
記住我
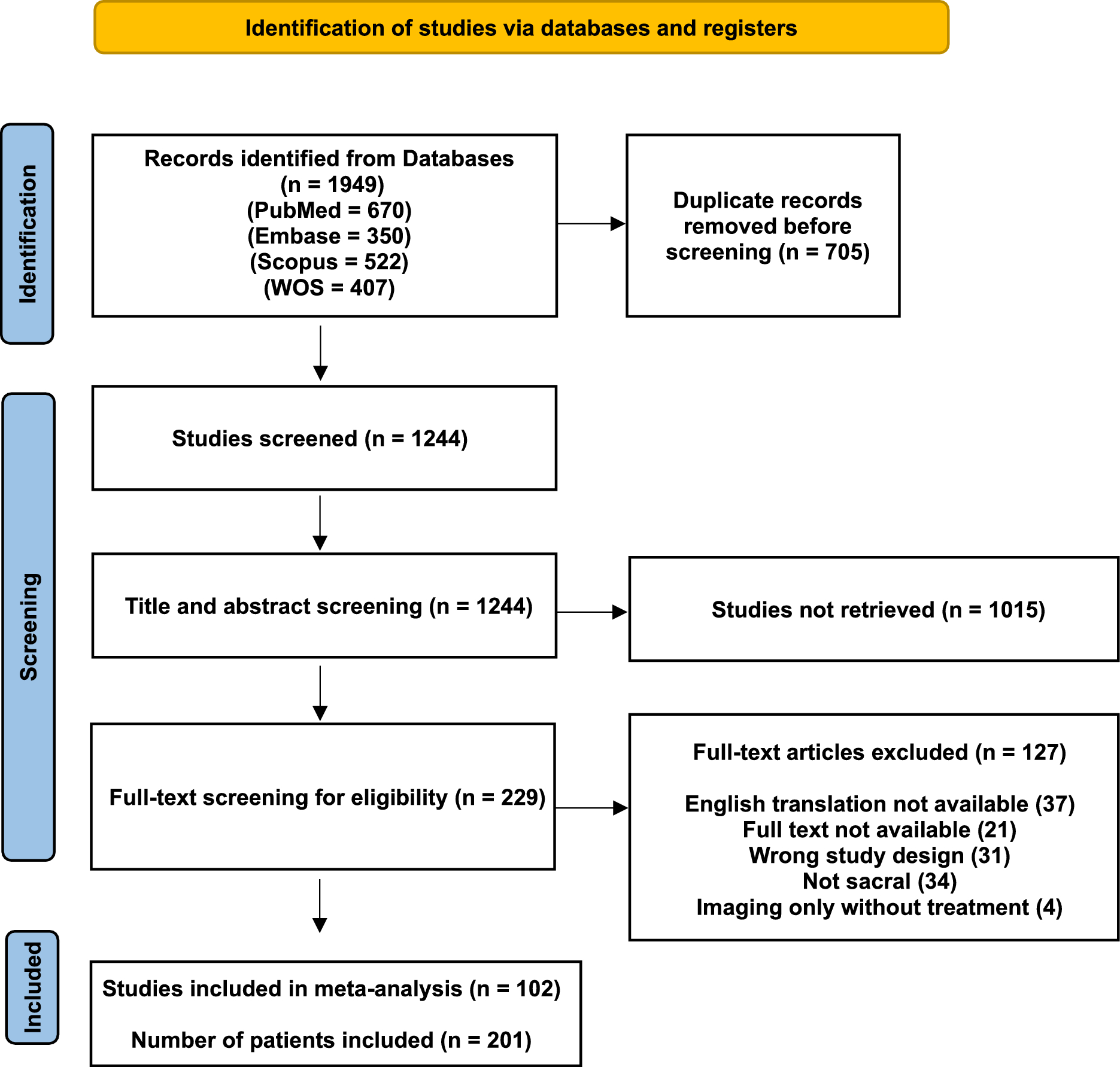


A cross-sectional study comparing ten standing imaging positions.
