
記住我

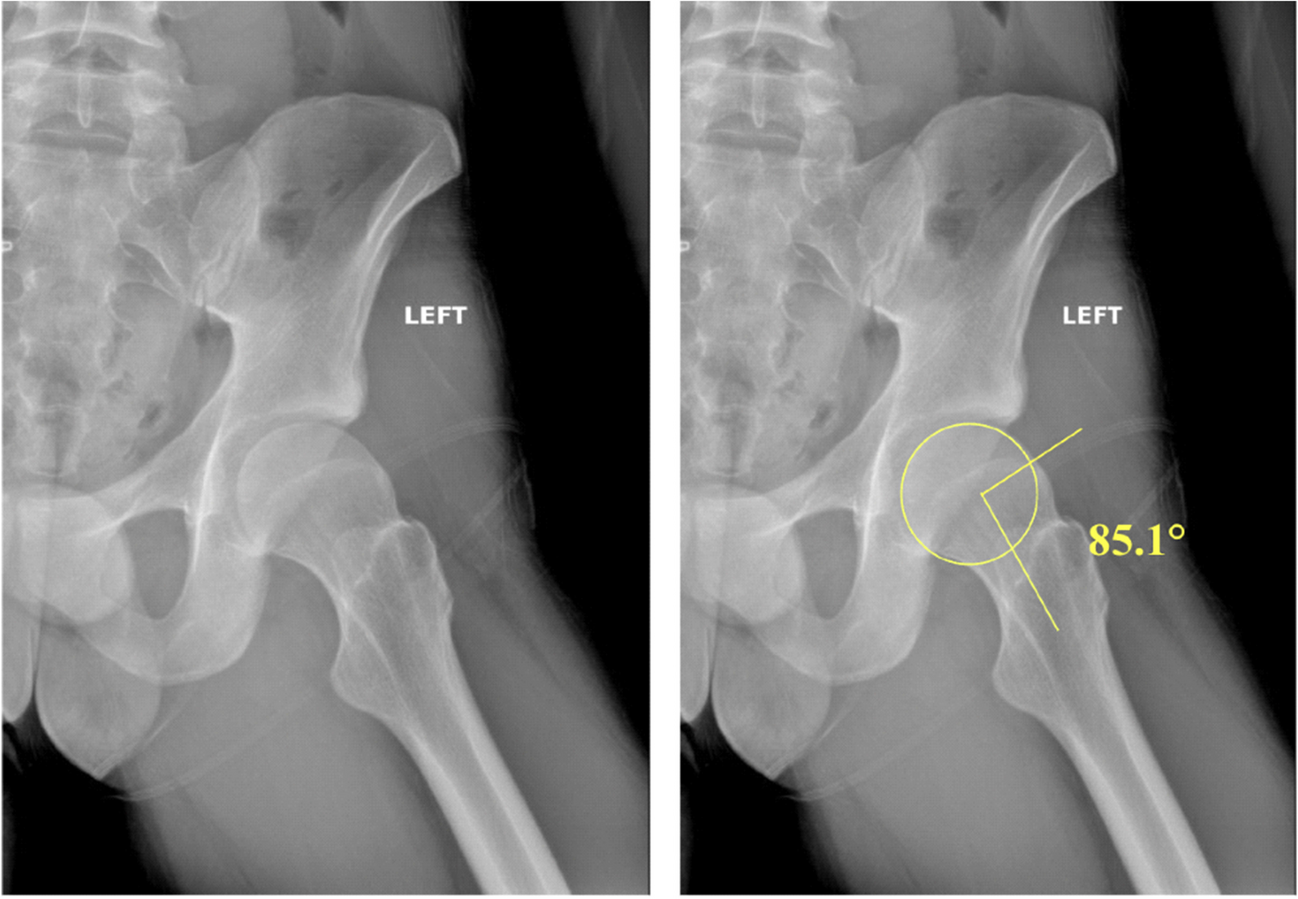

In general, type II SCFs are most commonly treated with CRPP [3]. This consists of a closed reduction under anesthesia followed by percutaneous fixation with smooth Kirschner wires. This allows for correcting the extension deformity, and the pins hold the reduction to minimize re-displacement. Radiographically, the normal alignment of the humerus to the elbow joint can be achieved by re-establishing the anterior humeral line and the Baumann angle (Fig. 4). The anterior humeral line should pass through the capitellum, and the Baumann angle should measure 64–81º [14].
Fig. 4
Illustrates the anterior humeral line (A) and the Baumann angle (B)
Then, a cast is applied. Pins are usually removed in the outpatient setting at 3–4 weeks, during which patients may begin ranging the elbow [2, 3, 15].
