
記住我
This retrospective study was conducted at Tinaztepe University Galen Hospital and Egesehir Hospital between January 2023 and December 2023; patients who underwent LSG were divided into two groups based on the method of liver retraction used. We retrospectively analyzed data collected prospectively from the patient populations in which we applied these two methods. Our clinical practice has routinely used the NR for liver retraction in LSG until May 2023. However, we hypothesized that we could get the needed retraction with a combination of a SurG and positional changes. Since June 2023, we have been using the SurG technique for retraction of the liver. Inclusion criteria for the study were patients over the age of 18 with complete data who provided informed consent. Exclusion criteria included patients with missing data, who underwent other bariatric procedures and those under 18 years of age. This study was conducted in full compliance with the ethical standards and protocols approved by the Ethics Committee of the tertiary health institution (1764.1784).
Study GroupsPatients were divided into two groups according to the method of liver retraction used during LSG. One group underwent liver retraction using the NR, while the other group utilized SurG for liver retraction. Both groups were compared for postoperative outcomes, including pain levels, liver enzyme changes, and recovery. Both groups followed Enhanced Recovery After Surgery (ERAS) protocols.
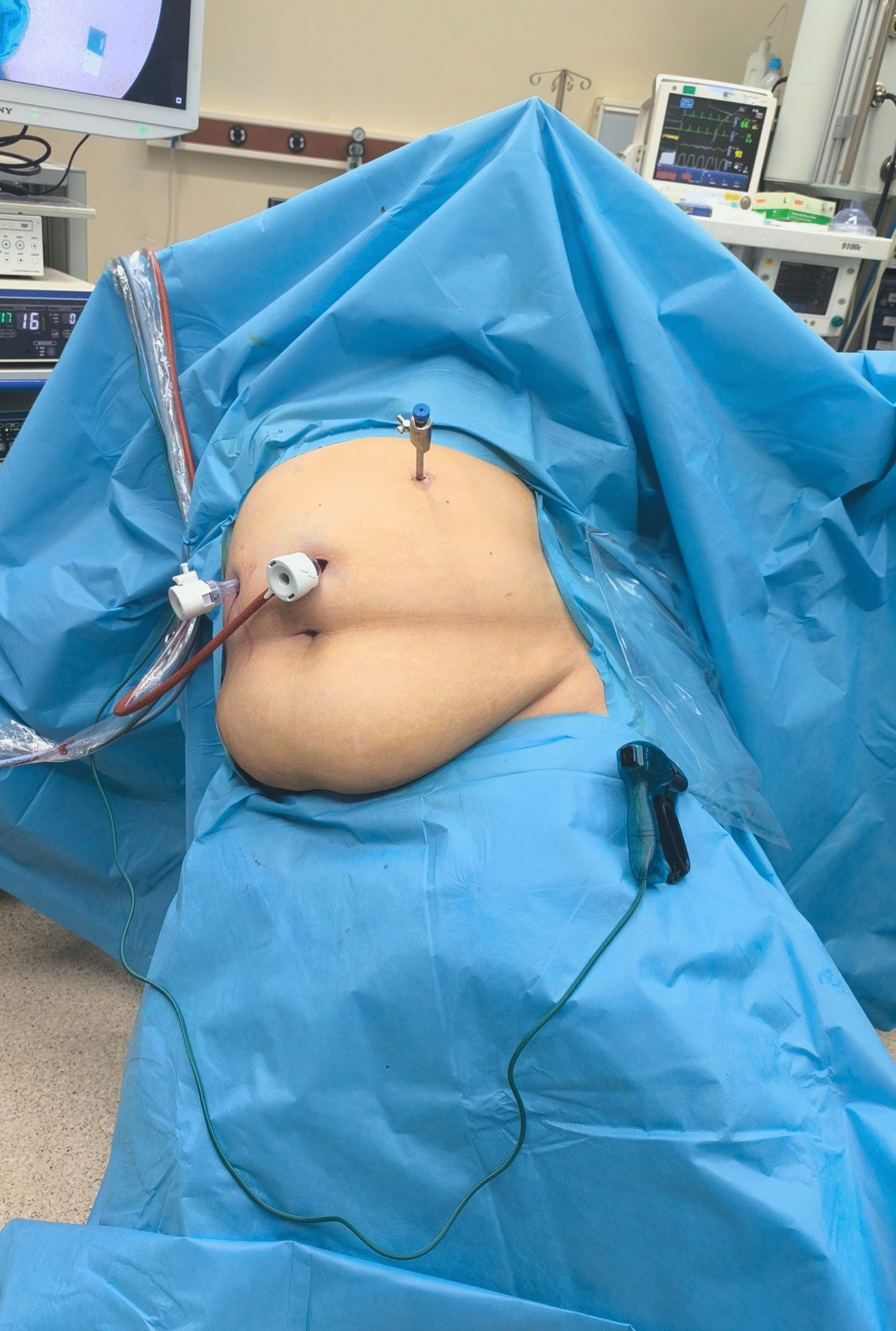
Surgical TechniqueAll patients were evaluated preoperatively with gastroscopy. Sleeve gastrectomy procedures were performed using a laparoscopic approach. Initially, trocars were placed in the abdominal region. In our clinical practice, for the first trocar entry, the camera port is placed 10–12 cm below the xiphoid process and to the left of the midline. After the incision, dissection is performed with a finger down to the fascia. The fascia is held with two towel clamps, and after insufflation of the abdomen with a Veress needle, a 12-mm trocar is inserted. In the three-port technique, a 10-mm trocar was inserted above the umbilicus, a 12-mm trocar in the right upper quadrant, and a 5-mm trocar in the left upper quadrant. After obtaining an adequate view of the abdominal cavity, the patient was placed in a reverse Trendelenburg and right-tilted lateral decubitus position. This position helps rotate the liver to the right, improving the visibility of the surgical field (Fig. 1). Then, a long surgical gauze was shaped into a ball and placed between the liver and stomach, approximately 2 cm away from the hiatus, to retract the liver (Fig. 2). The gauze is inserted through a 12-mm trocar and then shaped into a ball.