Recruitment of the participantsThirty females without scoliosis, 30 females with single AIS curves, 30 females with double AIS curves, and 10 males with AIS treated non-operatively were consecutively recruited from emailed ads, a specialized scoliosis clinic, and mailed letters. Thirty females with AIS had single and 30 had double curves. Complete tables of patient data is given in Online Resource 1. Inclusion criteria for participants without scoliosis included: able to stand unassisted for over five minutes, aged > 10 years old and without scoliosis (< 10°). Inclusion for AIS groups included: able to stand unassisted for over five minutes, aged 10 to 18 years old, treated non-operatively, and with curve angles > 10°. Spine or torso surgery, trauma, lower extremity conditions affecting posture, upper extremity conditions limiting movements or wounds affecting the back were excluded. Participants 18 years of age provided a signed informed consent. Participants below 18 provided assent and signed parental consent was obtained. This project was approved by the Health Research Ethics Board - Health Panel at University of Alberta (PRO00111881) .
Description of the participantsThe 30 females without scoliosis presented a mean age, height, and weight of 21 ± 4 years, 164 ± 5 cm, and 61 ± 10 kg, respectively. The 30 females with a single AIS curve presented a mean age, height, and weight of 15 ± 2 years, 160 ± 6 cm, and 52 ± 9 kg, respectively. The 30 females with AIS with a double curve presented a mean age, height, and weight of 14 ± 2 years, 161 ± 8 cm, and 52 ± 8 kg, respectively. After excluding one of 10 tested males participants due to discovering hyper-kyphosis (> 65°) during testing, nine males with AIS were included presenting a mean age, height, and weight of 16 ± 3 years, 173 ± 11 cm, and 63 ± 14 kg, respectively.
ProcedureDuring a 45-min assessment visit, participants were escorted from the parking to our lab where we conducted the informed consent procedures. Participants then changed, gel was applied to their back for each scan and they received the instructions to adopt each of our positions. Scanning equipment and our positioning frame was moved and readjusted to the participant’s characteristics as needed for each scan. Each scan was acquired in 20–30 s and saved in 30 s to a minute. A minimum of two scans were acquired in each of the 10 positions tested to ensure we had at least one good image to extract measurements. The participants were scanned twice using 3DUS in the 10 following standing positions in the following order: 1) habitual with arms down, 2) arms supported on bar anteriorly at 60° of shoulder flexion (local positioning), 3) fingers to clavicles, 4) to chin, 5) to zygomatic, 6) to eyebrows, 7) shoulders abducted 90° hands open with thumb on shoulder, 8) hands on wall, 9) on block, and 10) unsupported.(Table 1) In 8–10, hands are above the shoulders (possible maturity assessment).
Table 1 Patient Position and Corresponding Description for 10 Positions Used for 3DUS Scans3DUS image acquisitionThe evaluator instructed participants to adopt each position by demonstrating and stating the instructions in Table 1. A Sonix Q + system was used with a C5-2/60 convex curvilinear transducer. Acquisition parameters were as follows: scan frequency 2.5 MHz, gain 20%, reject 20, map 12, intensity 70db, frame rate 32 per second, clarity high, power 0, and time gain compensation used oblique two linear. Depth and focus were set (6-9 cm) to visualize the lamina. Scans were exported for off-line analysis using custom Matlab software (MIAS v10.3.26). The 3D volume images were obtained by registering the 2D ultrasound images in space based on the recorded position and orientation of the probe to position each pixel within the 3D volume. Intra-rater reliability for curve angles obtained using 3DUS has been very good (ICC(2,1) = 0.86–0.96) with a low standard error of measurement (≤ 2.5°) [19, 21]. Colleagues have completed previous validation work for curve angle measured in 20 adolescents with idiopathic scoliosis with curves between 10 and 45o imaged on the same day within 1 h with 3DUS and radiographs. All US images were measured blinded to the radiographs by 2 novice researchers with under a year of previous experience in scoliosis research. Results showed that 3DUS curve angles correspond to radiographs with an inter-method standard error of measurement ≤ 3.4° [19].
