
記住我





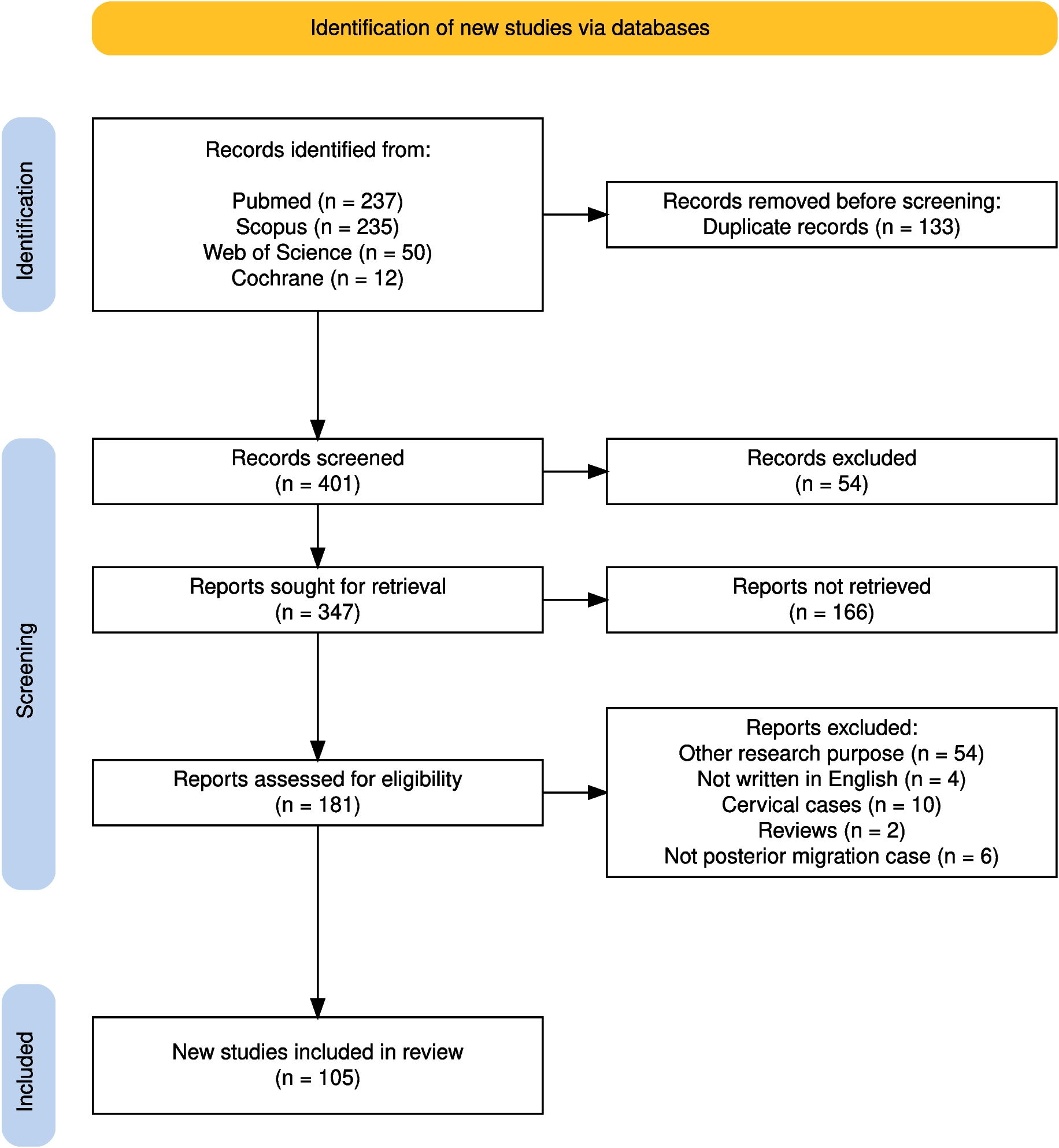
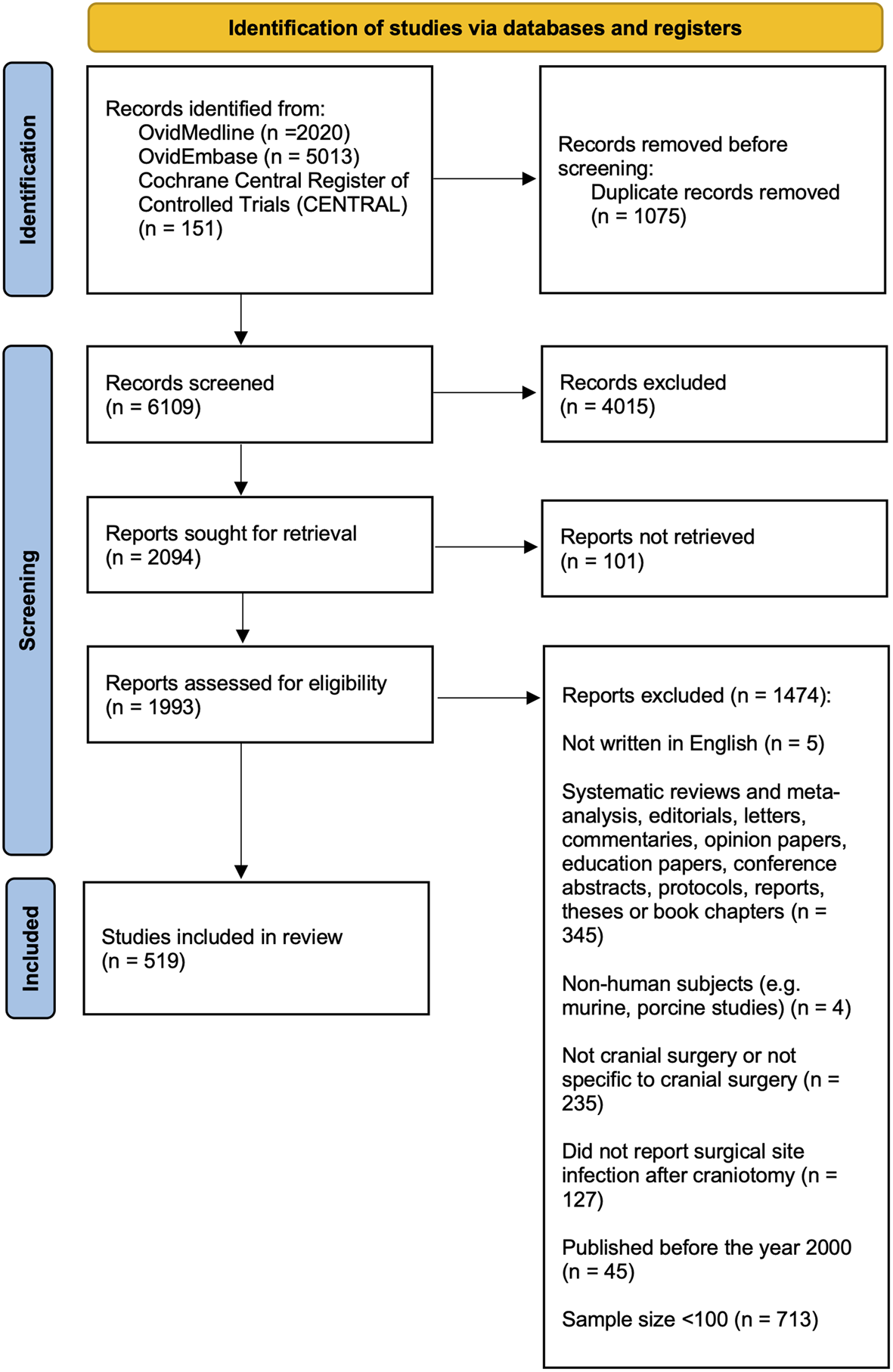
The study included 240 patients who underwent neuroendoscopic procedures between 2017 and 2023. After excluding 8 cases with missing data, 25 patients with postoperative infections (e.g., CSF infections, pneumonia, cystitis) during the first seven postoperative days were also excluded. This left 207 patients with complete data, including 104 (50.2%) who underwent endoscopic third ventriculostomy (ETV) and 103 (49.8%) who underwent other neuroendoscopic procedures. The cohort was further divided into pediatric and adult groups, with 58 pediatric and 46 adult ETV cases, and 79 pediatric and 24 adult non-ETV cases. Figure 2, presented as a flowchart, outlines the steps for inclusion and exclusion in the study.
