the image as a sudden rapid rise curve in the middle and late stages of physiological detrusor contraction, the incidence was 48.2%, this type of DAC was observed in 36% of A.C. Ruarte's study. It often appears in the middle and back of the detrusor's physiological contraction curve. Simultaneously, Type 1 DAC displays a higher maximum contraction amplitude compared to other types. As with other studies on DAC, they often define DAC as a sudden curve rise after completing a urine stream or after a detrusor contraction. However, based on the graphical features we observed in female patients with pure USI, the majority of DAC did not manifest at the times described in previous studies on DAC in adult individuals.
The correlation analysis between DAC and traditional urodynamic parameters revealed a positive correlation between DAC time and total detrusor contraction time, as well as a positive correlation between the maximum DAC contraction amplitude and total detrusor contraction time. Additionally, there was a negative correlation between PVR before DAC and Qmax. Previous studies have been conducted on the index of detrusor contraction time, and the research results suggested that was correlated with symptom severity and urodynamic outlet obstruction in men, but the implications for female patients were not presented. At the same times, that detrusor contraction duration depends on several factors related to detrusor and outlet function [22]. Based on these results, DAC time and the maximum DAC contraction amplitude may be a potential indicator of detrusor contractility. However, further studies with larger sample sizes are needed.
This study has several limitations that merit acknowledgment. Firstly, the observed data were obtained from a single center. Despite a substantial sample size, regional and hospital-specific influences may introduce biases. Concurrently, the study's sample size might be constrained as current urogynecological guidelines do not recommend UDS for patients with pure SUI. Secondly, the morphological classification we employed may lack standardized criteria, and future research should focus on refining quantitative indicators for morphological classification.Thirdly, in China, where the authors are based, most medical institutions have transitioned from using WFS to ACS urodynamics equipment, therefore, the conclusions of this study need to be further validated and observed in the WFS. The potential of DAC-related parameters to predict prognosis requires further validation through large-sample, multi-center prospective studies.




留言 (0)