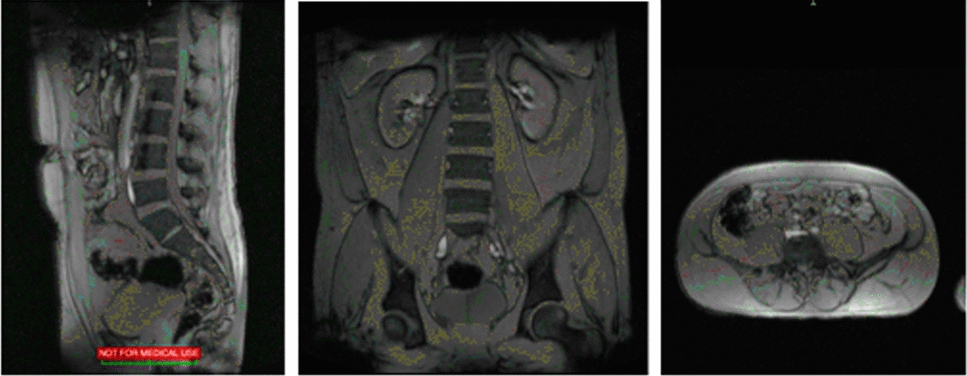
Image analysisFrontal parametersUsing MIAS, the center of the lamina (COL) on the right and left side of each vertebra was manually digitized on the coronal image. The curve angle was the angle between the most tilted laminas above and below the apex for each curve (Fig. 1a). The depth of the lamina was verified on the transverse view (Fig. 1b).
Fig. 1
Laminae, spinous process column, skin, subcutaneous fat and transverse processes in an ultrasound image: a Coronal plane and b Transverse plane. (L) = Left, (R) = Right
Transverse parametersAVR was automatically determined between the line going through the COLs and a horizontal reference (Fig. 1b). The apex of all curves was determined by choosing the lamina that was most lateral from the midline in the frontal projection view of the 3D reconstructed US image. AVR was extracted at, above and below the apex for all curves. To determine AVR Twist, first take the average of the AVR’s measured above, at, and below the apex of the curve that deviates laterally to the right ((AVR above + AVR at + AVR below the curve apex most rotated to the right) /3). Then follow the same process to find the average AVR for the most rotated laminae to the left ((AVR above + AVR at + AVR below the curve apex most rotated to the left) /3) [22]. Then, you take the difference between these two averages to find the AVR Twist (Mean AVR for the curve rotated to the right – Mean AVR for the curve rotated to the left). High accuracy for AVR measurements was demonstrated in a cadaveric study (mean absolute difference < 1.7°) [18]. High intra-rater reliability has also been observed in-vivo for AVR measurements (ICC(2,1) > 0.95, mean absolute difference < 0.7 ± 0.7°) [17].
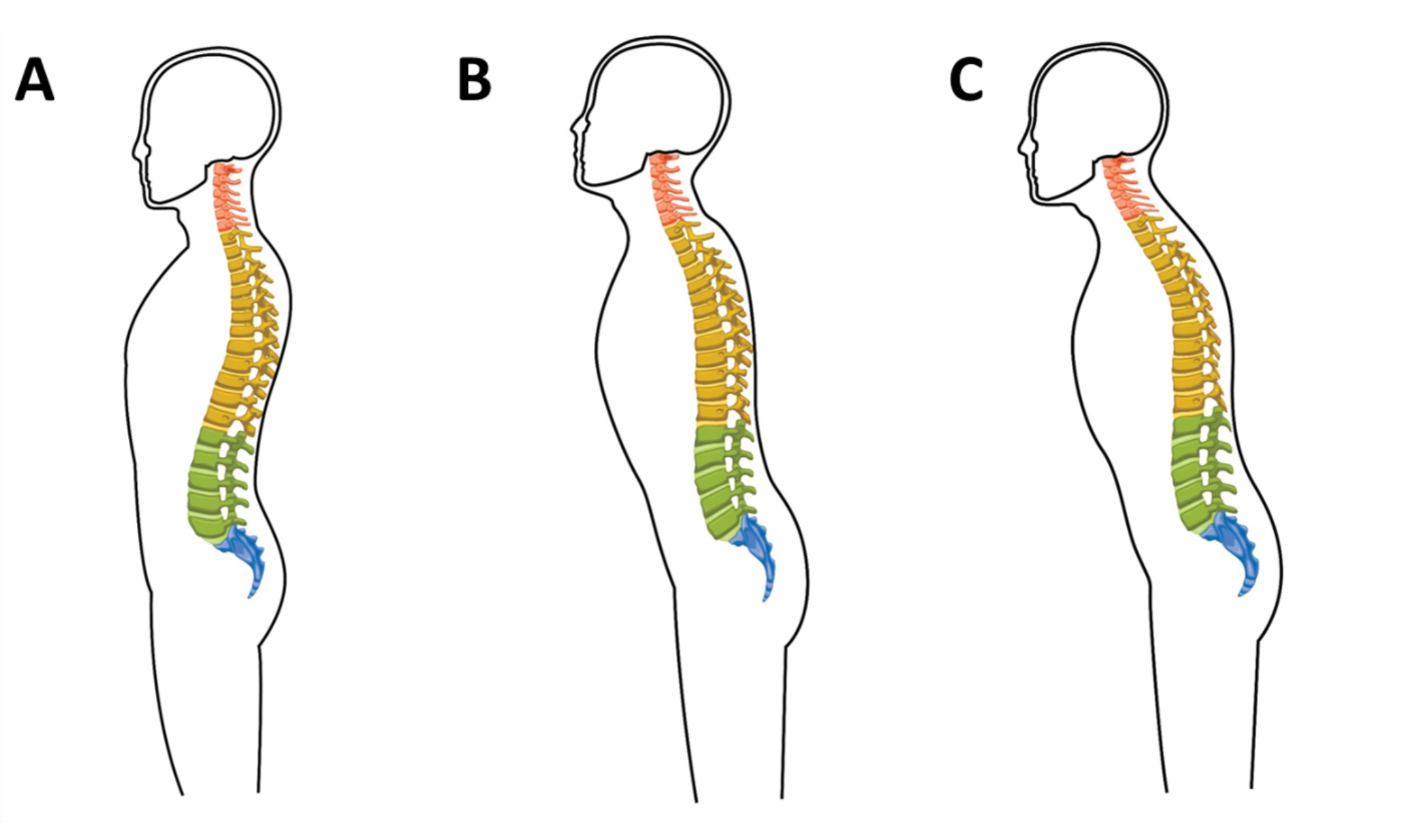
