This study investigated the 30-day clinical outcomes and incidence of HALT in patients undergoing TAVI with the NAVITOR system. The results indicated high feasibility and safety of the NAVITOR system, as evidenced by the high rate of technical success, procedural success, device success, and early safety. The rate of permanent pacemaker implantation was as low as 3%, whereas the high incidence of HALT was observed 30 days after the procedure.
The need for pacemaker implantation after TAVI varies significantly based on the device type and the patient background, with reported rates ranging from 2 to 36% [13, 14]. The rate of pacemaker implantation after the procedure has been reported between 14.7 and 26.7% in the self-expanding Evolut™ (Medtronic, Minneapolis, MN, USA) series [15]. In our study, the rate of pacemaker implantation was lower than that reported in previous studies utilising the NAVITOR system [5, 6, 16]. One reason contributing to this lower rate could be the absence of a right bundle branch block in pre-TAVI assessments, indicating a lower baseline risk [17]. Although the length of the MS is a risk factor for pacemaker implantation, our study found no significant difference in MS length compared to other studies [18]. The reduced pacemaker implantation rate might be attributed to preoperative evaluations of MS length and subsequent adjustments to implantation position based on these measurements. In this study, the high positioning of the valve was targeted without using the distal opening method. The distal opening method involves initiating valve expansion deeper within the left ventricle (7–8 mm), partially opening the valve, and then pulling the entire device to the target depth (3–5 mm). Once optimal positioning and sufficient valve expansion are achieved, the position is maintained, and valve deployment is completed. Instead of this approach, the conventional cusp-overlap method was employed, achieving a mean implant depth of 3.1 mm at the non-coronary cusp. This successful high positioning likely contributed to avoiding the need for pacemaker implantation [7, 19]. The mean length of MS exceeded the implant depth of the non-coronary cusp (1.75 ± 2.0 mm), and successful placement above the MS length was achieved in 27 (84.5%) patients. Particular attention must be paid to preventing non-uniform expansion during the implantation of self-expanding valves. To prevent this, we first assess whether non-uniform expansion is occurring. Prior to full valve release, multi-directional fluoroscopic evaluation is performed to detect under-expansion. If non-uniform expansion is identified, the initial step is to consider recapturing and redeploying the valve, or replacing it with a new one. Additional pre-dilation with a larger balloon is then considered. Finally, following valve deployment, balloon post-dilation is evaluated. In our study, two (6.2%) of the 14 patients who underwent recapture were due to the assessment of non-uniform expansion.
Previous studies have reported that the PORTICO valve, the predecessor of the NAVITOR, achieves a sufficient valve effective orifice area with a minimal valve gradient compared to other commercially available valves [5]. The large, open cells and intra-annular design of the PORTICO valve stent frame contribute to increased haemodynamic stability during deployment and improved access to the coronary arteries post-deployment. These features have been retained in the NAVITOR valve, along with an active outer fabric cuff designed to reduce the risk of PVL by ensuring close integration with the native valve [4]. In this study, echocardiography at 30 days post-TAVI showed no moderate or severe aortic regurgitation due to PVL, with most instances classified as none or trivial, indicating favourable outcomes. These results are comparable to those seen with self-expanding valves with a supra-annular leaflet position and balloon-expandable valves [5, 16]. In addition, minimal pressure gradients and adequate valve expansion were observed in most patients, aligning with previous NAVITOR studies. These results suggest performance comparable to self-expanding valves with supra-annular leaflets, with numerically superior outcomes when compared to balloon-expandable valves.
