Detection of cerebellar injury in neonates, particularly premature babies who are more vulnerable, is a key imperative because of its potentially adverse neurodevelopmental consequences [21]. Early and precise identification of cerebellar hemorrhage is helpful for diagnosis and treatment plans. The overall incidence of cerebellar hemorrhage in our study population was 7.32% according to the brain MRIs at term equivalent age, and the incidence showed an inverse correlation with birth weight and GA. Our study included preterm and full-term neonates admitted to the NICU. Therefore, the lower incidence of cerebellar hemorrhage, compared to prior studies that exclusively focused on preterm neonates [1,2,3, 13], may be attributed to differences in the target population.
In our study, cerebellar hemorrhage occurred more frequently in preterm infants and those with lower birth weight. Moreover, in more than half (58.9%) of the cases, the cerebellar hemorrhages were accompanied by supratentorial abnormalities. Such predilections have also been demonstrated in several previous reports [6, 9]. Therefore, it is important to keep in mind that extremely preterm infants, low birth weight infants, or infants with supratentorial abnormalities are at risk of developing cerebellar hemorrhage and should be carefully evaluated with cranial US.
Previous studies evaluating the impact of cerebellar hemorrhage on neurodevelopmental outcomes have used a broad categorization of cerebellar hemorrhage location as either unilateral or bilateral involvement of a hemisphere and/or the vermis, and have consistently reported that larger, bilateral lesions and broader distribution were associated with poorer outcomes [10, 19, 20, 22]. A summary of previous studies [5, 9, 11, 18, 19] and this study is listed in Table 3. However, such broad categorization is too simple and does not reflect the radiologic involvement patterns of cerebellar hemorrhage.
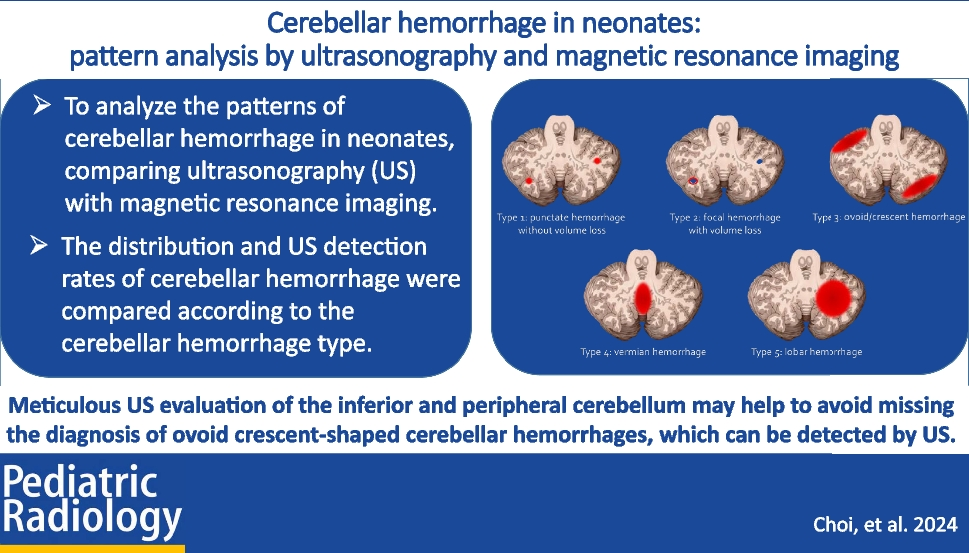
Table 3 The summary of previous studies of cerebellar hemorrhage in neonates and this studyWe classified the type of cerebellar hemorrhage into five categories based on the anatomical and pathological considerations, in addition to the MRI findings, reflecting the size and distribution of lesions. The main blood supply to the developing cerebellum is provided by the posterior inferior cerebellar artery, contributing to the higher prevalence of cerebellar hemorrhages in the inferior regions [18, 23] (especially types 3 and 4 in our classification). The external granular layer, the germinal matrix of the cerebellum, is located in the periphery of the cerebellum, making it prone to bleed in the peripheral cerebellum [13, 14] (as observed in types 1 and 3 in our classification). Furthermore, this classification reflects the size and extent of the hemorrhage, with smaller hemorrhages without volume loss are more likely to be missed but clinically insignificant, while larger lesions with a higher potential for sequelae are more readily detected.
