
記住我








A comprehensive, stepwise approach was undertaken to integrate systematic literature review findings and expert opinion to develop a comprehensive brain biopsy scoring tool through stages of “Item generation”, “Item reduction” and “Tool development”. The scoring tool was subsequently utilized in standardized evaluation of brain biopsies in cases of Sv-cPACNS.
Histopathological scoring tool developmentLiterature review, expert panel creation and item generation (Fig. 1)Fig. 1
Histopathological brain biopsy scoring tool development for small vessel childhood primary angiitis of CNS (sv-cPACNS)
An exhaustive literature review was conducted via PubMed/ MEDLINE based on the following key terms: “central nervous system vasculitis”, “demyelinating autoimmune diseases”, “multiple sclerosis”, “neuromyelitis optica”, “acute hemorrhagic leukoencephalitis”, “transverse myelitis”, “acute disseminated encephalomyelitis”, “neurosarcoidosis”, “Rasmussen encephalitis”, “hemophagocytic lymphohistiocytosis”, “Limbic encephalitis”, “Autoimmune encephalitis”, “anti NMDAR encephalitis”, “brain biopsy”, “histology” or “histocytochemistry” or “immunohistochemistry”. The initial tool consisted of 56 variables derived from published literature in both adult and pediatric cohorts. This preliminary tool was distributed to a panel of nine expert neuropathologists across Canada for evaluation and feedback.
Expert panel consensus meeting, tool development and item reduction (Fig. 1)Following the initial round of literature reviews, a consensus meeting was held in Ottawa, Canada at the Children’s Hospital of Eastern Ontario. The expert panel discussions led to the truncation and revision of items, modification of the tool design to enhance scoring efficiency and feasibility, and the development of biopsy and feature-specific definitions. It was recommended that each case and control slide deck include a full set of standardized stains, such as Hematoxylin & Eosin (H&E) and immunohistochemistry (IHC) (Fig. 2). Suggested antibody panels included markers like anti-CD3, anti-CD4, anti-CD8, anti-CD20, and anti-CD68, which were chosen to identify various immune cell subsets. Severity definitions were also clarified: mild inflammation was described as scattered lymphocytes, moderate as more extensive but not vessel-obliterating inflammation, and severe as inflammation leading to vessel wall obliteration (Brain Biopsy Scoring Tool- Supplementary material) (See results section, tool development). Following the consensus meeting, adjustments were made and agreed upon by the panel members. Once finalized, the tool was locked to ensure consistency in evaluations across cases.
