As oncological control for cT1a SRMs becomes more comparable between PN and thermal ablative measures, maintaining kidney function and preventing the morbidity of CKD becomes increasingly important. Many studies have shown that MWA can achieve excellent cancer control and is especially suited for patients who are high-risk for surgical complications [4,5,6]. With the low renal reserve of SK patients, avoiding renal ischemia time and achieving cancer control is the ideal balance.
We found that at 12 months post-MWA, most patients experienced a decrease in eGFR. For those with follow up at 12 months, 50% had CKD upstaging. There was a significant difference in pre-op eGFR compared to 12 months (median 52 and 40, p = 0.0051). Two other studies have looked at MWA in SK with cT1a SRM. Meng et al. found no significant difference in creatinine for 16 patients when comparing pre-op, 1 day post-op, and 24 months post-op [7]. Their median pre-op and 24-month creatinine was 1.06 µmol/L and 1.08 µmol/L, respectively. Lin et al. also reported that there was no significant change from pre-op (1.11 Cr) compared to most recent follow up at approximately 9.3 months [4]. Our median pre-op and 12-month creatinine was 1.3 and 1.6, which also showed no significant difference (p = 0.11). However, eGFR is much more sensitive to change as it takes into account patient characteristics [11]. Our patients had worse kidney function at presentation, which has been shown to be a predictor for further worsening kidney disease [12].
More broadly, it is unclear if these findings generalize to patients with two functional kidneys because few studies directly compare SK and 2-kidney patients. Our renal function findings are similar to a prior study by Qiu et al. analyzing a different cohort from the same database. Comparing eGFR at 6 months post-op vs. pre-op, our cohort had a median eGFR change of 6 (Fig. 2B) compared to an eGFR change of 5 for patients with 2 kidneys [13]. Furthermore, Ibrahim et al. found that there was no difference in renal outcomes between SK patients and age and sex-controlled patients with 2 kidneys, however, the 2 groups had different baseline comorbidities [14].
Our studies reported similar rates of CSS at 1, 2, and 3 years post-op compared to Meng et al [7]. However, their study reported no local recurrence, contrasted to our rate of 15.4% local recurrence. Furthermore, they had better OS rates at 1, 2, and 3 years post-op (100%, 93.3%, and 93.3%, respectively) compared to ours (92.3%, 84.6%, and 76.9%). The higher local and metastatic recurrence could be due to our median mass size being larger at 2.6 cm (2.2–3.1) compared to theirs at 2.1 cm (1.7–2.8), which has been shown to be correlated to recurrence in patients with nonmetastatic RCCs ≤ 4 cm [15]. Furthermore, a study by Guan et al. on patients with SK receiving MWA or PN observed similar 3-year CSS and OS rates (90.4% and 91.3%, respectively) compared to our study (92.3% and 76.9%), with our cohort again having a lower OS rate [16]. Furthermore, our 6 month, 12 month, and 36 months LRFS rates (100%, 100%, and 88.5%) were similar to a prior study on the same cohort with the majority of patients having 2 kidneys with 3–4 cm RCC (100%, 100%, and 94.5%) [13].
Our oncologic findings are comparable to studies using other ablative techniques. In a study by Xiaobing et al. comparing RFA and PN in SK with RCC, the local recurrence rate of RFA was 18.75%, similar to ours at 15.4% [17]. However, they reported a lower metastasis rate of 6.3%, compared to the 19.2% observed in our cohort. A meta-analysis conducted by Liu et al. compared the safety and efficacy of CA and PN in SK patients [18]. When looking at local and metastatic recurrence rates of CA, Liu et al. observed a local recurrence rate of 14.6% and a metastatic recurrence rate of 9.7%, compared to ours (15.4% and 19.2% respectively), with our study having a higher metastatic recurrence rate.
One explanation for our lower OS rate is that our cohort had a median CCI index of 5, which suggests a high baseline comorbidity risk. The most likely source of discrepancy in metastatic recurrence outcomes is patient selection, tumor characteristics, and duration of follow up. Our study, in conjunction with Xiaobing et al. and Liu et al.’s findings, highlights the need for further research to demonstrate these differences and broaden the potential therapeutic options for managing RCC and its associated metastatic recurrence in this high-risk patient population [17, 18].
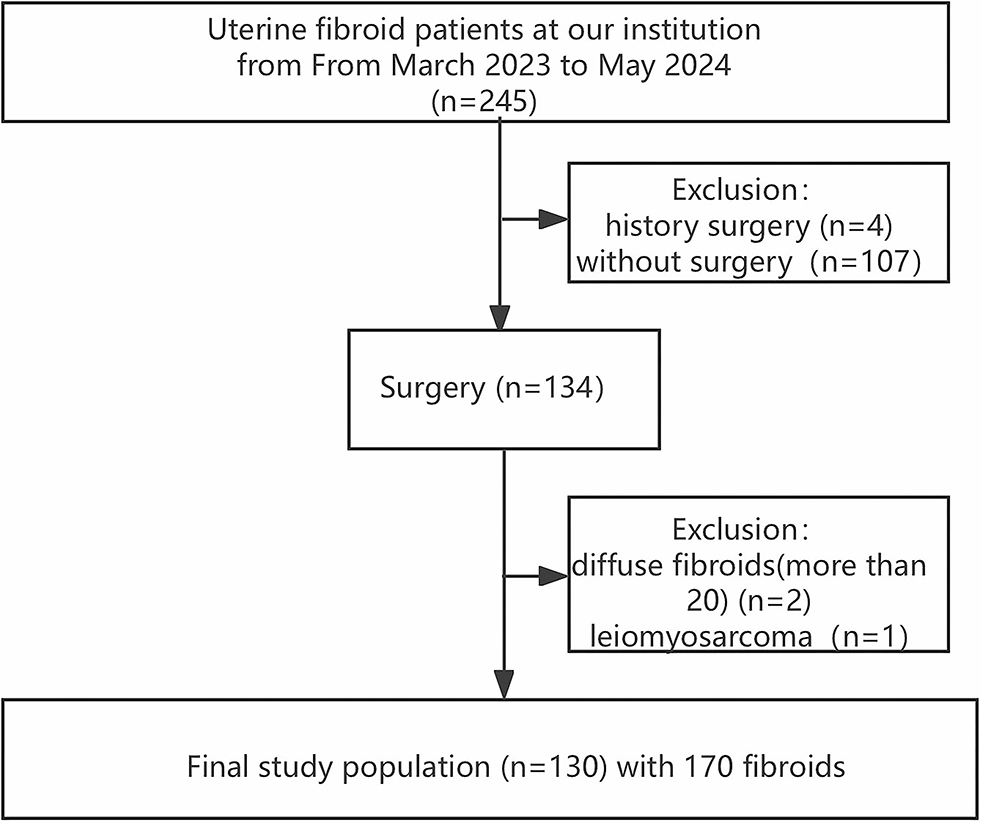
This study is limited by the small cohort of only 26 individuals. There were three congenital SK patients included, and this may skew our results. Prior work has shown that congenital SK, but not acquired SK, can undergo compensatory hypertrophy, which could lead to differences in eGFR over time [19, 20]. Reliability of our findings is also limited by the variability in patient follow-up adherence. As such, we cannot fully assess whether MWA contributes to sustained renal function preservation or if further decline may occur beyond the 12-month period. Future research with extended follow-up durations and comparison to our gold standard of PN is necessary to demonstrate these long-term outcomes and to provide a more comprehensive understanding of how MWA affects SK patients.






留言 (0)