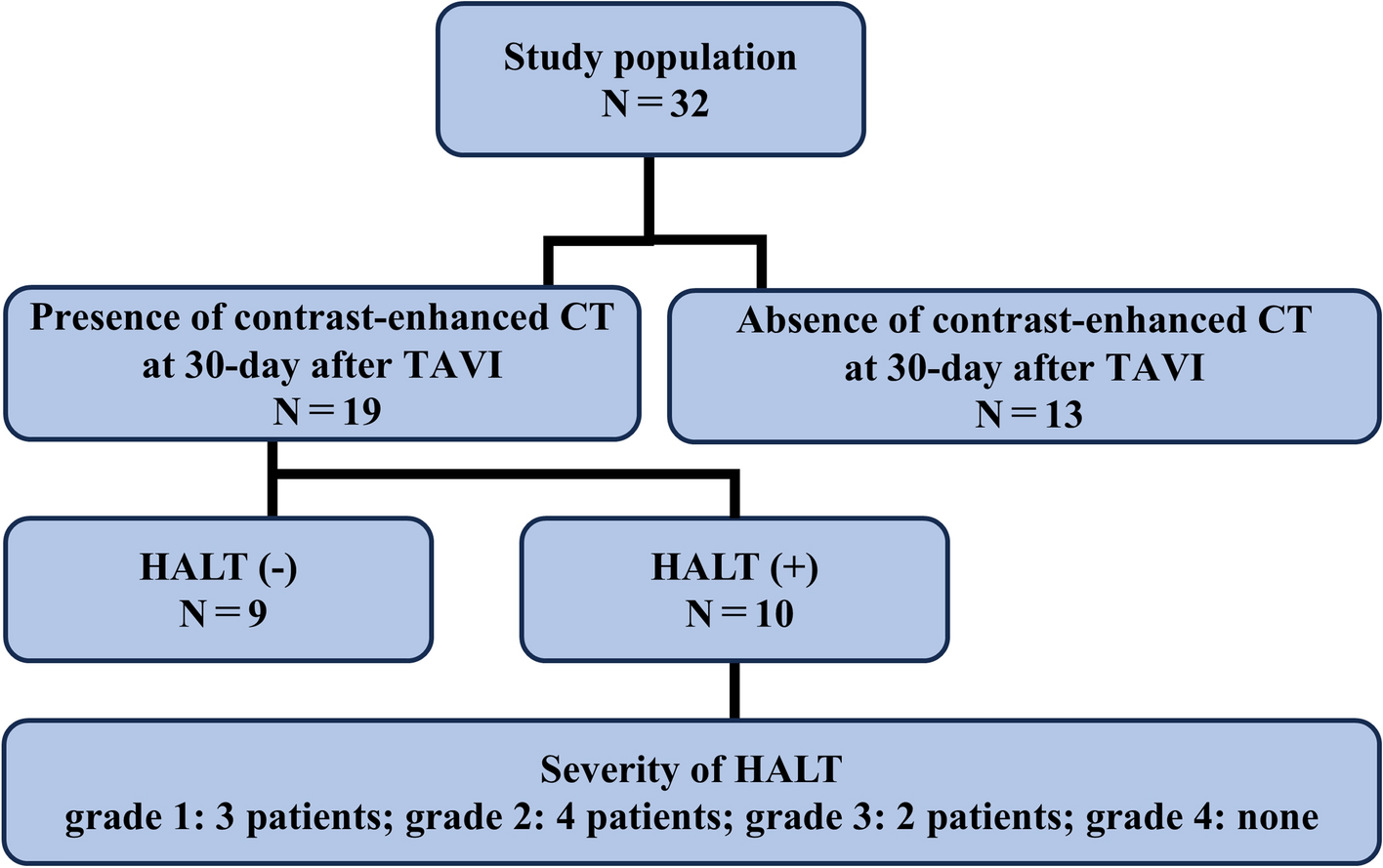
In this study, follow-up contrast-enhanced CT was performed on 19 (59%) patients at 30 days post-TAVI, detecting HALT in 10 (52.6%) patients. Notably, this incidence was higher compared to previous reports, where HALT rates, depending on device type and patient characteristics, ranged from 7 to 15% [20, 21]. Previous studies have demonstrated that transcatheter prosthetic leaflets undergo significant stress and microtrauma during both valve delivery and deployment [11]. First, the TAVI prosthesis undergoes crimping for delivery through a small arterial sheath, which may result in irregular leaflet surfaces, microfilament damage, and reduced integrity of the pericardial leaflets [22]. In addition, valve leaflets are exposed to further damage during ballooning through direct trauma from forceful valve expansion [23]. In this study, HALT was observed in two cases that required post-dilatation with balloon aortic valvuloplasty. For repositionable valves, the process of recapturing may also lead to leaflet abrasions and further damage. In this study, the group with HALT had fewer recaptures than the group without HALT, indicating that recapture was not a significant contributing factor. Recent studies have revealed that the development of HALT is associated with neo-sinus [24]. The deployment of the TAVI prosthesis creates two distinct periprosthetic spaces: the native aortic sinus and the neo-sinus, defined as the space between the prosthesis frame and its leaflets. In vitro flow modelling comparing intra-annular valves to supra-annular valves showed that intra-annular valves tend to have larger neo-sinuses and areas of flow stagnation, particularly at the base of the prosthesis leaflets, where HALT typically forms. Previous studies evaluating HALT on CT scans 30 days post-TAVI have shown that intra-annular balloon-expandable valves exhibit a higher incidence of HALT than supra-annular self-expanding valves [20]. Therefore, the intra-annular valve design of the NAVITOR valve may contribute to a higher incidence of HALT. One of the key innovations in the NAVITOR valve, compared to the Portico valve, is the NaviSeal cuff, which encases the lower outer portion of the valve to mitigate PVL. The NaviSeal is engineered to flexibly adapt to cardiac motion and leaflet movement, effectively reducing PVL. However, it may be prone to deformation when subjected to calcific pressure, which could restrict leaflet motion and potentially contribute to the development of HALT. Although these novel findings suggest the significance of fluid haemodynamics in HALT pathogenesis, further validation in larger and more diverse cohorts is necessary.