Fig. 1
Patient positioned in reverse Trendelenburg and right-tilted lateral decubitus position to enhance liver rotation and improve surgical field visibility
Fig. 2
Stapling phase: surgical field and retraction with long gauze
In the four-port technique, an additional 5-mm trocar was inserted in the subxiphoid area, and the Nathanson retractor was used for liver retraction. In both techniques, the operative view scoring system, ranging from 1 to 5, was used to evaluate the visualization of the gastroesophageal junction (GEJ), angle of His, lesser curvature (LC), and greater curvature (GC), with 1 representing the poorest view and 5 representing optimal visibility [9].
In both methods, the intra-abdominal manipulations proceeded similarly, and the stomach was carefully resected using staplers. Along the staple line, continuous sutures were placed using 3/0 absorbable barbed sutures to secure the staple line (Fig. 3). The fascia of the trocar site and camera port, where the stomach was extracted, was closed using an endoscopic fascia closure device.
Fig. 3
Retraction with long surgical gauze and reinforcement of the staple line with sutures
Data CollectionData collected included demographic details, body mass ındex (BMI), hepatosteatosis (assessed by ultrasound), comorbidities (diseases), abdominal operation history, duration of surgery, staple line leaks, staple line bleeding, deep tissue infections, deep vein thrombosis, instances of liver laceration, trocar-induced hemorrhage, subxiphoid trocar site infections, and liver enzyme levels both preoperatively and at 24 and 48 h postoperatively. The enzymes measured were aspartate transaminase (AST) with normal levels of 1–35 U/L, alanine transaminase (ALT) with normal levels of 1–34 U/L, C-reactive protein (CRP) with normal levels up to 5.0 mg/L, alkaline phosphatase (ALP) with normal levels between 40 and 130 IU/L, and gamma-glutamyl transferase (GGT) with normal levels between 5 and 45 U/L. The analysis was conducted with reference to established normal ranges for each enzyme. The length of hospital stay was also assessed for both groups to determine the average hospitalization duration. Pain levels were evaluated using the Visual Analog Scale (VAS) at various time points, including preoperatively, and at 6, 12, 24, and 48 h postoperatively, as well as on the 10th postoperative day. VAS scores, surgical hematomas, bleeding, and postoperative nausea and vomiting (PONV) are routinely evaluated independently of the surgical procedure. These parameters are systematically assessed for every surgery by clinical ward and outpatient clinic nurses and are documented in patient records.
Statistical AnalysisBaseline clinical data were analyzed using the t-test or Mann–Whitney U test for continuous variables and the Fisher’s exact test or chi-square test for categorical variables. SPSS version 22.0 (SPSS Inc., Chicago, IL, USA) was used for data analysis. Descriptive statistics (mean, standard deviation, median, frequency, percentage, minimum, maximum) were applied to evaluate the data. The one-way ANOVA test was used to compare normally distributed quantitative variables between the groups. A p-value of less than 0.05 was considered statistically significant.
Outcome MeasuresPrimary OutcomesThe main endpoints of this study were to determine the reduction of liver-related complications, including ischemia, necrosis when using (SurG versus the NR). Other key outcomes were if or not SurG reduces post-operative pain as measured by the VAS at different times.
Secondary OutcomesSecondary outcomes assessed the improvement of postoperative recovery, early mobilization, and lower consumption of analgesics. Cosmetic advantages regarding trocar incisions, postoperative complications such as liver lacerations, hematomas, and infections, and the quality of the operative view were also assessed. Lastly, the duration of surgery and duration of hospital stay were compared for both groups.
留言 (0)