Fig. 2
Histopathological Brain biopsy scoring application on cases of small vessel childhood primary angiitis of CNS (sv-cPACNS) and inflammatory brain diseases (IBrainD) and epilepsy controls
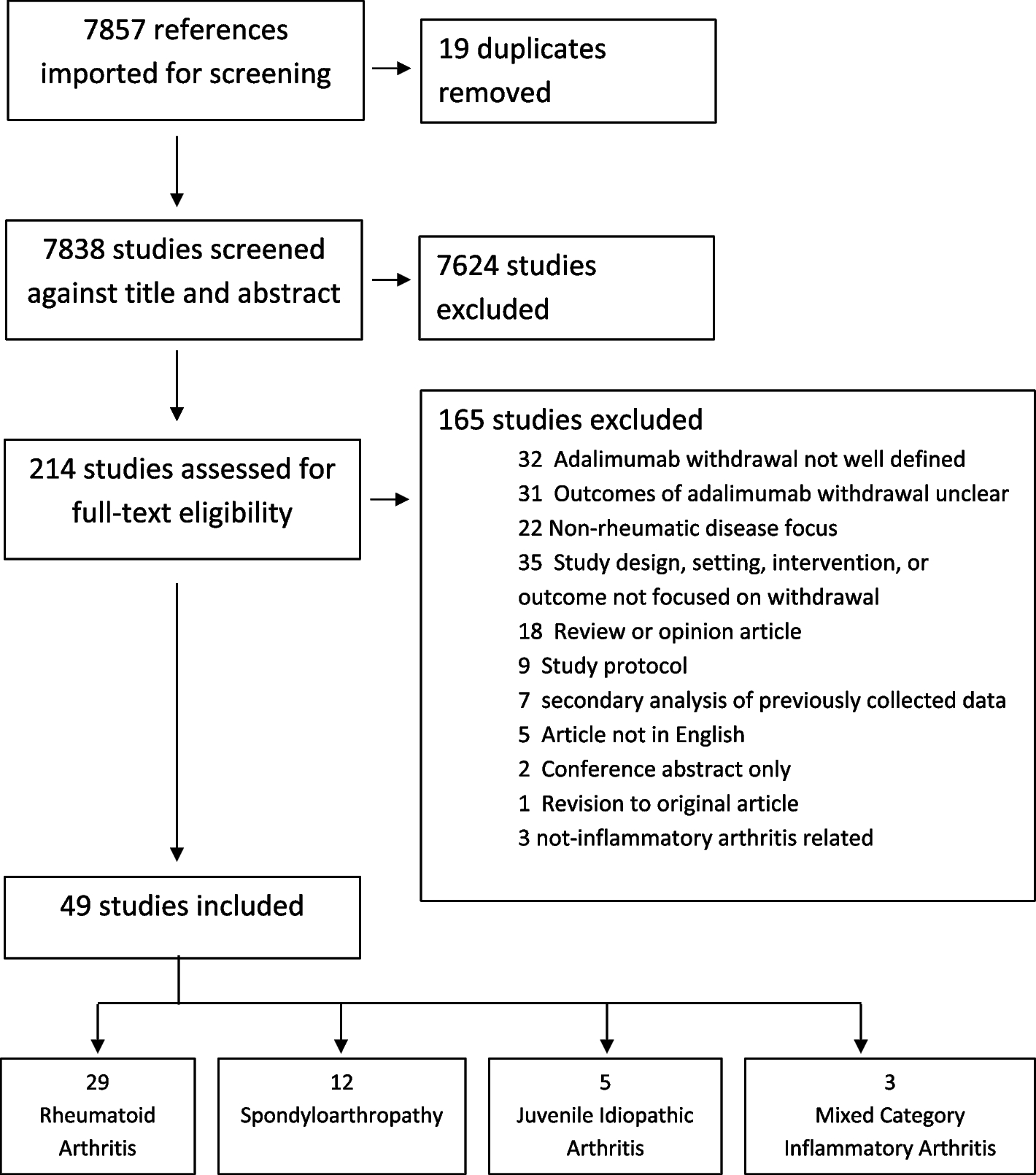
Tool application and validation (Fig. 2)Cases and controls were meticulously de-identified and assigned unique study IDs to maintain confidentiality. These cases were then randomly distributed between two neuropathologists, who independently evaluated them without knowledge of case-control status, or the evaluations performed by the other reviewer, ensuring an unbiased assessment. Regarding specimen processing, pre-existing slides were utilized in the study, specifically chosen from a standard selection of stained and archived materials. In general H&E stains and IHC stains specific to inflammatory cell markers (e.g., CD3, CD20) were included to provide a comprehensive view of inflammatory and cellular characteristics. Slides were scanned, and images were distributed on DVDs for review. Data were entered into the finalized tool called “brain biopsy scoring tool” that was developed based on final expert consensus panel (Fig. 1). All study data were managed using the secure, web-based REDCap system, which ensured standardized data capture and analysis across multiple sites [15]. Reviewers had access only to their assigned cases and were blinded to other evaluations.
Patients and controlsPatients and controls were identified from a single-center prospective cohort of children under 18 years of age at Hospital for Sick Children between 1998 and 2014. Cases consisted of small vessel vasculitis patients diagnosed based on Calabrese criteria [6] of newly acquired neurologic deficits with no evidence of underlying systemic illness and negative angiography findings enrolled in the Brainworks CNS vasculitis registry; Controls were selected from two pools: (a) epilepsy patients who underwent surgery (b) patients with various inflammatory brain disorder that underwent brain biopsy to avoid diagnostic odyssey such as N-methyl-D-aspartate receptor (NMDAR), Rasmussen’s encephalitis, secondary Hemophagocytic lymphohistiocytosis (HLH), Febrile infection-related epilepsy syndrome (FIRES), Tuberculosis infection and Acute necrotizing encephalopathy of childhood. Only those whose brain biopsy was completed and available for cases and controls for review on-site at SickKids were included in the study.