Fig. 2
Flow diagram illustrating the process of inclusion and exclusion of the study cohort
Patients’ characteristics and intergroups’ comparison, ETV vs. non-ETVThe study included a total of 207 patients, with 104 (50.2%) undergoing endoscopic third ventriculostomy (ETV) and 103 (48.8%) undergoing other neuroendoscopic procedures without ETV. The gender distribution showed 105 males (50.7%) and 102 females (49.3%), with no significant difference between the ETV and non-ETV groups (p = 0.127), the mean age of patients was 19.1 ± 21.7 years, with those in the ETV group being significantly older (23.1 ± 23.4 years) compared to the non-ETV group (15.0 ± 19.1 years, p = 0.007). Pediatric patients comprised 66.2% of the total cohort, with a higher proportion in the non-ETV group (76.7%) compared to the ETV group (55.8%). The mean follow-up duration was longer in the ETV group (34.9 ± 23.3 months) than in the non-ETV group (27.9 ± 21.8 months, p = 0.026), Table 1.
Surgical duration was significantly shorter in the ETV group (68.9 ± 47.9 min) compared to the non-ETV group (86.8 ± 42.5 min, p = 0.005). Patients in the ETV group had a shorter ICU stay (0.7 ± 1.6 days) compared to the non-ETV group (2.0 ± 4.4 days, p = 0.005), the most common etiologies were arachnoid and ependymal cysts (26.1%), intraventricular tumors (25.1%), idiopathic aqueductal stenosis (25.6%), and posthemorrhagic hydrocephalus (17.9%). ETV was more frequently performed in patients with idiopathic aqueductal stenosis (42.3%) and intraventricular tumors (32.7%, p < 0.001), Table 1.
Postoperative clinical improvement was seen in 85.5% of patients, with no significant difference between the ETV (87.5%) and non-ETV (83.4%) groups (p = 0.437). Radiological improvement was observed in 83.6% of patients, again with no significant difference between the groups (p = 0.459). Postoperative hygromas occurred in 6.8% of cases, with no significant difference between the groups (p = 0.284). Laboratory analysis of cerebrospinal fluid (CSF) showed no significant differences in protein, lactate, or leukocyte content between groups, but glucose levels were higher in the ETV group (p = 0.001), Table 1.
Table 1 Patient’s characteristics und comparison between ETV- and Non-ETVComparison of body temperaturePostoperative body temperature elevation (above 37.5 °C) occurred more frequently in the ETV group (71.2%) compared to the non-ETV group (50.5%, p = 0.003). Fever (≥ 38.3 °C) was more common in the ETV group (37.5%) compared to the non-ETV group (19.4%, p = 0.005), though the rates of subfebrile temperatures (37.5–38.29 °C) were not significantly different between the groups (p = 0.767), Table 1.
Figure 3 presents a comparison of fever incidence between the ETV and non-ETV groups over a 7-day postoperative period, with body temperatures recorded during day and night. In the non-ETV group, fever was rare, starting in 8.3% on Night 0, peaking in 9.8% on Day 1, and then declining gradually to 0% by Day 7. In contrast, the ETV group had a much higher and more variable incidence of fever, beginning in 4.2% on Day 0, peaking in 26.9% on Night 0, and fluctuating throughout the week. Fever incidence in the ETV group also experienced notable increases on Days 4 and 7, with 11.1% recorded during those nights.