Sagittal parametersLines connected the mid-points of the lamina of T1-T2 and T11-T12 in the sagittal view to form a whole kyphosis angle. T4-T5 and T11-T12 were also connected to form a T4/T5–T11/T12 kyphosis angle (Fig. 2a,b).
Fig. 2
Sagittal curvature measurements and vertebral segments (a) Whole Thoracic Kyphosis and Lordosis angles (b) T4-T5 kyphosis angle. Ant = Anterior, Post = Posterior
Similarly, the mid-points of L1-L2 and L4-L5 were connected to measure lordosis. On images where T1 did not show clearly, the T2-T3 pair was used to calculate whole kyphosis angle [habitual standing (10 instances), arms 60° (7 instances), fingers to clavicles (14 instances), chin (11 instances), zygomatic (11 instances), eyebrows (10 instances), shoulders abducted 90° (10 instances), hands on wall (11 instances), on block (9 instances), and unsupported (15 instances)]. US kyphosis and lordosis are also reliable [23].
Statistical analysisSeparate mixed-model ANOVAs compared the 10 arm positions and the three female groups (without scoliosis, with single curves or double curves) for each alignment parameter. Sidak post-hoc pairwise comparisons were used to compare each position against habitual standing. Separate repeated measures ANOVA compared the 10 positions in males. Pairwise comparisons for the interaction were examined by determining if the compared mean fell within the 95%CI of other positions. Statistical significance was set to 0.05.
Sample sizeThree groups of 30 participants tested in 10 positions achieves a power of 80% with alpha at 0.05 to detect a moderate effect size (f = 0.107) for positions, assuming a r = 0.5 correlation between repeated measures. This sample also achieves 80% power to detect a 5° ± 7° difference using a significance level of 0.005 adjusted for multiple comparisons between each position and habitual standing.
留言 (0)