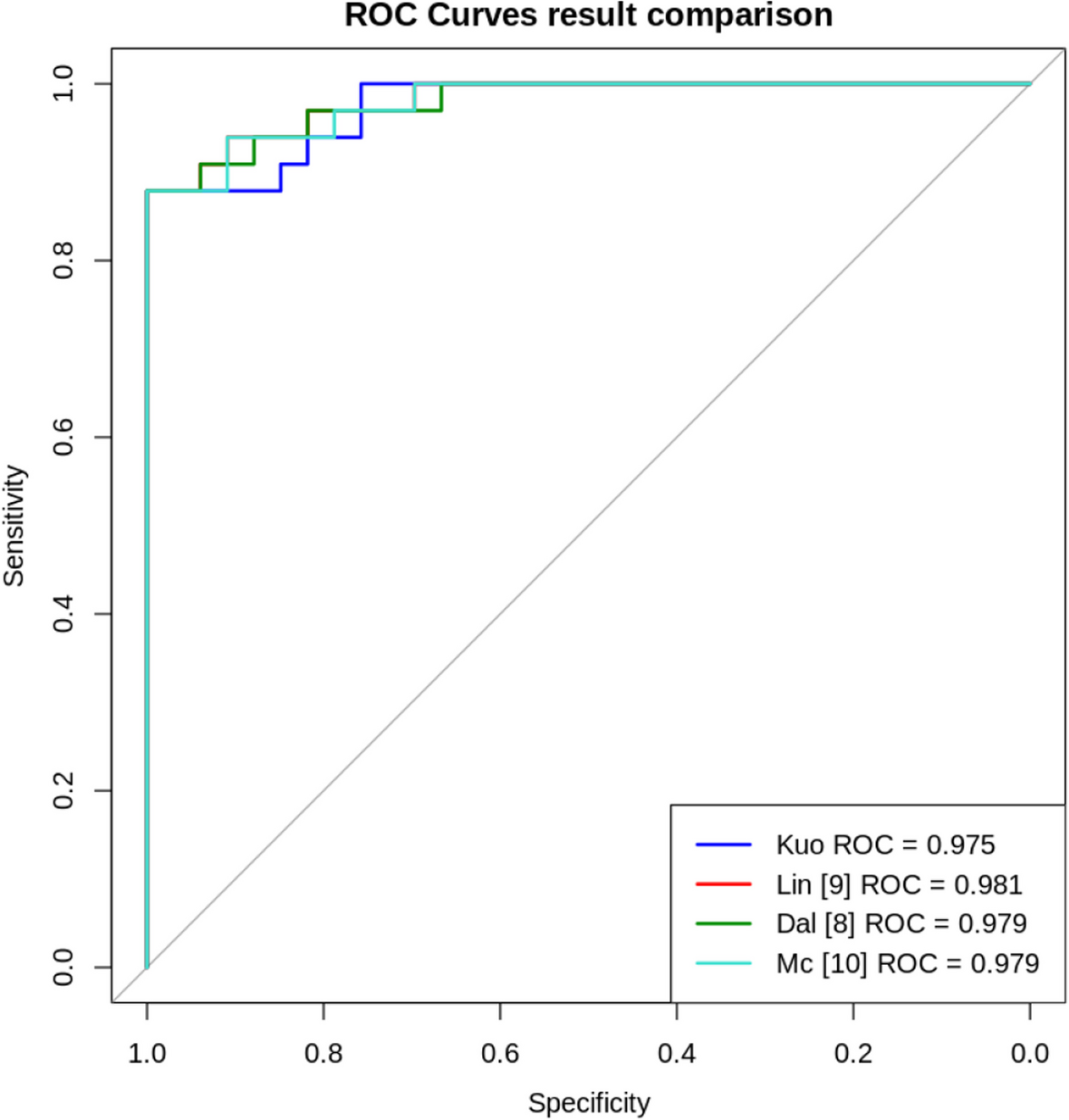
Statistical analysisDescriptive summary statistics were performed, including means with SD, medians with IQR for continuous variables, and percentages for categorical variables. Univariate analyses, such as the student’s t-test, Chi-square, or Fisher’s exact test, were used to compare variables between groups. Multivariable logistic models were employed to investigate associations between histological variables and sv-cPACNS diagnosis. Variable reduction was conducted based on hypothesis-driven univariate analysis before multinomial logistic regression. Odds ratios (OR) from logistic regression measured the association strength between histological characteristics and diagnostic categories, using the control group (Epilepsy cohort) as reference. Agreement between pathologists was evaluated using the Kappa statistic. Multiple correspondence analysis (CA) assessed multidimensional relationships between histological variables and diagnoses. All analyses were performed using SAS software, V.9.4 (SAS Institute, Cary, NC, USA).
留言 (0)