The risks of surgical management include anesthetic risks, neurovascular injury caused by the pins, and pin site infection [16]. The risk of a severe complication from anesthesia is less than 1% and includes aspiration, medication reactions, pulmonary complications, the requirement of blood transfusions, postoperative cognitive dysfunction, and postoperative nausea and vomiting [17, 18]. Because of these risks, there is an increase in the use of nerve-block anesthesia and local infiltration anesthesia [19]. Although these risks are small, they can be devastating. In addition to the anesthetic risks of CRPP, pins can also lead to neurovascular injuries. Medial pins with lateral pin start points have an increased risk of ulnar nerve injury, with some studies demonstrating that over half of their ulnar injuries are medial pin placement alone [20, 21]. The rate of pin infection is approximately 1%, and most are reported to be superficial and may be caused by hypergranulation tissue, pin migration, and loosening or bundling of pin tract irritation [22, 23]. Pin site infections are often treated with antibiotics and wound care [24]. Although the risks are minimal and easily treatable, there are rare instances where deep infections can occur, which would necessitate more aggressive therapies, including hospitalization, intravenous antibiotics, and surgical debridement [22].
Indications for Non-Operative ManagementSome type IIa fractures can be treated nonoperatively. In a study by Pierantoni et al., indications for nonoperative management included displacement of 2–15 mm or a 15 – 20º extension on the lateral view and a partially intact posterior cortex, which can maintain reduction without fixation [8]. Similarly, in a study by Spencer et al., indications for nonoperative management of type II fractures included fractures with minimal rotational deformities, no coronal malalignment, and no significant extension of the distal fragment [25].
These fractures typically undergo closed reduction under conscious sedation in the emergency room, followed by long arm casting. A closed reduction maneuver is performed in which a flexion and an anteriorly directed force are exerted on the distal fragment, with an additional posteriorly directed force on the distal humerus if necessary [26]. After reduction, alignment can be confirmed using fluoroscopy. Casting is performed by applying a well-molded long-arm cast to the forearm held in pronation and the elbow flexed at 80–85º [8]. The cast is usually in place for 4–5 weeks to maintain healing and alignment. For patients who may not be able to follow up closely, CRPP should be considered.
The risks of nonoperative management include the inherent risk of sedation, such as respiratory depression, hypotension, allergic reactions, etc. Additionally, while conscious sedation may provide certain benefits, such as a decreased time to manipulation and shorter length of stay, the risk of loss of reduction may be elevated [27]. Therefore, close and frequent follow-up is required to ensure appropriate fracture alignment is maintained.
OutcomesSeveral studies have assessed the outcomes of nonoperative management of type II supracondylar humerus fracture, some of which have estimated that nonoperative management’s failure rate is around 20–25% [27, 28]. A study by Spencer et al. suggested that up to 77% of patients undergo unnecessary surgical procedures [25]. They conducted a retrospective analysis of 259 patients with type II SCF and compared operative and nonoperative outcomes. They found that with appropriate follow-up, those treated nonoperatively had similar outcomes to those with surgical fixation.
Flynn’s criteria is a widely used tool to assess functional outcomes of supracondylar humeral fracture, combining range of motion and cosmetic outcomes such as changes in carrying angles [29]. Perantoni et al. reported excellent outcomes in 8 (25.8%) patients, suitable in 14 (41.9%), fair in 4 (12.9%), and poor in 1 (3.2%) [30]. Other studies reported similar findings, with most functional outcomes being either excellent or good [5, 12, 25]. Another tool utilized in evaluating functional outcomes is the shortened version of the Disabilities of the Arm, Shoulder, and Elbow questionnaire (Quick DASH). The Quick DASH is a self-reported questionnaire comprising 11 items related to various symptoms and activities of daily living that patients may experience [30]. Scores range from 0 (most minor disability) to 100 (most disability). Pierantoni et al. reported Quick DASH scores of 22.4 at cast removal (range: 19–40) and 2.3 (range: 0–9) at the last follow-up visit (P < 0.001) in patients without secondary displacement [30].
Risk Factors for Failure of Nonoperative ManagementSeveral studies have investigated risk factors associated with increased rates of failure of conservative treatment to help stratify which patients may benefit from operative management. Spencer et al. found that initial rotational deformity, coronal malalignment, and significant extension of the distal fragment are associated with an increased rate of nonoperative treatment failure [27]. Fitzgibbons et al. reported similar discoveries, finding that a more substantial extension of the distal humeral fragment at the time of injury was associated with increased failure rates [31]. Additionally, Ojeaga et al. reported that lower humerocondylar angles at presentation and failure to recreate the distal humerus “hourglass” and perpendicular distance from the anterior humeral line to the capitellum were associated with increased rates of failure [2]. Lastly, patients who may have issues with cast immobilization and adherence to restrictions, such as behavioral issues or developmental delay, may be at risk for failure with nonoperative management. [32]
ComplicationsSome of the most feared complications associated with nonoperative management of Gartland type II fractures are compartment syndrome and Volkmann’s ischemic contractures. Early studies strongly opposed closed reduction and casting as an acceptable treatment modality for Gartland type II fractures, as an early case series showed high Volkmann ischemic contractures and cubitus varus deformities [30, 33]. However, more recent studies estimate the rate of compartment syndrome or Volkmann’s ischemia to be < 1% [30]. Other potential complications include loss of reduction, fishtail deformity of the distal humerus, cubitus valgus, cubitus varus, and anterior interosseous nerve palsy [2, 5, 27, 30]. Malunions may require subsequent surgical management, consisting of a distal humerus osteotomy [34]. Indications of distal humerus osteotomy include pain or functional limitations after fracture healing and skeletal maturity [34].
留言 (0)