
記住我
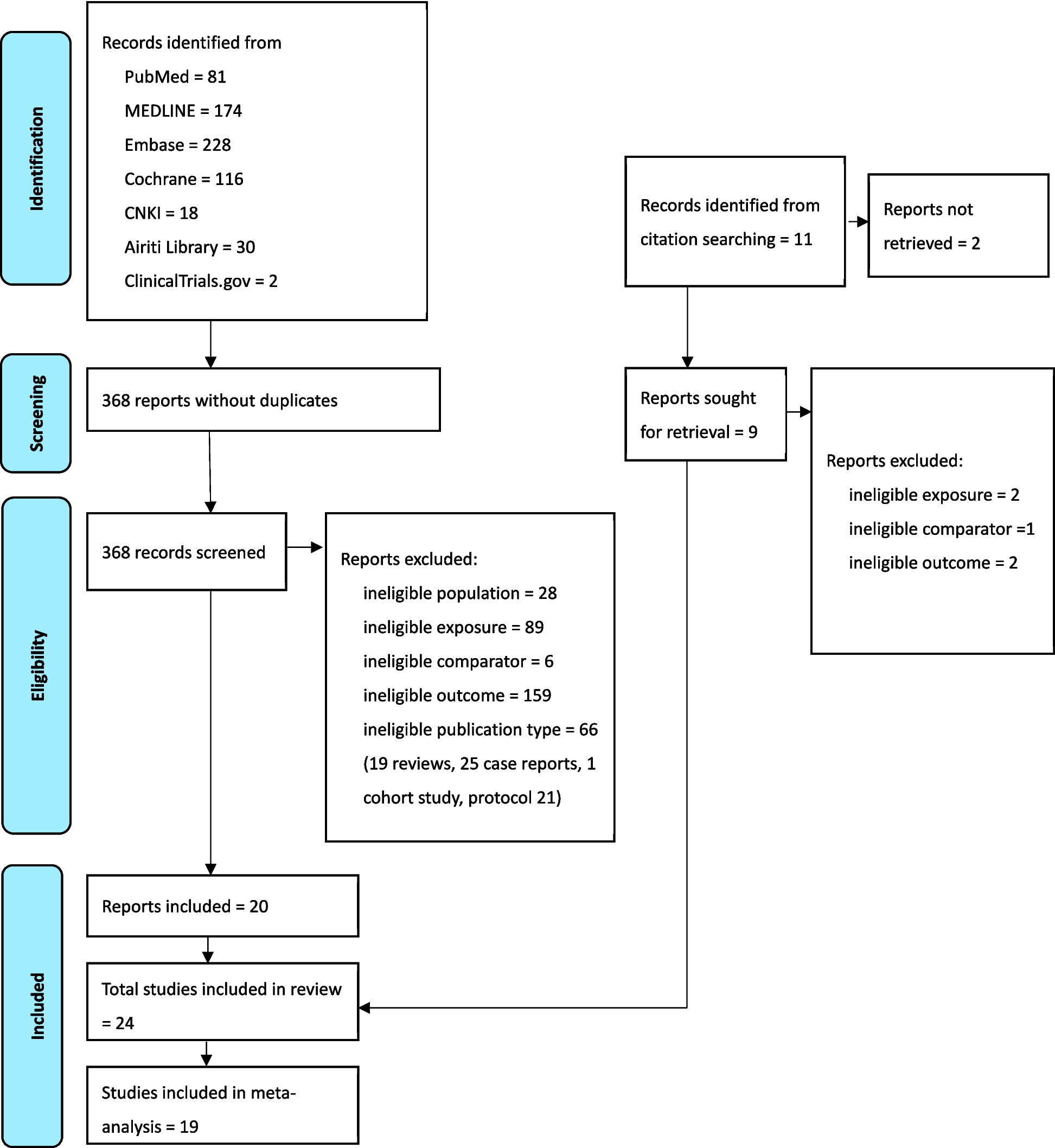
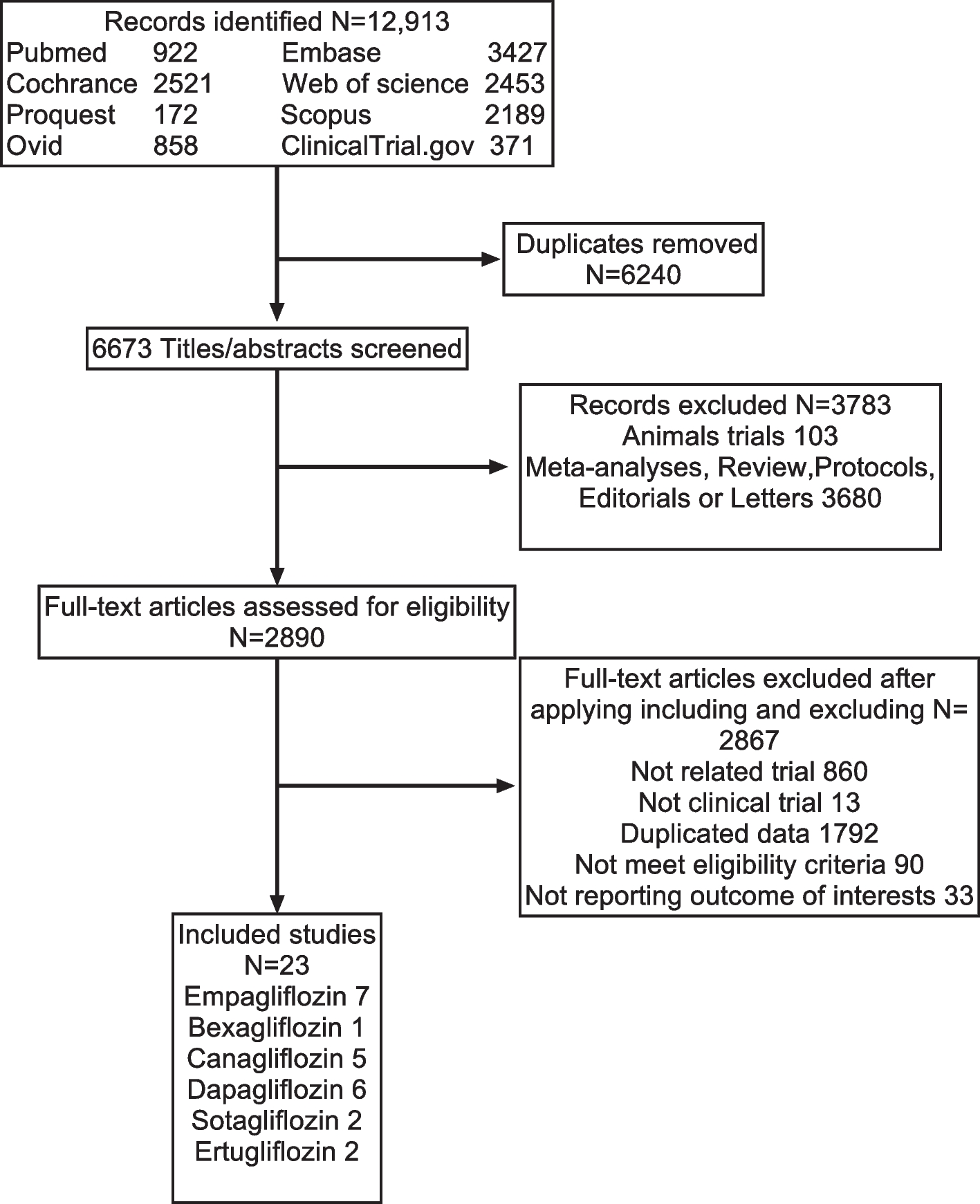

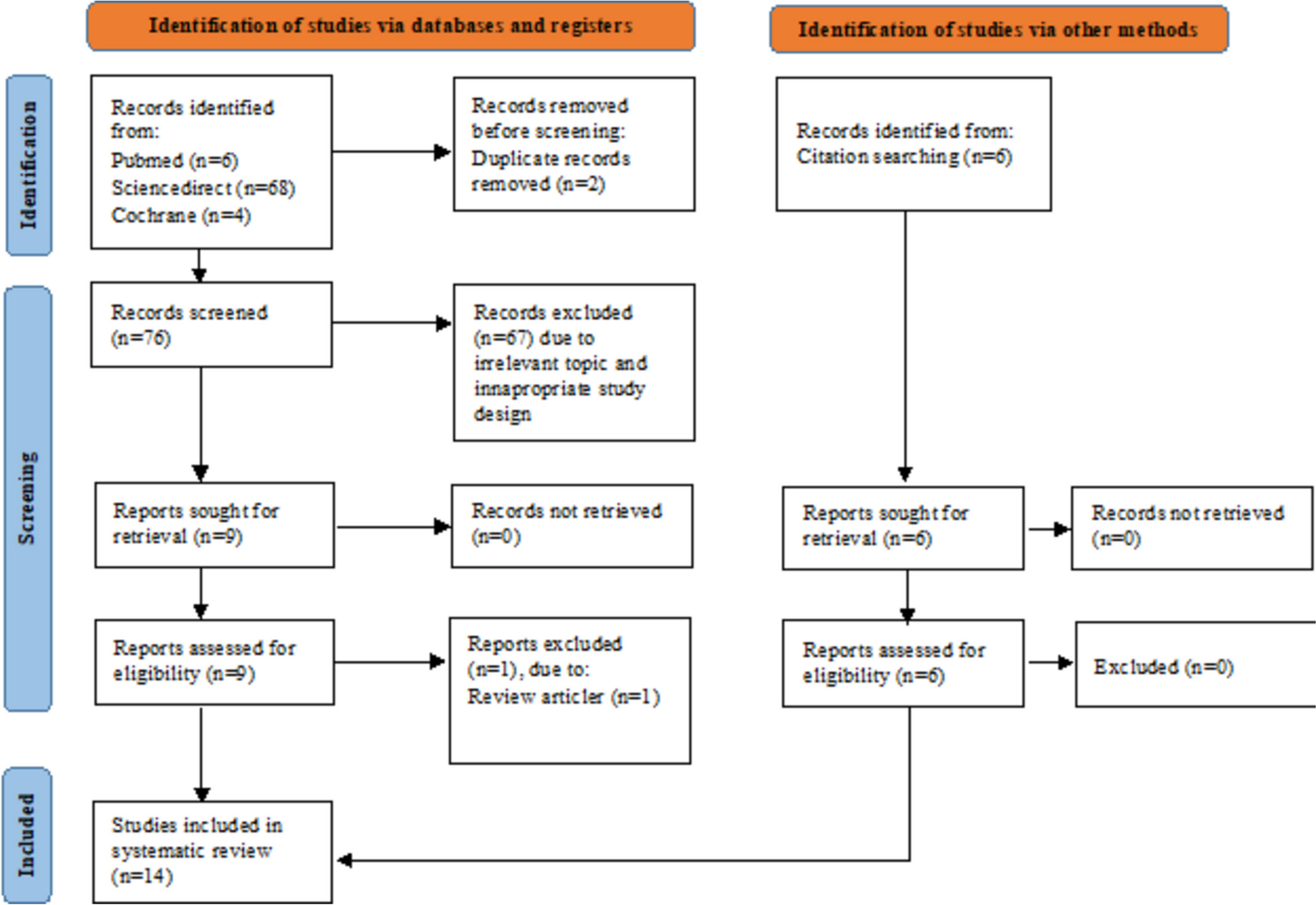

A total of 1067 titles were obtained, 1065 from searching of electronic databases and 2 titles from searching reference lists of eligible studies. After removing 568 duplicate titles, 499 titles were left for screening. The screening of titles and abstracts eliminated 487 titles leaving 12 titles for full-text assessment of eligibility. Full text of the 12 articles was obtained and printed out for thorough reading to assess eligibility, guided by the pre-set inclusion and exclusion criteria. At this stage, 3 articles were found ineligible. We therefore included 9 studies in the systematic review and none in the meta-analysis. Figure 1 below shows the study selection process.
Fig. 1 Description of included studiesStudy location and settings
Description of included studiesStudy location and settingsThree of the included studies were conducted in South Africa [23, 26, 28], two in Zimbabwe [24, 31], two in Kenya [27, 30], one in Ethiopia [25], and one in Malawi [29]. All studies were conducted within the community but in different settings. Four studies were conducted in homes of people living with HIV [25, 27, 28, 31], three in schools [23, 29, 30], and two in unspecified settings within the community [24, 26].
Study design and participantsStudies employed 3 different designs: a randomized controlled trial design was used in 5 studies [25, 27, 28, 30, 31], a pre-test and post-test design in three [23, 26, 29], and mixed methods in one [24]. Studies involved both male and female participants of various categories. People living with HIV (PLH) were involved in 6 studies [24,25,26, 28, 30, 31]. Among the 6 studies that involved PLH, 2 reported involving adolescents [30, 31]. Educators/teachers were involved in three studies [23, 29, 30].