Our new classification scheme of cerebellar hemorrhage showed an inverse correlation with birth weight and GA. In addition, the US detection rates showed a consistently increasing trend from type 1 through type 5 cerebellar hemorrhage. The detection rate of type 1 cerebellar hemorrhage was <5% while that of higher grades was ≥ 75%. We look forward to evaluating the clinical impact of our classification scheme in the future.
While the cranial US is commonly used for routine screening and follow-up of the neonatal brain, our results showed that its detection rate for cerebellar hemorrhage is far inferior to that of brain MRI. Particularly for small cerebellar hemorrhages, such as types 1 and 2 in our study, only 1 out of the 38 cases was initially detected, and 2 additional cases were detected in retrospective image review. Previous studies by Boswinkel et al. [19] and Brossard-Racine and Limperopoulos [10] have suggested that small cerebellar hemorrhages are clinically less significant. In our study, type 1 cerebellar hemorrhage, which was very challenging to detect by US, would have had little clinical impact based on the prior studies. On the contrary, type 3 cerebellar hemorrhage, the second most common type (21.4%) in our study, involves larger areas than types 1 and 2 and thus has greater clinical significance [10, 18, 19]. However, our study revealed that type 3 cerebellar hemorrhages were most frequently overlooked in the initial reports of the cranial US, with the most substantial improvement observed during retrospective review (only 4 cases were reported on the formal radiology reports, while 5 additional cases were identified during the retrospective review). This underscores the significance of prior knowledge regarding the US imaging features of cerebellar hemorrhages. In all cases of type 3 cerebellar hemorrhage, the lesion was located in the peripheral cerebellar hemisphere, predominantly in the inferior part. This positional predilection is in line with previous studies [18, 23, 24], and may be associated with the location of the germinal matrix of the cerebellum. The external granular layer, the germinal zone of the cerebellum located in the peripheral cerebellar hemisphere, is particularly vulnerable to hemorrhage. Notably, even higher vulnerability of the inferior and posterior area of cerebellar external granular layer is attributed to a combination of developmental and vascular factors: the anterior-to-posterior progression of external granular layer maturation, which results in delayed maturation of the posterior cerebellum; the late expression of Math-1 in the posterior cerebellum, which prolongs its immature, proliferative state; and the relatively fragile blood supply from the posterior inferior cerebellar artery, where instability in blood flow regulation may more easily disrupt the posterior and inferior cerebellum due to this vessel’s later maturation [18, 23, 25, 26]. Our study suggests a need for a more careful examination of the peripheral and inferior parts of the cerebellum to improve the detection of type 3 cerebellar hemorrhage.
Some limitations of this study should be acknowledged such as the small sample size and the retrospective design. Furthermore, on retrospective review of US images, it was not clear whether the small hemorrhages were truly not visible on US or were simply not captured in the image. Additionally, the time interval between the US and MRI may have led to imaging in different stages of hemorrhage, including instances of new development or disappearance. The inherent heterogeneity in US images, due to the use of different machines and operators throughout the study period, along with unavoidable factors such as portable examination conditions, operator skills, and patient-specific acoustic windows, may have also affected the accuracy of lesion detection.
In this study, we introduced a new classification of cerebellar hemorrhage based on the MRI findings. The detection rates of cerebellar hemorrhages on US vary consistently across the types of cerebellar hemorrhage. Small type 1 cerebellar hemorrhages were generally not discernible on US. To avoid missing cerebellar hemorrhage on US, preterm infants, low birth weight infants, or infants with supratentorial abnormalities should be more carefully evaluated and the peripheral and inferior parts of the cerebellum should be scrutinized in order not to miss the type 3 cerebellar hemorrhage.







留言 (0)