
記住我
Quantitative abnormalities refer to variations in the level of motor activity. They can be further classified into underactivity and overactivity. Underactivity includes retardation, obsessive slowness, and stupor. Retardation refers to slowness in the initiation, execution, and completion of actions. Obsessive slowness is characterized by slowness secondary to repeated doubts and compulsive rituals. Stupor is a state of markedly slowed motor activity, often to the point of immobility and seeming unawareness of surroundings.
Overactivity includes hyperactivity and agitation. Hyperactivity is characterized by increased motor activity numerous and quick movements and gestures, but with a specific purpose. Agitation refers to excessive motor activity and restlessness without a specific purpose. It may manifest as drumming the fingers, rubbing the hands, getting up and sitting down nonstop, or scratching the head.
Qualitative abnormalitiesQualitative abnormalities involve specific patterns of motor behavior and can be further categorized into catatonic, noncatatonic, and other abnormalities. Catatonic abnormalities are characterized by a range of motor symptoms and can be assessed using the Diagnostic and Statistical Manual (DSM) criteria.[3] DSM-5 notes 12 symptoms out of which three are required for diagnosis. The MEEPE mnemonic may be used to remember the symptoms [Supplementary Table 1].[3] However, there are several other symptoms of catatonia which can be named non-DSM symptoms. These non-DSM symptoms are described according to the Bush-Francis scale [Supplementary Table 2].[4]
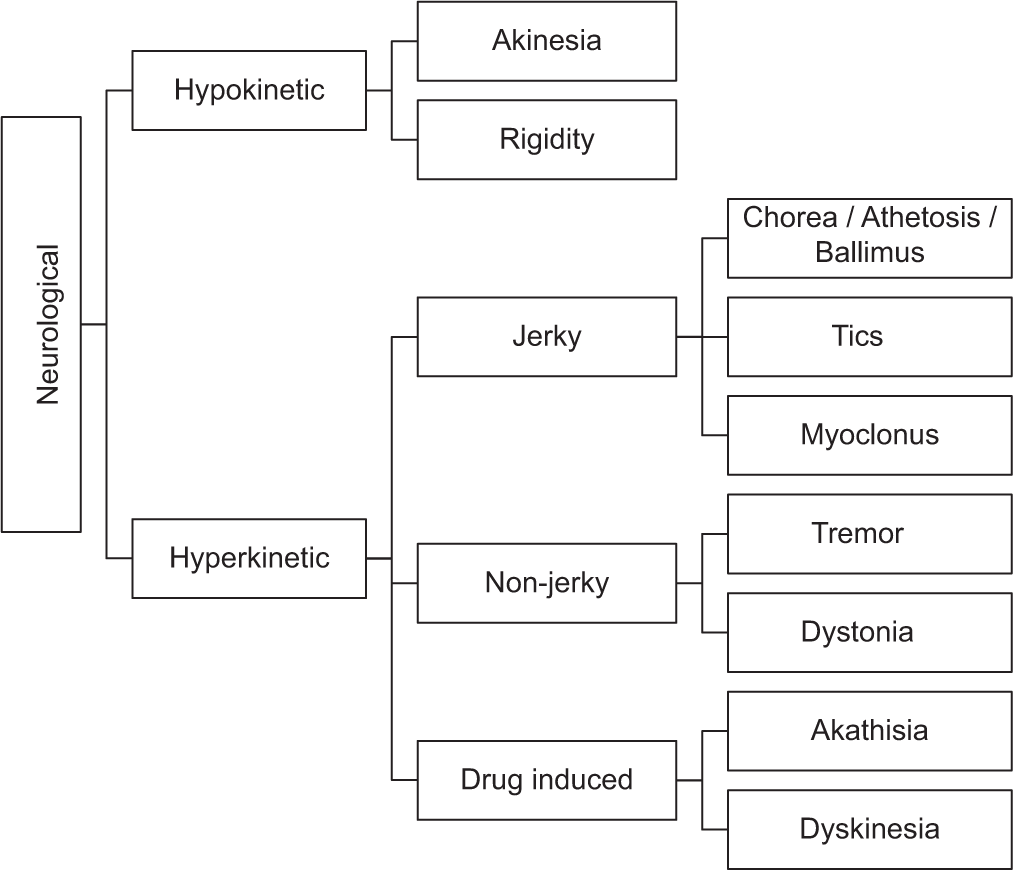
Apart from catatonic abnormalities, there are other motor abnormalities that can be observed in psychiatric practice. These abnormalities have a neurological basis and can be classified into hypokinetic and hyperkinetic categories [Figure 2].[5] Hypokinetic abnormalities are characterized by reduced movement and include symptoms such as bradykinesia, rigidity, postural instability (seen in parkinsonism), and apraxia [Supplementary Table 3].[5]
Export to PPT
Hyperkinetic abnormalities involve excessive and abnormal movements and are further clinically differentiated as jerky or non-jerky.[6] Hyperkinetic abnormalities include symptoms such as tremors, chorea/athetosis/ballismus, tics, dystonia, myoclonus, akathisia, dyskinesia, and ataxia [Supplementary Table 4].[5,7]
In addition to the above categories, there are motor abnormalities that are related to sleep disorders and epilepsy. Sleep-related motor abnormalities can manifest as dyssomnias or parasomnias [Supplementary Table 5].[8,9] Dyssomnias are a broad category of sleep disorders that involve difficulties with falling asleep, staying asleep, or excessive sleepiness. Parasomnias are a category of sleep disorders that involve abnormal behaviors, movements, emotions, perceptions, or dreams that occur during sleep or the transition between wakefulness and sleep. Whereas motor abnormalities are not pathognomonic of epilepsy, several motor symptoms can be associated with epilepsy. Depending on the specific seizure type, these abnormalities can present as various types of motor movements [Supplementary Table 6].[10-12] Astasia-abasia is an inability to stand or walk normally, even though normal leg movements can be performed in a sitting or lying down position. The gait is bizarre and does not suggest a specific organic lesion as seen in conversion disorder. La-belle indifference refers to a lack of psychological distress or concern about physical symptoms or disabilities, even when they are significant.
留言 (0)