Characteristics of included studiesIntervention characteristicsKey features of interventions are reported in 3 major themes that were developed during the analysis. These are described below.
Actors and sites of interventionsWe categorized actors in interventions as implementers and intervention recipients. Studies reported varying categories of individuals in both groups. In 4 studies [25, 28, 30, 31], the implementers were known to be living with HIV and thus acted as peer supporters/mentors [28, 31], community social workers [25], and volunteers [30]. In 4 studies, the HIV status of implementers was not explicitly stated [23, 24, 27, 29]. These included community members [27] and teachers [23, 29, 30]. In one study [26], PLH and those whose status was unknown were involved as intervention implementers.
Intervention recipients also varied across studies. Four studies focused exclusively on PLH [24, 25, 28, 31], while others included both PLH and individuals with unknown HIV status [26, 30]. Additionally, some studies targeted only individuals with unknown HIV status [23, 27, 29]. The study by Chindrawi et al. [26] involved PLH and people living close (PLC) to them. The PLCs were spouses/partners, children of PLH, family members, friends, religious leaders, and community members. In 3 studies [23, 29, 30], schoolteachers were the intervention recipients, while in another study [27], all consenting adults in households were targeted.
Although all included studies were categorized as community-based, they were conducted under different settings. Three studies were conducted in educational institutions, that is teacher training colleges [29] as well as primary and secondary schools [23, 30]. Four studies were conducted in households [25, 27, 28, 31], and 2 were not explicit on the exact settings within the community [24, 26].
Intervention processesInterventions reported in the included studies involved a variety of actions and interactions by the various actors described in the preceding theme. All interventions involved information sharing through different fora in the form of individual sessions or group sessions or both. In 2 studies, information sharing occurred through workshops and lectures [24, 26]. In one study [23], simulations of a person living with HIV were done through a digital platform using a compact disc read-only memory (CD-ROM) computer program and roleplay without direct contact with PLH. This was to build capacity of teachers to act as mentors and be able to address HIV-related issues within school and classroom settings. The study by Chidrawi et al. [26] involved workshops and lectures involving PLH and PLC to improve interactions between them, the understanding of HIV stigma, and the management of disclosure. Ferris France et al. [24] involved the intervention team working with PLH to address self-stigmatizing beliefs through face-to-face workshops, remote classes, and self-inquiry, as well as peer and mentor methods. In one school-based study [30], teachers underwent a multi-media HIV-stigma focused training.
Individualized counselling, health education, and other forms of social support including referrals to healthcare facilities for management of emerging health issues were reported in 5 studies [25, 27,28,29, 31]. The intervention by Lifson et al. [25] involved community social workers (CSW) who visited PLH and offered the intervention package, while for Low et al. [27], the same was delivered through the home-based counselling and testing program for all consenting adults. The intervention by Masquillier et al. [28] involved the provision of nutritional supplements during the visits to PLH, in addition to the counselling and other support. The one-on-one (friend-to-friend) intervention by Norr et al. [29] involved peer sessions covering various topics including HIV stigma. In the study by Willis et al. [31], community adolescent treatment supporters provided counselling to adolescents living with HIV in addition to monitoring their adherence to antiretroviral therapy and general well-being.
Cost and sustainability of interventionsStudies were not explicit on the cost of the interventions and how interventions would be sustained. We thus devised a framework to assess the cost of the interventions and their likelihood to be sustained by the community members. Four criteria were used to make judgement: number of people involved, level of motivation/incentive to engage in the intervention, and procurable tools used. Based on these, interventions were judged as low cost and sustainable, moderate cost and likely to be sustained, as well as high cost and unsustainable.
Interventions in three studies [25, 28, 31] were judged low cost and sustainable. These involved few individuals (PLH working with community social workers/peer adherence supporters/community adolescent treatment supporters) at household level. The one-on-one interaction would lead to a sense of accountability and individualized responsibility for continuity.
Four interventions [23, 24, 27, 30] were found to be of moderate cost and likely to be sustained. Costs were deduced from the purchase of computers/television sets and associated repairs for interactive digital media [23, 30], workshops for teachers in schools [24], and community-wide sensitization for home-based testing and counselling [27]. These also involved more people with the likelihood of self-propagation.
The intervention by Chindrawi et al. [
留言 (0)