Comorbidities, including advanced age, cancer, chronic kidney disease, diabetes, and inflammatory conditions, are associated with hypercoagulability [25, 26]. Whether a more aggressive antithrombotic strategy can reduce the incidence of HALT is currently a topic of ongoing debate. Recent guidelines recommend the selective use of oral anticoagulants for patients with confirmed HALT and elevated gradients (Class IIa recommendation, Level of Evidence B) [3]. In this study, all cases of HALT were asymptomatic, with no events such as stroke, transient ischaemic attack, or myocardial infarction occurring within 30 days post-procedure, classifying these cases as subclinical leaflet thrombosis. Haemodynamic assessment through echocardiography 30 days post-TAVI showed that patients with HALT achieved a sufficient effective orifice area index, and no cases of moderate or severe aortic regurgitation were observed. Although HALT can sometimes regress spontaneously, it has been reported to increase in many cases [26]. Previous studies have suggested that HALT does not affect valve haemodynamics up to 1 year post-procedure; however, the long-term significance remains unclear [20]. Therefore, careful monitoring for subclinical valve thrombosis via echocardiography is recommended, and contrast-enhanced CT scans should be performed during follow-up when feasible.
This study has several limitations. First, the small sample size was small, which may affect the generalizability of the findings. Second, the study utilised only a single device, limiting comparisons with other TAVI systems. Third, in this study, implant depth was assessed by 2D angiography whereas MS length was determined by 3D CT. Post-TAVI CT would likely provide a more accurate and reproducible analysis of the relationship between MS length and implant depth. However, since CT imaging was not performed in all cases following TAVI, its accuracy has not been fully assessed. Fourth, since CT scans were not performed in all patients after TAVI, there is a possibility that selection bias may have occurred.
Finally, the follow-up period was relatively short, which may not capture long-term outcomes and complications. Future studies should aim to increase the sample size, compare different devices, and extend the follow-up periods.







留言 (0)