Fig. 3
Comparison of fever incidence between the ETV and non-ETV groups over a 7-day postoperative period
Sub-analysis in pediatric patients with intragroup compression between ETV and non-ETVThe study included 137 pediatric patients, with 58 (42.3%) undergoing endoscopic third ventriculostomy (ETV) and 79 (57.7%) undergoing non-ETV neuroendoscopic procedures. Postoperative body temperature elevation (above 37.5 °C) was significantly more frequent in the ETV group, occurring in 87.9% of patients, compared to 51.9% in the non-ETV group (p < 0.001). Fever (above 38.3 °C) was also notably higher in the ETV group, affecting 53.5% of patients, whereas only 21.5% of the non-ETV patients experienced fever (p < 0.001). However, the rate of subfebrile temperature (37.5–38.2 °C) was not significantly different between the groups (p = 0.712).
The study also found that the ETV group had a shorter ICU stay (0.7 ± 1.4 days) compared to the non-ETV group (2.2 ± 4.7 days, p = 0.007), while the surgery duration, age, and follow-up periods showed no significant differences. Surgical complications were more common in the ETV group (8.6% vs. 1.3%), although this difference was not statistically significant (p = 0.083). for more details see Table 2.
Table 2 Pediatric Patient’s characteristics und comparison between ETV- and Non-ETVFigure 4 illustrates the incidence of subfever and fever in the ETV group over a 7-day postoperative period, with body temperatures measured both during the day and night. Subfever was consistently present, beginning in 15% on Day 0 and persisting throughout the 7 days, with peaks around 40% on Nights 3, 5, and 7. In contrast, fever showed a more variable pattern, peaking in 26.9% on Night 0 and fluctuating throughout the week before subsiding after Day 4.
Fig. 4
Postoperative Body temperature elevation in Children with ETV
Sub-analysis in adult patients with intragroup compression between ETV and non-ETVTable 3 summarizes the characteristics and outcomes of 70 adults’ cases, with 46 (65.7%) undergoing ETV and 24 (34.3%) non-ETV procedures. The groups were similar in age (p = 0.915) and sex distribution (p = 0.081). ETV patients had a significantly longer follow-up (mean 31.9 vs. 19.1 months, p = 0.015) and shorter surgery duration (54.5 vs. 83.7 min, p = 0.001), while ICU stays showed no significant difference (p = 0.508).
Postoperative temperature elevations were recorded in both groups, with body temperatures > 37.5 °C observed in 51.4% of cases, with 50.0% in the ETV group and 45.8% in the non-ETV group (p = 0.804). Specifically, subfebrile temperatures were noted in 32.9% (32.6% in the ETV and 33.3% in the non-ETV group, p = 0.737), and postoperative Fever (> 38.2 °C) was observed in 15.7% of cases, with a slightly higher occurrence in the ETV group (17.4%) compared to the non-ETV group (12.5%) (p = 0.737).
Adverse events remained low, with surgical adverse events in 4.3% of cases (p = 1.0) and non-surgical adverse events also in 4.3% (p = 0.269). Clinical improvement was observed in 82.9% of cases and radiological improvement in 85.5%, with no significant difference between ETV and non-ETV groups.
Table 3 Adult Patient’s characteristics und comparison between ETV- and Non-ETVOccurrence of fever in relation to age and type of endoscopic procedureFinally, upon categorizing the patients in 3 groups according to age; <18 or ≥ 18 years and presence or absence of ETV as endoscopic procedure (see Table 4), we found in group 1, including adults without ETV, fever was present in 3/24 patients (12.5%). In group 2, including adults with ETV and children without ETV, fever was present in 25/125 (20%). In group 3, including children with ETV, fever was present in 31/58 (53%).
Table 4 Points distribution and patients’ groups
留言 (0)